Diseases Of Nervous System
Question.1. Enumerate causes of facial pain.
Answer. Causes of facial pain are:
- Neuritis of cutaneous nerves of face and scalp.
- Arthralgia of temporomandibular joint
- Trigeminal neuralgia.
- Post herpetic neuralgia.
- Temporal arthritis.
- Miscellaneous causes:
“Understanding nervous system diseases through FAQs: Causes, symptoms, and treatments explained”
- Facial neuralgia: It is a form of inflmmation of nerve of face and scalp.
It generally occurs as complication of septic state or due to involvement of neurotrophic virus. The pain is confied to face and scalp. - Arthralgia of TMJ: It is in the form of rheumatic arthritis or ankylosing spondylitis (a chronic progressive inflmmatory disorder unlike other rheumatological disorders) when there is pain and swelling of joint.
- Trigeminal neuralgia: This is a disease seen commonly in middle and elderly individuals and is characterized by attcks of sever pain in distribution of trigeminal nerve and its branches especially in maxillary and mandibular branches.
- Postherpetic neuralgia: Herpes zoster commonly involves the ophthalmic division of 5th nerve,characterized by vesicular eruption on the face.
- Temporal arthritis: It is a form of collagen disorder of unknown etiology which involves mainly the arteries. It occurs in elderly age group.
Patient may complain of pain on the face, jaw,mouth and tongue in distribution of branches of external carotid artery. - Miscellaneous causes: These include lesions of trigeminal nerve in brain stem, *syringobulbia and thrombosis of posterior inferior cerebellar artery.
Tabes dorsalis is another cause of pain coming in attcks over the face.
“How do degenerative disorders affect the nervous system? FAQ answered”
Read And Learn More: General Medicine Question And Answers
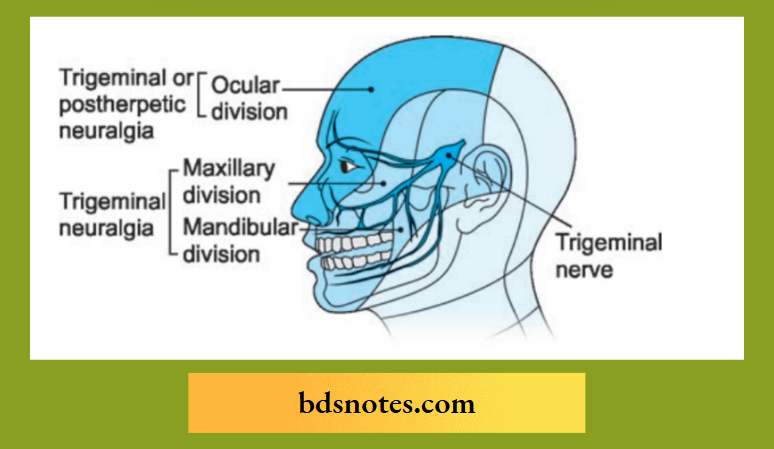
Question.2. Write short note on trigeminal neuralgia.
Answer. Trigeminal Neuralgia is also called as Tic Douloureux.
A disorder characterized by the *paroxysmal attcks of neuralgic pain with affction of one or more division of trigeminal nerve.
The pain involves the third and second divisions equally and rarely the fist.
Trigeminal Neuralgia Clinical Features or Trigeminal Neuralgia Treatment
- Pain is unilateral and is confined to one of the three divisions of nerve. Pain is sharp and onset is sudden. The pain is only of a few seconds.
- During the attcks there is flshing of face, i.e. redness of the face.
- Dilatation of pupil is present.
- There is excessive lacrimation
- After repeated attcks skin becomes shiny and hair in the area becomes gray.
- Sometimes secretion of nasal mucus and saliva may occur in the side of pain.
Trigeminal Neuralgia Etiology
Trigeminal neuralgia is spontaneous and following exposure to cold wind, blow on face, or chewing or eating, drinking hot or cold flid and washing the face.
Trigeminal Neuralgia Management or Trigeminal Neuralgia Treatment
- Elimination of all possible sources of infection.
- Drugs:
- Analgesics: Potent analgesics must be used with caution because of danger of habituation.
- Carbamazepine: 100–200 mg BD a day and increasing the dose to 600–800 mg per day.
- Phenytoin sodium: 0.1 gm TDS when carbamazepine is not tolerated.
- Vitamin B12: 1000 μg IM daily for two weeks.
- Injection ofalcohol: It is given in affcted nerve, or gasserian ganglion.
If more than one division is affcted inject 10 minims of 90% alcohol after local anesthesia with 2–3 drops of procaine. - Microvascular decompression: In this there is separation of blood vessels is done which are in contact with trigeminal nerve roots.
There is also insertion of non absorbable sponge which provide relief of pain in most of the patients. - Radiofrequency thermocoagulation: This procedure is carried out at the trigger spot or site of pain origin which is localized by electric stimulation of needle inserted in trigeminal ganglion and leads to permanent relief.
- Surgery: In this selective or complete preganglionic section of trigeminal root is done.
This technique can lead to disadvantages such as permanent dysesthesiae.
Another bettr technique is percutaneous electrocoagulation of preganglionic rootlets corresponding to trigger zone, the temperature of probe being so regulated as to coagulate small thinly myelinated pain fiers but preserving most heavily myelinated touch fiers.
Trigeminal Neuralgia Treatment
“Importance of studying nervous system diseases for healthcare professionals: Questions explained”
Question.5. Write short note on Migraine.
Answer. Migraine is defied as recurrent attcks of headache varied in intensity frequency and duration and is commonly unilateral in onset and is associated with anorexia and sometimes with nausea and vomiting.

Migraine Clinical Features
- The headache follows and the pain is confied on one side by occasionally it may be bilateral.
- Nausea and vomiting may be present and last for the few hours.
- Light and noise sensitivity is present.
- Fatigue and stress are present in the case.
- There is presence of polyuria.
Simplifid Diagnostic Criteria for Migraine
Repeated attcks of headaches lasting for 4 to 72 hours which have features:
- Normal physical examination
- No other reasonable cause for headache
- At least two of:
- Unilateral pain
- Throbbing pain
- Aggravation of pain by movement
- Moderate or severe intensity
- At least one of:
- Nausea or vomiting
- Photophobia or phonophobia
Migraine Management
Migraine During attack
- Analgesics: NSAIDs, e.g. diclofenac can be given orally or im and is particularly useful when severe vomiting is a feature. Sublingual Piroxicam has significant analgesic effcts in acute migraine without aura with excellent tolerability.
- Ergotamine: Ergotamine tartrate 0.25 to 0.5 mg IM or orally 1–2 mg. tablet preferably in combination with 100 mg caffine –2 tablets at onset followed by l tablet after 30 minutes, if necessary, or Dihydroergotamine 1 mg IM, or 1–2 mg by mouth.
Whichever preparation is used, a high dose often causes nausea and vomiting.
These may be prevented by giving cyclizine 50 mg.or chlorpromazine 25 mg. - 5-HT1 agonists: Sumatriptan 6 mg s.c. gives relief from headache in 60 minutes, with corresponding improvement in nausea, vomiting and photophobia.
Oral dose of 100 mg provides relief within 2 hours.
Headaches recur within 48 hours in litte less than half the patients.
Rizatriptan given orally acts faster than sumatriptan. Zolmitriptan nasal spray 5 mg gives relief in 5 minutes. - General: Lying in a darkened and quiet room and ice pack to the head may help.
“Common challenges in diagnosing and treating nervous system diseases effectively: FAQs provided”
Reducing frequency and severity of subsequent attcks
- Elimination oftrigger factors: Sleeping late, irregular and hurried meals, certain foods, especially chocolate and fried food, or missing of meals, psychological stress,contraceptive pills.
Treatment of cervical spondylosis - Relaxation exercises: They may include biofeedback from a temporalis electromyogram. Yoga, Pranayama.
Drugs:
- Serotonin (5-HT) inhibitors: Calcium antagonists suchas Flunarizine 10 mg/day Or Cyproheptadine 4 mg tds. Or Pizotifen 0.5 mg tds or 1.5 mg nocte.
Or Methysergide 1–2 mg t,d.s. is the most effctive drug in this group, but should be used under supervision in courses not exceeding 3–4 months. - Topiramate: It is an antiepileptic drug used in prophylaxis of migraine, Dose: 2.5 to 5 mg BD
- Divalproex (valproic acid) 200 mg BD
- Tricyciic agents: Amitryptiline 25 mg TDS may be effective irrespective of the presence of depression.
- Ergotamine tartrate: For histamine cephalgia 1 mg by mouth or 0.25 mg by selfadministered injection or by suppository used regularly last thing at night can be continued for many weeks without harmful effcts, 2 days being left without treatment each week.
- Hormones: Progesterone given for last eight days may be useful for migraine occurring in the immediate premenstrual period or at beginning of catamenia.
