Drugs Used In Periodontal Therapy
Write short note on local drug delivery system.
Or
Write short note on local drug delivery (LDD).
Or
Write short note on LDD.
Or
Write short answer on local drug delivery.
Answer. Local drug delivery systems are developed due to the limited efficacy of mouthrinsing and irrigation in deep pockets.
“Understanding the role of systemic antibiotics in gum disease treatment”

“Importance of studying systemic antibiotics for better periodontal care”
Main aim of the drug delivery system is to direct antimicrobials to the infection sites and maintaining effective level of drugs for sufficient period of time without producing any major side effects.
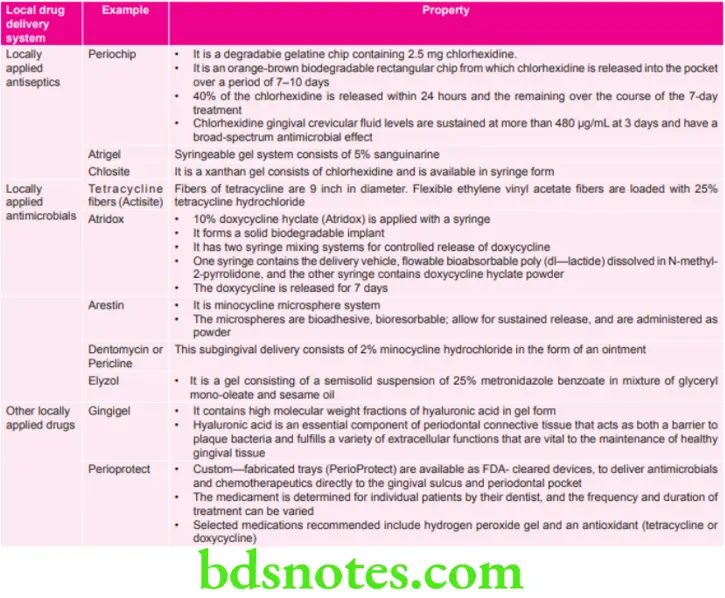
Various Local Drug Delivery Systems Used in Periodontics are:
“Common challenges in using systemic antibiotics effectively”
Local Drug Delivery Indications
- As an adjunct in the treatment of few localized nonresponding sites in an otherwise controlled patient.
- In failing implant cases.
- In medically compromised patients in whom surgical procedures are not recommended.
- In cases with periodontal abscess.
- In cases with periodontal maintenance therapy.
- In patient with gastrointestinal intolerance to systemic drug medication.
“Steps to explain the mechanism of systemic antibiotics in periodontal therapy”
Local Drug Delivery Contraindications
- Patients having history of allergy to any particular antimicrobial agent.
- During pregnancy and lactating periods.
- In the children under the age of 12 years.
- Subjects with complete renal failure.
- Subjects susceptible to infective endocarditis.
“Role of bacterial suppression in systemic antibiotic treatment”
Local Drug Delivery Advantages
- Presence of high concentration of drug in subgingival sites.
- Patient compliance is absent.
- Does not affect symbiotic microflora of gastrointestinal tract.
- Systemic intolerance gets bypassed.
“Early warning signs of improper use of systemic antibiotics”
Local Drug Delivery Disadvantages
- It is difficult to place therapeutic concentrations of the antimicrobial agents in deeper areas.
- Professional application is mandatory, if used manually requires undergo dexterity and patient compliance.
- Complete drug penetration is impossible and extra pocket sites remain unaffected.
Read And Learn More: Periodontics Question And Answers
Leave a Reply