When migraine begins or becomes worse at the time of menopause, estrin, given in small doses as continuous therapy sometimes helpful.
Schedule:
- Propranolol 40–160 mg/day or Flunarizine 5–10 mg/day as fist line of therapy.
- In patients with episodic and chronic migraine
- Topiramate 50–100 mg/day.
- In patients with episodic migraine Divalproex
250–750 mg/day. - For mixed migraine and tension type headache:
Amitryptiline 10–25 mg/ day.
After 6–12 months of prophylaxis gradual
withdrawal should be considered.
Question.6. Classify headache. Discuss etiology, symptoms, signs,pathogenesis of cluster headache.
Answer.
Classification of Headache
The classifiation is given by International Headache Society,which is as follows:
- Migraine (Classical common, opthalmoplegic and basilarartery)
- Tension type, headache (e.g. episodic or chronic)
- Cluster headache and chronic hemicrania
- Miscellaneous headache not associated with structural lesion (e.g., cold stimulus induced, cough headache,idiopathic, sexual activity induced)
- Traumatic headache
- Headache associated with vascular disorders (e.g. CVA,intracranial hemorrhage or hematoma, arteritis, venoussinus thrombosis and other vascular disorders).
- Hedache associated with nonvascular intracranial diseases(e.g. high or low CSF pressure, intracranial infections orneoplasm).
- Headache associated with substance abuse or their withdrawal.
- Headache associated with systemic infection (e.g. viral and bacterial).
- Headache associated with metabolic diseases (e.g. hypoxia, hypercapnia, hypoglycemia, dialysis, etc.)
- Headache due to referred pain (e.g., disorders of eyes, ear,nose and sinuses, teeth, jaw and temporomandibular joint)
- Cranial neuralgia (e.g., trigeminal, glossopharyngeal or occipital neuralgia).
- Unclassifid headache.
Cluster Headache/Migranous Neuralgia
This is distinctive and treatable vascular headache syndrome which is characterized by one to three short lived attcks of periorbital pain per day over 4 to 8 weeks.
Migranous Neuralgia Etiology
Headache associated with at least one of the following on the painful site namely:
- Conjunctival injection
- Nasal *congestion
- Forehead and facial flshing
- *Miosis
- *Ptosis
- Eyelid edema
- Rhinorrhea.
Migranous Neuralgia Symptoms
- There is periodic, severe and unilateral periorbital pain.
- Reddening of eye is present.
- Nasal *stuffiss is present.
- Nausea is present.
- Pain occur after 1 or 2 hours when patient fallen asleep.
Migranous Neuralgia Signs
- Conjunctiva infection
- Rhinorrhea
- Nasal congestion
- Lacrimation
- Miosis
- Ptosis
- Flushing, sweating
- Edema of face.
“Why is early detection critical for preventing nervous system disease complications? Answered”
Migranous Neuralgia Pathogenesis
Carotid body plays major role in cluster headache.
- Disturbance in some specific areas in hypothalamus due to cyclic cluster periods which causes disturbances in sympathetic and parasympathetic supplies to body.
It causes increase in vasomotor tone which activate peripheral chemoreceptors. - It induces attacks with oxygen desaturation which reaches the threshold level of oxygen causing activation of chemoreceptor and stimulate the nuclei of 7th and 10th cranial nerve in respiratory center.
- It results in stimulation of peripheral secretory and other receptors innervated by the cranial nerves causing cluster headache.
Question.7. Outline the management of Headache.
Answer. The management of headache is as follows:
- Mild headache responds to rest, massage,acetaminophen or listening to relaxing music.
- Moderate headache typically requires NSAID therapy
Caffine helps ameliorate many mild-to-moderate headache. - Antiemetics such as prochlorperazine or metoclopramide helps to relieve moderate to severe headache especially those accompanied by nausea.
Ergotamine and triptan drugs are suited to treating migraine.
Cluster headache often resolves after treatment with corticosteroid or high flw oxygen.
The headache of temporal arteritis also responds to high dose steroids, but these agents must be continued for months or years until syndrome remits.
Question.9. Write short note on Temporal Epilepsy.
Answer. Temporal epilepsy is the form of epilepsy where aura (A subjective, but recognizable sensation that precedes and signals the onset convulsion) is either auditory, visual, olfactory or gustatory.
Temporal Epilepsy Clinical Features
- There is feeling of unusual smell, an emotional feeling or*hallucinations.
- Motor activity stops and patient looks vacant.
- There is unilateral dystonic posturing of the limb.
- There is temporary cessation of the activity followed by lip smoking, chewing movements or the patient may walk aimlessly. When seizure and amnesia is present.
Temporal Epilepsy Management
General:
- Avoid physical exertion, regular habits of eating and sleeping.
- Avoid alcohol.
Pharmacological:
- Clonazepam 1.5 mg/day reduces excitability of neurons.
- Methsuximide 500 mg daily is effctive.
- Clobazam 10 to 20 mg has antiepileptic activity.
- Gabapentin 300 mg TDS is used to control epilepsy.
- Lamotrigine 50 mg daily for two weeks followed by 100 mg/day given in two divided doses for 2 weeks.
- After dose is increased by 100 mg every 1 to 2 weeks till response is obtained.
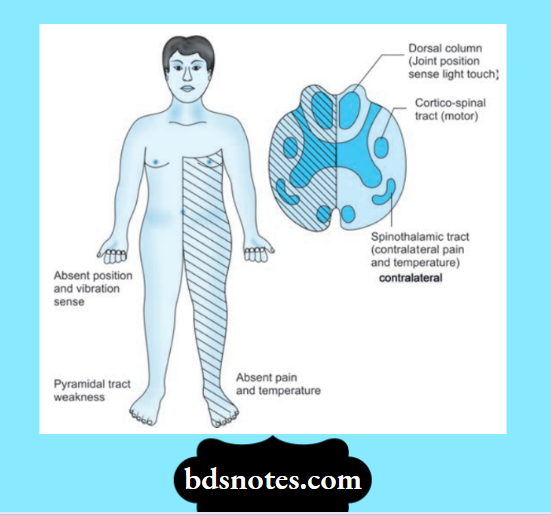
Question.11. Write short note on Brown-Sequard’s syndrome.
Answer. BrownSequard’s syndrome is a spinal cord lesion. In it hemisection (Bisection) of spinal cord is present.
Brown-Sequard’s syndrome Etiology
- Compression of cord
- Intramedullary neoplasm
- Due to *stab in back
- Bullet wounds
- Vertebral fracture and caries
- Vascular causes, i.e. *arachnoiditis.
Brown-Sequard’s syndrome Clinical Features
Below the site of lesion
- Motor changes: Spastic paralysis, i.e.
- Positive Babinski’s sign
- Clasp knife rigidity
- Exaggerated tender jerks and loss of voluntary power. All the above features are seen in unilateral side of lesion. The sign are due to interruption of already crossed pyramidal tract.
- Sensory changes:
- Loss of fie touch, tactile sensation and vibration sense is loss in ipsilateral side. This is due to loss of lemniscal fiers.
- Loss of crude touch, pressure, pain and temperature sense on contralateral side. This is due to loss of spinothalamic tract fier.
At the site of lesion
- Motor changes: Lower motor neuron paralysis is segment corresponding to level of lesion on ipsilateral side, due to loss of anterior horn cells of segment.
- Sensory changes: There is anesthesia or ipsilateral *dermatomes due to loss of posterior root of corresponding spinal cord segment.
“Factors influencing success with nervous system disease knowledge: Q&A”
Question.12. Enumerate the cause of Epilepsy.
Answer. The causes ofepilepsy are:
Follwing are the causes of epilepsy in diffrent age groups.
In neonates (0 to 2 years)
- Perinatal hypoxia, or ischemia
- Birth injury
- Acute infections, i.e., meningitis, encephalitis metabolic d isturbance, i.e hypoglycemia, hypocalcemia,hypomagnesemia structural lesions such as congenital vascular malformations
- Familial or genetic disorders.
In chidren (2 to 12 years)
- Idiopathic
- Acute infections, i.e., meningitis, encephalitis,toxoplasmosis, cerebral abscess
- Head injury or trauma
- Febrile convulsions
In adolescents (12 to 18 years)
- Idiopathic
- Head trauma
- Drugs, i.e., amphetamines, antidepressants, phenothiazines,etc.
- Alcohol withdrawal
- Arteriovenous malformations
- Infections, i.e., meningitis, encephalitis, cerebral abscess,toxoplasmosis
In Person of age 18 to 35 years
- Head injury or trauma
- Alcoholism
- Brain tumors, cysts, hydrocephalus, aneurysms, AV malformations
- Inflammatory disorders such as sarcoidosis, multiple sclerosis, SLE.
In older adults and old Persons
- Brain tumours
- Cerebrovascular accidents (thrombosis, infarction,hemorrhage)
- Alcoholism
- Uremia
- Hepatic encephalopathy
- Hypertensive encephalopathy
- Electrolyte disturbances
- Hypoglycemia
Question.14. Enumerate the etiological factors of Bacterial Meningitis. Describe clinical features, complications and management of a case of meningococcal meningitis.
Answer. Etiology of Bacterial Meningitis
Bacterial meningitis is caused by various bacteria which are as follows:
- In neonates or infants
- Gram negative bacilli, i.e. E. coli and B. proteus
- Group B streptococci
- Listeria monocytogenes
In adolescents or adults
- Streptococcus pneumoniae
- Neisseria meningitidis
- Mycobacterium tuberculosis
- Staphococcus aureus
- Hephilus inflenzae
In old age
- Hemophilus inflenzae
- Neisseria meningitides
- Streptococcus pneumoniae
- Mycobacterium tuberculosis
In immunocompromised
- Listeria monocytogenes
- Gram negative bacilli
- Streptococcus pneumoniae
- Mycobacterium tuberculosis
- Cryptococcus neoformans
Clinical Features Of Meningococcal Meningitis
- Meningococcal rash, petechial rash on skin, mucus membrane and conjunctiva.
- Acute fulminant illness with adrenal insuffiency.
- Hypotension, shock and patient go quickly in comma. This is called as Water house–Friderichsen syndrome.
- It is due to necrosis in adrenal gland during course of meningococcal septicemia.
- Signs of meningeal irritation, i.e. Kernig’s and Brudzinski’s sign are positive.
- In children and adults it is mainly present.
- Neck rigidity
- Vomiting
- Fever with rigor
- Dilatation of pupil.
Complications of Meningococcal Meningitis
- Neurological defect like hemiplegia, aphasia, ocular nateor, hemianopia, blindness and deafness.
- Mental deterioration
- Cerebritis, brain abscess
- Focal fis
- Auditory impairment
- Subdural empyema
- Internal hydrocephalus
- Spinal cord compression due to arachnoiditis.
“Steps to explain nervous system diseases: Causes vs symptoms vs treatment: Q&A guide”
Management of Meningococcal Meningitis
- For adult patients penicillin G 5 to 10 million units IV 6 hourly.
- Cephalosporins, i.e. cefotaxime 2 gm IV or ceftriaxone
2 gm IV OD is also effctive. - Patients allergic to penicillin are treated with chloramphenicol 1 gm IV 6 hourly
- Treatment is continued for 7 to 10 days.
- For raised intracranial tension IV mannitol is given which is accompanied by high doses of dexamethasone 4 mg IV 6 hourly. The supportive treatment is to maintain nutrition, flid and electrolytic balance.
Question.15. Describe the management of tubercular meningitis.
Answer.
Management of Tubercular Meningitis
General management:
- Maintenance of nutrition, hydration and electrolyte balance.
- Case of bowel and bladder
- Nursing should be good
- If there are convulsions, anticonvulsants are given.
Tubercular Meningitis Treatment:
- Antitubercular drugs: Rifampicin 600 mg/day + Isoniazide (600 to 900 mg/day) + Pyrazinamide(1.5 gm) should be given. Treatment with this regimen is given for 2 months.
This is followed by rifampicin 600 mg/day + Isoniazide (600 to 900 mg/day) for 12 to 18 months. - Steroids: Prednisolone 40–60 mg/day to reduce toxicity, piaarachnoid adhesions and felling of wellbeing.
Question.16. Describe clinical features and evaluate management of Meningitis.
Answer.
Meningitis Clinical Features
Meningitis Symptoms
- Fever coming with rigors.
- Headache which is very severe (bursting in character) mainly in frontal region radiating down to back.
- Vomiting
- Convulsion in children
- Malaise
- Severe photophobia
- Ptosis: Due to raised intracranial tension
- Stiffess in neck and back
- Pain in neck
- Impairment of consciousness i.e. confusion, delirium and coma.
Meningitis Signs
- Head retraction is present in infants and children.
- Neck rigidity, i.e. bending of neck causes pain and spasm of neck muscles or it is diffilt to bend the neck.
- Kernig’s sign is positive
- Brudzinski’s sign is also positive if patient is conscious.
- Presence of papilledema
- Presence of cranial nerve palsies
Clinical Features Of Tuberculous Meningitis
Meningitis Symptoms
- Headache
- Vomiting
- Low grade fever
- Lassitude, i.e. weariness or exhaustion
- Depression
- Confusion
- Behavior changes.
Meningitis Signs
- Meningism may be present
- Occulomotor palsies
- Papilledema
- Depression of conscious level
- Focal hemisphere signs.
Management- Cholinesterase inhibitors, i.e. pyridostigmine 30 to 120 mg or neostigmine 15 to 45 mg TDS is given.
- Thymectomy is performed as soon as feasible in any antibody positive patient with symptoms not confied to extraocular muscles.
- Plasma exchange is done
- IV immunoglobin 0.4 gm/kg/day for 5 days is given.
- Immunosuppressant: Azathioprine 2.5 mg/kg body weight
is helpful in reducing dosage of steroids necessary and allows steroids to withdraw.
“Role of infections in causing nervous system diseases: Questions answered”
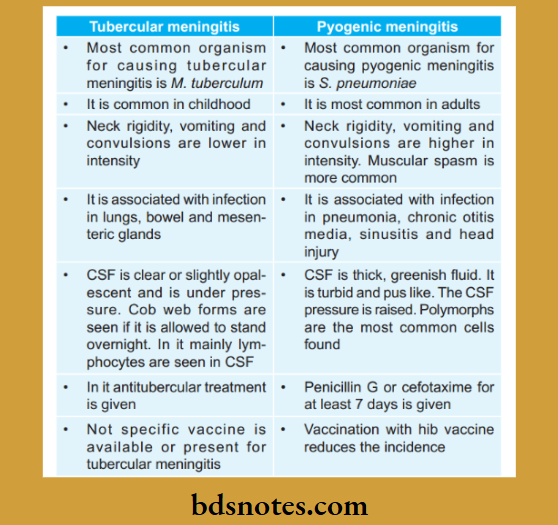
Question.17.Diffrentiate between Tubercular Meningitis and Pyogenic Meningitis.
Answer.
Question.18.Write briefl on Myasthenia Gravis.
Answer. An acquired autoimmune disorder causing skeletal muscle fatigability and weakness which can be present at any age is called as myasthenia gravis.
Myasthenia Gravis Symptoms And Signs
Muscular weakness: There is repetitive contraction with tendency to recovery of motor power after inactivity
- Ocular muscles: The ocular muscles are fist to be involved.
There is presence of double vision or Ptosis. Symptoms are asymmetrical. - Limb weakness: It may involve proximal or distal limbs.
- Bulbar muscle weakness: It leads to the loss of facial expression, inability to whistle, diffilty with speech,chewing and swallowing.
- Respiratory muscle involvement: It leads to shortness of breath and ventilatory failure.
Myasthenia Gravis Management
- Cholinesterase inhibitors, i.e. pyridostigmine 30 to 120 mg or neostigmine 15 to 45 mg TDS is given.
- Thymectomy is performed as soon as feasible in any antibody positive patient with symptoms not confied to extraocular muscles.
- Plasma exchange is done
- IV immunoglobin 0.4 gm/kg/day for 5 days is given.
- Immunosuppressant: Azathioprine 2.5 mg/kg body weight is helpful in reducing dosage of steroids necessary and allows steroids to withdraw.
Question.19. Describe the clinical and diagnostic features of Tberculous Meningitis.
Answer.
Tberculous Meningitis Clinical Features
Tberculous Meningitis Symptoms
- Fever coming with rigors.
- Headache which is very severe (bursting in character) mainly in frontal region radiating down to back.
- Vomiting
- Convulsion in children
- Malaise
- Severe photophobia
- Ptosis: Due to raised intracranial tension
- Stiffess in neck and back
- Pain in neck
- Impairment of consciousness i.e. confusion, delirium and coma.
Tberculous Meningitis Signs
- Head retraction is present in infants and children.
- Neck rigidity, i.e. bending of neck causes pain and spasm of neck muscles or it is diffilt to bend the neck.
- Kernig’s sign is positive
- Brudzinski’s sign is also positive if patient is conscious.
- Presence of papilledema
- Presence of cranial nerve palsies
Tberculous Meningitis Diagnostic Features
- Person with history of contact with tubercular patient presenting with low grade fever, ill health, weight loss, odd behavior, headache should make one suspect tubercular meningitis.
- Diagnosis shall be confimed by the lumbar puncture.
CSF examination reveals following results:
- CSF is straw colored, clear but when allowed to stand, a fie clot, i.e. spider web is formed.
- Lymphocyte count is high
- Protein content is high
- Glucose is low
- In acute cases, polymorphs may predominate AFB stain can be positive. Culture or AFB is positive in 80% of cases
CT or MRI brain may show meningeal enhancement or hydrocephalous
Question.21. Describe causes, clinical features, treatment and complication of meningitis.
Answer.Inflmmation of the meninges is called as meningitis.
Meningitis Causes
Infectious causes:
Bacterial:
- Common: N. meningitides, S. pneumoniae, H.inflenza, M tuberculosis
- Neonatal: Group B streptococcus, E. coli, L.monocytogenes
- Uncommon: S. aureus, Ps. Areuginosa
- Rare: Salmonella, Shigella, N. gonorrhea
Viral:
- Common: Mumps, Echovirus, Coxsackie virus A and B, Genital herpes virus 1 and 2
- Neonatal: Other herpes virus, EpsteinBarr virus,
Varicella zoster virus - Uncommon: Cytomegalovirus, HIV, Lymphocytic choriomeningitis virus
- Rare: Adenovirus Types 3 and 7, Arbovirus
- Protozoa: Naegleria
- Fungal: Cryptococcus neoformans, Candida
- Spirochaetal: Leptospirosis, Syphilis and Lyme disease
- Ricketssial: Typhus fever
Noninfectious causes
- Malignant: Leukemic meningitis Other non-infectious causes:
- Sarcoidosis, connective tissue disease, systemic lupus erythematosus,
Sjögren’s syndrome - Vasculitis: Granulomatous polyangiitis, Eosinophilic granulomatous polyangiitis, CNS vasculitis
Meningitis Clinical Features
Meningitis Symptoms
- Fever coming with rigors
- Headache which is severe mainly in frontal region radiating down to back
- Vomiting
- Convulsion in children
- Malaise
- Severe photophobia
- Ptosis due to raised intra cranial tension
- Stiffess in neck and back
- Pain in neck
- Impairment of consciousness, i.e. confusion, delirium and coma
Meningitis Signs
- Head retraction is present in infants and children.
- Neck rigidity, i.e. bending of neck causes pain and spasm of neck muscles or it is diffilt to bend the neck.
- Kernig’s sign is positive
- Brudzinski’s sign is also positive if patient is conscious.
- Presence of papilledema
- Presence of cranial nerve palsies
Meningitis Treatment
Empirical treatment should be given before CSF culture and
Gram stain report.
Treatment should be directed to the most common microorganism present in particular age group.
Meningitis Antibiotic treatment
- Ceftriaxone or cefotaxime is given against S. pneumonia,H. inflenzae, Group B streptococci and N. meningitides.
In this vancomycin can be added to cover cephalosporin resistant S. pneumonia. Ampicillin can be added to cover L. monocytogens in neonates of less than 3 months and more than 55 years of age. - Ceftazidime is active against P. aeuroginosa and is preferred over ceftriaxone or cefotaxime in hospital acquired meningitis.
- Choice of empirical antibiotics in pyogenic meningitis is:
- In neonates or infants of less than 3 months: Ampicillin 100 to 50 mg/dL + Ceftriaxone 500 to 1000 mg/kg/day or cefotaxime 50 mg/kg
- In children and adults: Ceftriaxone 500 to 1000 mg/kg/day or cefotaxime 50 mg/kg + vancomycin 60 mg/Kg
- Adults more than 55 years: Ampicillin 3 gm TDS or QDS + Ceftriaxone 2gm BD or cefotaxime 50 mg/kg + vancomycin 1gm 8 hourly
- In hospital acquired meningitis, posttraumatic or postsurgical, immunocompromised patients: Ampicillin 3 gm TDS or QDS + Ceftazidime 2 gm 8 hourly + vancomycin 1gm 8 hourly.
“How does Alzheimer’s disease impact the nervous system? FAQ explained”
Duration Of Antibiotic Therapy
- One week for H. inflenzae and N. meningitides infection
- S. pneumoniae for two weeks
- L. monocytogenes and Gramnegative bacilli infections for 3 weeks
Adjunctive Therapy
Dexamethasone 0.4 mg/kg BD for 4 days with fist dose of antibiotic.
Supportive Therapy
- Patients having raised intracranial pressure should be treated in ICU.
- IV mannitol, hyperventilation and elevation of patient’s head to 30° is done to decrease raised intracranial pressure.
Treatment
Emperical treatment should be given before CSF culture and Gram stain report.
Treatment should be directed to the most common microorganism present in particular age group.
Antibiotic Treatment
- Ceftriaxone or cefotaxime is given against S. pneumonia,H. inflenz, Group B streptococci and N. meningitides.
In this vancomycin can be added to cover cephalosporin resistant S. pneumonia. Ampicillin can be added to cover L.monocytogens in neonates of less than 3 months and more than 55 years of age. - Ceftazidime is active against P. aeuroginosa and is preferred over ceftriaxone or cefotaxime in hospital acquired meningitis.
- Choice of empirical antibiotics in pyogenic meningitis is:
- In neonates or infants ofless than 3 months: Ampicillin 100 to 50 mg/dL + Ceftriaxone 500 to 1000 mg/kg/day or cefotaxime 50 mg/kg
- In children and adults: Ceftriaxone 500 to 1000 mg/kg/ day or cefotaxime 50 mg/kg + vancomycin 60 mg/kg
- Adults more than 55 years: Ampicillin 3 gm tds or QDS + Ceftriaxone 2 gm BD or cefotaxime 50mg/kg + vancomycin 1gm 8 hourly
- In hospital acquired meningitis, posttraumatic or postsurgical, immunocompromised patients—Ampicillin 3 gm tds or qds + Ceftazidime 2gm 8 hourly+ vancomycin 1 gm 8 hourly.
Duration of Antibiotic Therapy
- One week for H. inflenzae and N. meningitides infection
- S. pneumonia for two weeks
- L. monocytogenes and Gramnegative bacilli infections for 3 weeks.
Adjunctive Therapy
Dexamethasone 0.4mg/kg BD for 4 days with fist dose of antibiotic.
Supportive Therapy
- Patients having raised intracranial pressure should be treated in ICU.
- IV mannitol, hyperventilation and elevation of patient’s head to 30° is done to decrease raised intra-cranial pressure.
Complications
- Neurological defiiencies: Hemiplegia, aphasia, hemianopia,blindness, deafness.
- Mental deterioration
- Cerebritis, brain abscess, focal fis, auditory impairments,subdural empyema, internal hydrocephalus.
Question.22. Discuss causes and management of unconsciousness.
Answer. Causes of Unconsciousness
Decrease in the cerebral perfusion:
Inadequate vasoconstriction mechanism
- Postural hypotension
- Vasovagal shock
- Antihypertensive drugs
- Carotid sinus syncope.
Hypovolemia:
- Addison’s disease
- Due to blood loss i.e. hemorrhage.
Decrease in the venous return
- Mediastinal compression
- Micturition
- Cough
- Straining during defecation.
Decrease in cardiac output
- Myocardial infarction
- Pulmonary embolism
- Aortic stenosis
- Cardiac temponade.
Arrhythmias
- In AV blocks
- Supraventricular tachycardia
- Ventricular asystole
- Ventricular tachycardia.
Cerebrovascular disturbances
- Hypertension
- Transitory ischemic attck
- Vertebrobasilar insuffiency.
Non-circulatory causes:
- Anemia
- Anxiety neurosis
- Hypoxia.
Management
- All the medical/dental procedure or treatment is stopped.
- Remove instruments from oral cavity such as rubber dam,gauze, cottn etc.
- Patient is kept in Trendelenburg position, i.e. patient is kept in a head low and feet up position.
- Loose tighten clothing of patient.
- Aromatic fumes inhalation is given or sprinkle cold water on face of patient for reflx stimulation.
- If recovery is gained escort patient home.
- If recovery is not gained Injection Atropine 0.6 mg IM or I.V. is given.
- If still recovery is not gained look for hypoglycemia and Addison’s crisis
- Start basic life support
- Summon medical help.
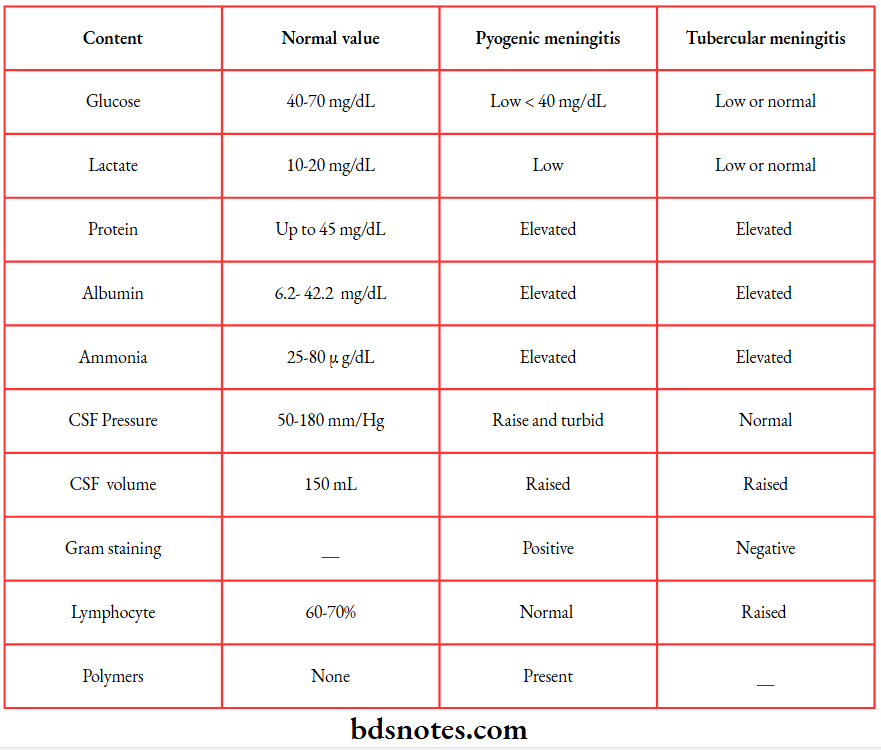
Question.23. Describe the CSF picture of pyogenic meningitis and tubercular meningitis.
Answer.
“Early warning signs of gaps in understanding nervous system disease basics: Common questions”
Question.24. Discuss the causes of headache.
Answer. The causes of headache are:
Intracranial and local extracranial
- Trauma leads to contusional or posttraumatic headache
- Intracranial inflmmations: Meningitis, encephalitis, cerebral abscess.
- Vascular headaches: Hypertension, cerebral or subarachnoid hemorrhage, intracranial aneurysm;vasodilator drugs like nitrites and histamine,adrenaline.
- Menopausal: Alcohol hangover or withdrawal, coffe withdrawal. Giant cell arteritis (temporal arteritis),thrombosis of intracranial venous sinus.
- Traction headache: Pain produced by intracranial arterial displacement and distortion of the dura, usually caused by space occupying lesions or raised intracranial pressure or low intracranial pressure (intracranial hypotension).
- Post-lumbar puncture headache: Low CSF pressure headache.
- Cough headache: A benign syndrome of severe headache which accompanies coughing, straining or sneezing can be due to posterior fossa tumour.
- Cranial neuritis and neuralgias: This is of sensory nerves of scalp, e.g. orbital neuralgia, or neuralgia of auriculotemporal, posterior auricular or great occpital nerves, herpes of Gasserian ganglion.
General Or Systemic Causes
- Anoxemia: Anemia, carbon monoxide or carbon dioxide poisoning.
- Toxic: Fevers, uremia, eclampsia, metallic poisoning,”alcoholic” hangover, postconvulsive, drugs like quinine, tobacco, cocaine, morphine, sulphonamides.
Pelvic or gallbladder disease, constipation, intestinal stasis. Nervous exhaustion. - Metabolic factors: Hypoglycemia, alkalosis or acidosis.
- Hemopoietic factors: Essential polycythemia,thromobasthenia.
Referred pain
- Eyes: Errors ofrefraction, glaucoma, iritis, etc.
- Ears: Otitis, mastoiditis, vestibular nerve lesions,
- Eustachian tube block, tumors of middle and inner ear.
Teeth: Impacted teeth, infected tooth sockets and dental roots. - Paranasal sinuses: Infection of paranasal sinuses may cause localized pain.
- Neck: Diseases of upper cervical spine may be associated with both occipital and frontal pain.
- Psychogenic: Common cause of headache in depression.
- Tension (muscle contraction) headache:
- Pain resulting from sustained contraction of skeletal muscles of the neck, frontalis, occipital muscles due to emotional tension.
- Exertional headache:
Headache may come on during exertion and persist for few hours afterwards.
Other primary headaches:
- Hypnic headache syndrome is a late onset disorder and usually wakes up the patient from sleep at around the same time every night.
The headache is usually treatable with flnarizine and lithium. - Exploding head syndrome can occur any time during day or night.
Question.25.Write short note on defiition and classifiation of epilepsy.
Answer. Epilepsy is defied as condition characterized by the recurrent episodes primarily of cerebral origin in which there is disturbance of movement, sensation, behavior and consciousness.
Classifiation
Classifiation of epileptic seizures modifid in 1981 Partial or focal seizures:
Simple partial seizures (awareness preserved)
Depending on the concomitant signs, they are:
- Motor
- Sensory
- Visual
- Versive
- Psychomotor
Complex partial seizures (awareness lost)
Depending on the area involved due to spread, they are:
- Temporal lobe
- Frontal lobe
Secondary generalized partial seizures
Primary generalized seizures:
- Tonic clonic (grand mal)
- Tonic
- Absence (petit mal)
- Akinetic
- Myoclonic
- Infantile spasms
Unclassifid seizures:
Seizures which do not fi into above two categories;
- Neonatal seizures
- Infantile spasms
Question.26.Write short note on panic attck.
Answer.
Panic attacks are discrete episodes of paroxysmal severe anxiety and are characterized by severe and frightening autonomic symptoms, i.e. shortness of breadth, palpitations, excessive perspiration; dizziness,faintness and chest pain.
Many patients believe they are in immediate danger of death or collapse and seek urgent medical attntion.
Typical Feature Of Panic Attack
- It is of sudden onset and short duration
- It shows rapidly escalating physical and psychological
Symptoms - Presence of incapacitating symptoms of breadthness and/or palpitations
- Fear of impending death, collapse or loss of control
- Rapid escape from situation where attck is occurred
- Sometimes panic attcks are labeled nocturnal when they occur at night only
- Panic attck in social phobia is restricted to feared social situations
- Panic attck in panic disorder occurs unexpectedly in social encounters and when person is alone.
Diagnostic Guideline For Panic Attack
- A panic attck is characterized by all ofthe following:
- A discrete episode of intense fear or discomfort
- It starts abruptly
- It reaches maximum intensity within a few minutes
- It lasts for at least several minutes
- At least four symptoms are present (including at least one autonomic symptom)
- The attack is not caused by a physical disease, an organic mental disorder, or another condition such as schizophrenia, mood disorder or somatoform disorder.
- Panic attck may accompany any anxiety disorder, but a specifi diagnosis of panic disorder can be made if they occur frequently and unexpectedly.
Management
Psychological:
- Helping patients to understand that their symptoms are not caused by serious physical ailment.
- Relaxation training can be helpful, but severely ill patients are more likely to benefi from cognitive behavior therapy.
- Exposure therapy can be formed under supervision of a behavior therapist.
Drugs:
- High dose benzodiazepines, e.g. alprazolam are effctive but can cause substantial depression and should be prescribed in severely ill patients who have not responded to other treatment approaches.
- Antidepressant drugs, i.e. imipramine, clomipramine and selective serotonin reuptake inhibitors, i.e. paroxetine are as efficacious in reducing anxiety symptoms, lessening agoraphobia and minimizing overall impairment.
Question.27. Write short note on depression.
Answer. Depression is defied as depressed mood on a daily basis for a minimum duration of two weeks.
Depression is present in a quarter to half of all mental patients.
Etiology
- Genetic factors: They play a major role in mood disorders and their effct is stronger in patients with more severe biological symptoms.
In twin studies of bipolar disorder, average concordance rate is 65% in monozygotic twins and 14% in dizygotic twins. - Social factors: Events associated with depression are generally ’loss events’ such as loss of a job, relative or tend, money, health or status.
Other factors that adversely affct the response to the events can be, a working class background, lack of confiing relationship with a spouse, unemployment, loss of a parent before l l years of age. - Biological markers for depression: They show strong associations, particularly with the somatic (endogenous) syndrome.
Falsepositive results occur in the presence of various medical disorders.
Dexamethasone suppression test is the most important biological marker. - Circadian rhythms and related markers: They have also been found abnormal in depression.
This is suggested by the diurnal variations in mood, early morning waking and the sometimes periodic course, for example, yearly attcks of illness. - Psychological factors: Repeated trauma, stressful life events and disturbed marital and interpersonal relationships.
Clinical Features
- General: Hopelessness, helplessness, low mood, low self esteem, reduced energy, suicidal thoughts, loss of interest,poor concentration, guilt, pessimism, depersonalization.
- Somatic: Appetite disturbance, weight change, constipation,amenorrhea, low libido, sleep disturbance
- Anxiety: Tension, apprehension, phobias.
Management
- Antidepressants are used in all phases of the treatment of major depression, acute management, continuation therapy and maintenance or prophylactic treatment.
- Tricyclic drugs: They increase recovery rate signifiantly,but have a wide range of side effcts. These lead to noncompliance and limit usefulness in illnesses of mild to moderate severity.
The dose of tricyclics should be initially low and increased gradually. - Selective serotonin re-uptake inhibitors: They are effctive drugs and are bettr tolerated at therapeutic doses than other compounds.
- If patient is not responding to antidepressant drugs ECT treatment should be given. Usually 6 to 10 ECTs are effctive in resolving acute depression.
As course is completed prophylactic treatment should be given to prevent relapse - Congenitive psychotherapy should also be done

“Asymptomatic vs symptomatic effects of ignoring nervous system disease principles: Q&A”
Question.28. Write short note on anxiety neurosis.
Answer.
Anxiety is a normal response to threat or stressful events and is usually short lived and controllable.
It probably functions as an ‘alarm mechanism’ to prepare an individual for a physical response to perceived danger (the fiht or—flght’ response).
Anxiety symptoms are considered clinically signifiant when they:
- Are abnormally severe
- Are unusually prolonged
- Occur in absence of stressful circumstances
- Impair physical, social or occupational functioning
Features of anxiety neurosis
Anxiety Neurosis Psychological
- Fear and apprehension
- Inner tension and restlessness
- Irritability
- Impaired ability to concentrate
- Increased startle response
- Increased sensitivity to physical sensations
- Disturbed sleep
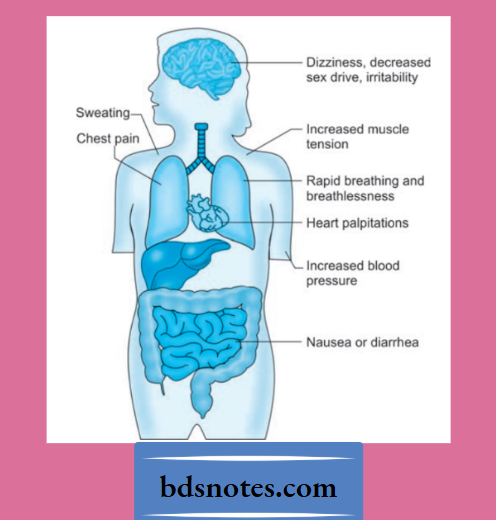
Anxiety Neurosis Physical
- Increased muscle tension
- Tremor
- Sweating
- Palpitations
- Chest tightness and discomfort
- Shortness of breath
- Dry mouth
- Diffilty in swallowing
- Diarrhea
- Frequency of micturition
- Loss of sexual interest
- Dizziness
- Numbness and tingling
- Faintness
Anxiety Neurosis Management
Defiitive need for treatment depends on severity of symptoms,degree of personal distress, level of occupational and social impairment.
- Benzodiazepines are effctive anxiolytic drugs but can cause sedation and have potential for dependence.
They should be given in short courses. - Other drugs include certain tricyclic antidepressants e.g.imipramine (50 300 mg/d), buspirone (15–45 mg/d) and venlafaxine (serotonin—noradrenaline re uptake inhibitor 75 mg/d) none of which have same potential for psychological or physical dependence.
- Behavior therapy in form of relaxation training, systemic desensitization and cognitive therapy.
Psychotherapy and family education is must.
Question.29. Describe clinical features, diagnosis and management of tubercular meningitis.
Answer.
Tubercular Meningitis Clinical Features
Tubercular Meningitis Symptoms
- Headache
- Vomiting
- Low grade fever
- Lassitude, i.e. weariness or exhaustion
- Depression
- Confusion
- Behavior changes.
Tubercular Meningitis Signs
- Meningism may be present:
- Oculomotor palsies
- Papilledema
- Depression of conscious level
- Focal hemisphere signs.
Tubercular Meningitis Diagnosis
- Person with history of contact with tubercular patient presenting with low grade fever, ill health, weight loss, odd behavior, headache should make one suspect tubercular meningitis.
- Diagnosis shall be confimed by the lumbar puncture. CSF examination reveals following results:
- CSF is straw colored, clear but when allowed to stand,a fie clot, i.e. spider web is formed.
- Lymphocyte count is high
- Protein content is high
- Glucose is low
- In acute cases, polymorphs may predominate
- AFB stain can be positive. Culture or AFB is positive in 80% of cases
- CT or MRI brain may show meningeal enhancement or hydrocephalous
Tubercular Meningitis Management
General management
- Maintenance of nutrition, hydration and electrolyte balance.
- Case of bowel and bladder
- Nursing should be good
- If there are convulsions, anticonvulsants are given.
Tubercular Meningitis Treatment
- Antitubercular drugs: Antitubercular drugs—
Rifampicin 600 mg/day + Isoniazide (600 to 900 mg/day) + Pyrazinamide (1.5 gm) should be given.
Treatment with this regimen is given for 2 months.
This is followed by rifampicin 600 mg/day + Isoniazide (600 to 900 mg/day) for 12 to 18 months. - Steroids: Prednisolone 40–60 mg/day to reduce toxicity, piaarachnoid adhesions and felling of wellbeing.
Question.30. Write short note on examination of cerebrospinal flid.
Answer.
Normal CSF is colorless, clear.
- Presence of blood indicates either local trauma or subarachnoid hemorrhage especially fresh.
- Xanthochromia or yellowish coloration of CSF is found in cerebral hemorrhage and when pus is present in CSF in considerable amount.
- Turbidity when present indicates excess of polymorphonuclear cells (meningitis).
- A clot or cob web may form in cases of tuberculous meningitis.
- Of the biochemical tests, protein content is 30–40 mg/dL and sugar 80 mg/DL.
- Normal CSF contains a small number of cells mostly lymphocytes (0–5/cumm).
- Excess of cells in the CSF indicate meningeal irritation.
- In cases of meningitis, CSF is examined for bacteria by gram’s staining.
- A culture examination of CSF is often carried out in suspected infective process for identifying the causal organism.
- CSF examination has animportant role indiagnosing bacterial and viral diseases, but its role in cases of cerebral hemorrhage is now being taken over by CT scan because of hazards involved.
- Colloidal reactions in the form of colloidal gold reaction is of value in cases of general paralysis of insane (GPI) and diffrentiates it from other form of neurosyphilis.
- Serological reactions like wasserman reaction are also of help in cases of neurosyphilis.
Question.31. Diffrentiate between syncope and epilepsy.
Answer.

“Can targeted interventions improve outcomes for nervous system disease patients? FAQs provided”
Question.33.Write short note on transient ischemic attck.
Answer.
These are transient attcks of loss of function of one part of the brain coming suddenly and lasting for variable period of time ranging from minutes to hours.
- Since arteries supplying the brain are end arteries so any pathology which produces obstruction to the flw of that vessel shall produce symptoms in the distribution of that blood vessel.
- Internal carotid artery is one of the commonest cerebral vessel which is involved by atherosclerosis and patient complains of transient disturbances due to localized cortical ischemia in the form of confusion contralateral hemiparesis and sensory loss.
There may be aphasia (if lesion on left side) and hemianopic visual loss. - Most commonly occlusion is in the common carotid artery and one may be able to appreciate diminished pulsation in the vessel in the neck.
When obstruction is severe a bruit may be auscultated at the site. - Obstruction of other arteries like anterior cerebral artery, middle cerebral artery and posterior cerebral artery produce picture almost like above except for litte variations depending on the occlusion site.
- On the other hand involvement of posterior circulation (basilar artery, vertebral artery, postinferior cerebellar artery) produces a picture of crossed hemiplegia, hemisensory loss and hemianopic visual loss. In addition patient has impairment of consciousness, small fied pupils,pseudobulbar palsy and quadriplegia seen mainly.
- In basilar artery lesions while cases with posterior inferior cerebellar artery involvement are associated with severe vertigo, vomiting, dysphasia and diplopia. In addition there is some degree of cerebellar defiiency with hypotonia and incoordination on the side of lesion, analgesia and thermoanesthesia on the face on the side of lesion and on the trunk and limbs on opposite side.
- Again neurological defiits shall be depending on which branch of the vessel is involved.
Question.34. Write short note on facial pain.
Answer. Various number of conditions are involved in the pain localized to face.
These may range from pain arising from diseases of teeth, gums, sinuses, temporomandibular joint to various causes.
Facial neuritis
- It is a form of inflmmation of the nerve of the face and scalp.
- It generally occurs as a complication of a septicemic estate or due to involvement by a neurotropic virus.
- Onset is usually acute and pain is confied to the face and scalp, occurring in paroxysms lasting for several hours and very often till the end of the day when the patient is exhausted.
- If the character ofpain is dull aching which is intensifid by exposure to cold and often occurs in the form of shooting pains in the distribution of the nerve.
Sometimes the pain is so severe that the patient is unable to sleep. - Physical examination shows presence of hyperalgesia in the distribution of nerves including face and scalp.
Nerve trunk is tender on pressure.
Myofascial Pain
- It is a form of dull constant pain with local tenderness of the muscles of jaw.
- There is often pain and diffilty in opening the mouth.
- This pain is related to bad and improper habits of clenching and grinding of teeth. This type of habit is present amongst hysterical persons especially women who often clench and grind their teeth.
- There is no physical fiding in such people except that these people have an emotionally labile personality and often suffr from depression.
- Treatment consists in giving them assurance, analgesics and tricyclic antidepressants.
Trigeminal Neuralgia
Trigeminal neuralgia is also called as Tic Douloureux.
A disorder characterized by the *paroxysmal attcks of neuralgic pain with affction of one or more division of trigeminal nerve.
The pain involves the third and second divisions equally and rarely the fist.
Clinical Features
- Pain is unilateral and is confined to one of the three divisions of nerve. Pain is sharp and onset is sudden. The pain is only of a few seconds.
- During the attcks there is flshing of face, i.e. redness of the face.
- Dilatation of pupil is present.
- There is excessive lacrimation
- After repeated attcks skin becomes shiny and hair in the area becomes gray.
- Sometimes secretion of nasal mucus and saliva may occur in the side of pain.
Etiology
Trigeminal neuralgia is spontaneous and following exposure to cold wind, blow on face, or chewing or eating, drinking hot or cold flid and washing the face.
Management
- Elimination of all possible sources of infection.
- Drugs:
- Analgesics: Potent analgesics must be used with caution because of danger of habituation.
- Carbamazepine: 100–200 mg BD a day and increasing the dose to 600–800 mg per day.
- Phenytoin sodium: 0.1 gm TDS when carbamazepine is not tolerated.
- Vitamin B12: 1000 μg IM daily for two weeks.
- Injection ofalcohol: It is given in affcted nerve, or gasserian ganglion.
If more than one division is affcted inject 10 minims of 90% alcohol after local anesthesia with 2–3 drops of procaine. - Microvascular decompression: In this there is separation of blood vessels is done which are in contact with trigeminal nerve roots.
There is also insertion of non absorbable sponge which provide relief of pain in most of the patients. - Radiofrequency thermocoagulation: This procedure is carried out at the trigger spot or site of pain origin which is localized by electric stimulation of needle inserted in trigeminal ganglion and leads to permanent relief.
- Surgery: In this selective or complete preganglionic section of trigeminal root is done.
This technique can lead to disadvantages such as permanent dysesthesiae.
Another bettr technique is percutaneous electrocoagulation of preganglionic rootlets corresponding to trigger zone, the temperature of probe being so regulated as to coagulate small thinly myelinated pain fiers but preserving most heavily myelinated touch fiers.
Post Herpetic neuralgia
- Herpes zoster commonly involves the ophthalmic division of the 5th nerve characterized by vesicular eruption on the face and pain.
When herpes heals it leave behind neuralgic pain in the distribution of previous eruptions. - It is a form of continuous aching or burning pain at that site on face and patient is often in great agony.
- Treatment is by analgesics. Sometimes codeine phosphate may have to be given.
- In some severe cases the course of post herpetic neuralgia may be prolonged one.
Migrainous neuralgia
- It is often called ‘Facio plegic migraine’ where there are attcks of severe pain especially at night and the pain is confied to face and around one eye.
This form of disease is common in men especially middle aged and the attck may be brought on after a bout of alcohol. - The pain may last for our. Because of associated vomiting and paroxysmal nature of disease it is called ‘migrainous neuralgia’ or ‘facioplegic migraine.
There is headache and patient complains of some degree of congestion in the face. - Treatment is by analgesics but response is poor.
Arthralgia Of Temporomandibular Joint
- It may be in the form of rheumatoid arthritis or ankylosing spondylitis when there is pain and swelling of the joint.
- Movements at the joint are limited and patient complains of pain at the site as well as along the jaw confied to face.
Involvement of other joints in the body shall favor the diagnosis. - Treatment is by heat and anti-inflmmatory drugs as well as by exercises of the joint involved with adequate periods of rest.
Temporal Arteritis
- It is a form of collagen disorder of unknown etiology which involves mainly the arteries.
- It commonly occurs in elderly age group.
- Patient may complain of pain on the face, jaw, mouth and tongue in the distribution of branches of external carotid artery.
- This pain worsens of if on eating and opening of the mouth.
- Since temporal arteritis is a collagen disorder there is a form of inflmmation of the arteries.
Question.35. Write short note on temporal lobe epilepsy.
Answer.
Temporal lobe epilepsy is a form of focal epilepsy,a chronic neurological condition characterized by recurrent seizures.
Temporal lobe epilepsy (TLE) is the most common single form causing refractory epilepsy.
Temporal lobe epilepsies are a group of medical disorders in which humans and animals experience recurrent epileptic seizures arising from one or both temporal lobes of the brain.
Types
- Two main types are internationally recognized:
Medial temporal lobe epilepsy (MTLE): arises in the hippocampus,parahippocampal gyrus and amygdala which are located in the inner aspect of the temporal lobe. - Lateral temporal lobe epilepsy (LTLE): arises in the neocortex on the outer surface of the temporal lobe of the brain.
Symptoms And Signs
- Simple partial seizures (SPS) involve small areas of the temporal lobe such as the amygdala or the hippocampus.
The term “simple” means that consciousness is not altered.
In temporal lobe epilepsy SPS usually only cause sensations. These sensations may be mnestic such as déjà vu (a feeling of familiarity), jamais vu (a feeling of unfamiliarity), a specifi single or set of memories, or amnesia.
The sensations may be auditory such as a sound or tune, gustatory such as a taste, or olfactory such as a smell that is not physically present.
Sensations can also be visual, involve feelings on the skin or in the internal organs.
The lattr feelings may seem to move over the body.
Dysphoric or euphoric feelings, fear, anger, and other sensations can also occur during SPS.
Often, it is hard for persons with SPS of TLE to describe the feeling.
SPS are often called “auras” by lay persons who mistake them for a warning sign of a subsequent seizure.
In fact, they are actual seizures in and of themselves.
Persons experiencing only SPS may not recognize what they are or seek medical advice about them.
SPS may or may not progress to the seizure types listed below. - Complex partial seizures (CPS) by defiition are seizures which impair consciousness to some extent.
This is to say that they alter the person’s ability to interact with his or her environment.
They usually begin with an SPS, but then the seizure spreads to a larger portion of the temporal lobe resulting in impaired consciousness.
Signs may include motionless staring, automatic movements of the hands or mouth, altered ability to respond to others, unusual speech,or unusual behaviors. - Seizures which begin in the temporal lobe but then spread to the whole brain are known as secondarily generalized
TonicClonic Seizures (SGTCS).
Treatment
- In temporal lobe epilepsy, the most commonly used drugs are phenytoin, carbamazepine, primidone, valproate and phenobarbital.
- Newer drugs, such as gabapentin, topiramate, levetiracetam,lamotrigine, pregabalin, tiagabine, lacosamide, and zonisamide promise similar effctiveness, possibly with fewer side-effcts.
- For patients with medial TLE whose seizures remain uncontrolled after trials of several antiepileptic drugs,resective surgery should be considered.
“Differential applications of central vs peripheral nervous system diseases: Questions answered”
Question.36. Write in brief signs, symptoms and treatment of epilepsy.
Or
Write short note on epilepsy.
Answer. Epilepsy is defied as the group of disorders in which there are recurrent episodes of altered cerebral functions associated with paroxysmal and hypersynchronous electrical discharge of cerebral neurons.
Symptoms
- Aura is present which means there is warning of the attck.
- Loss of consciousness
- Patient fall over the ground
- Irritability
- Depression and abnormal feelings
- Giddiness and abdominal cramps
- When patient awakes he complains of headache
Signs
- Tonic contraction of muscles and epileptic cry produced by forceful expiration through the partly closed vocal cords.
- Tonic convulsions of two sides of the body occur with head and eyes rotated to one side.
- Tonic phase followed by clonic phase, i.e. after completion of tonic phase patient remain unconscious for few minutes to half an hour.
- Frothing of mouth and increased salivation from the mouth.
- During clonic phase patient may bite his tongue and pass urine and stools.
Treatment
Treatment of epilepsy is directed at the elimination of the cause of seizures, suppressing the expression of seizures and dealing with psychosocial consequences.
Immediate treatment ofa seizure:
- Patient should always be migrated to the safer place.
- Loose the clothes around the neck and move people away from the place so that patient can breathe fresh air easily.
- At the time of convulsion, helpers are not allowed to put the figers inside the mouth. Tongue biting should be prevented by puttng tightly rolled piece of cloth in mouth.
- As convulsion ceases, patient is turned into semiplane position and make air passage clear.
- Patient is advised to consult the doctor for medical advice.
Drug therapy:
Choice of the drug depends on type of seizure.
- In localization related epilepsy fist line prophylactics are lamotrigine, carbamazepine (slowrelease),oxcarbamazepine, levetiracetam.
- In primary generalized, symptomatic generalized and unclassifid epilepsies, initial therapy should be lamotrigine or valproate (broad spectrum gents).
Valproic acid is useful in absences and benzodiazepines in myoclonic jerks. - Patients with refractory generalized epilepsy may benefi from adjunctive treatment with topiramate or levetiracetam, zonisamide, clonazepam, pregabalin.
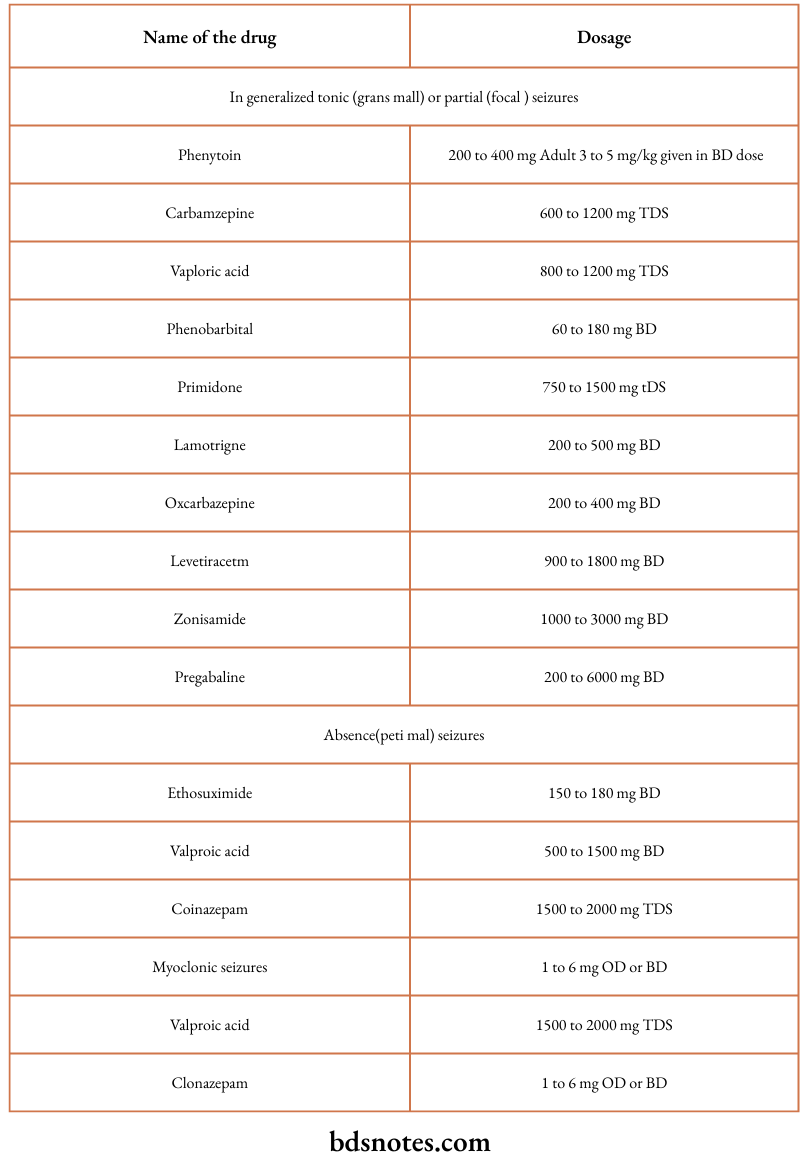
Various antiepileptic drugs along with their dosages used in epilepsy are:
Plan of treatment
- Initial regimen: The drug selected must be used in monotherapy.
The drug should be introduced in small doses, since rapid introduction may cause side effcts. - Maintenance treatment: The aim should be to find the lowest dose which achieves complete seizure control without side effcts which may be either idiosyncratic or due to intoxication, or chronic.
Serum anticonvulsant levels are a useful guide to therapy phenytoin (40–80) carbamazepine (20–50), phenobarbitone (40–170),ethosuximide (20–600).
Valproate 300-600, oxcarbazepine 50–125, lamotrigine 4–60 mmol/L.
If the optimum level of a single, fist line drug does not control seizures, or if side-effcts develop, the initial drug should be substituted with another fist line anticonvulsant.
If the second drug also fails to control seizures monotherapy with a third anticonvulsant, or combination therapy with two fist line drugs should be tried.
If a combination of two fist-line drugs is unsuccessful, one of the secondline drugs may be considered.
Drug Withdrawl
It should take place slowly over 2 to 3 months. If patient is receiving more than one drug, each drug should be withdrawn individually.
Question.37. Write in brief signs, symptoms and treatment of facial palsy.
Or
Write signs and symptoms of facial palsy.
Answer. It is the paralysis of the facial nerve.
Symptoms
- Post auricular pain is common and may precede paralysis by 2 days.
- Spontaneous complains of loss of taste sensation,hyperacusis and watering of eyes.
- Sweating is less over the affcted side.
Signs
- Forehead cannot be wrinkled; frowning lost.
- Eye of affcted cannot be closed.
On attmpting closure,eyeball turns upwards and outwards (Bell’s phenomena). - On showing the teeth, the lips do not separate on affcted side. Whistling not possible.
Articulation of labial components diffilt. Naso-labial fold flttned out.
Angle of mouth on affcted side droops with dribbling of saliva. - Cheek puff out with expiration because of buccinator paralysis.
Food collects between teeth and paralyzed cheek.
Fluid runs out while drinking. - Base of tongue is lowered.
- Vesicles within the external auditory meatus and ear drum in Ramsay Hunt syndrome.
Pain may precede facial weakness. Deafness may result.
Treatment
- Local heat: Infrared or moist heat over the face or parotid region or both if there is tenderness of nerve trunk.
- Local treatment ofmuscles: The patient should massage the facial muscles with bland oil for twice a day for 5 min.
The massaging movements should start from the chin and lower lip and are directed upwards.
With return offunction the patient should practice movements of various muscles of face before a mirror. - Prevention offacial sagging: Application of strips of adhesive tape is done to lift up the angle of mouth.
Tape is attched to the temple and extends down in a V shaped fashion to upper and lower lips. - Protection of eye: It is done with dark glass or eye patch.
Mild zinc boric solution is used to wash the eye to prevent conjunctivitis. - Corticosteroids: If seen under a week of onset. Prednisolone 40 mg/day for 4 days and in tapering doses for over next 6 days helps by reducing secondary edema.
- Anti-virals: Acyclovir, Valacyclovir or Famciclovir in combination with steroids, ifstrated within 3 days ofonset.
- Surgery: Decompression of facial nerve in second or third week cannot inflence favorably natural course of Bell’s palsy. Cases which fail to recover after 9 months in them anastomosis of facial nerve with accessory or preferably hypoglossal nerve is considered, or plastic surgery in cases of total paralysis with atrophy of muscle.
“Steps to master nervous system diseases for exams: Study plans vs mock tests: Q&A guide”
Question.38. Write on causes of meningitis and discuss in detail bacterial meningitis.
Or
Describe the etiology, clinical features and management of bacterial meningitis.
Answer.
Following are the causes of meningitis:
- Neonates: E.coli
Children:
- H. inflenzae
- S. pneumoniae
- N. meningitidis.
Adults:
- Young people: Meningococcus
- Older people: S. pneumonia.
Elderly and immunocompromised persons:
- Pneumococcus
- Listeria
- Tuberculosis
- Gramnegative organism
- Cryptococcus.
Viral:
- Enterovirus
- Herpes simplex virus
- Mumps virus
- Inflenza virus
- Japanese encephalitis virus
- Arbo viruses
- Rabies virus
- HIV.
Nosocomial and post-traumatic meningitis:
- Klebsiella pneumonia
- E.coli
- Pseudomonas aeruginosa
- S. aureus.
Meningitis in special situation:
- CSF shunts staphylococcal
- Spinal procedurespseudomonas.
Bacterial Meningitis
Pathophysiology Involves
- Transmission, colonization and invasion of nasopharyngeal epithelium.
- Survival in the blood stream by evading host immune response.
- Meningeal invasion. Bacteremia may be rapidly followed by seeding of meningeal pathogens and secondary infection of the meninges.
- CSF inflmmatory response.
- Cerebral edema and thrombosis.
- Bacterial meningitis causes loss of cerebrovascular anticoagulation.
Clinical Features
Symptoms
- Fever, malaise headache and vomiting.
- Pain over the neck
- Stiffess over the neck
- Confusion, delirium and coma.
Signs
- Kernig’s sign is positive.
- Neck rigidity, i.e. when neck is bended there is presence of pain and there is spasm of neck muscles.
- Brudzinski’s sign is also positive.
- Photophobia is present
- Cranial nerve palsies most commonly IIIrd, IVth, VIth and VIIth.
- Focal neurological defiits such as nystagmus, aphasia, ataxia and peripheral nerve palsies.
- Partial or generalized seizures tend to be more common in Strep. pneumoniae and HIV meningitis.
- Purpura or petechiae in meningococcal meningitis, with or without features of septic shock.
Diagnosis
- Examination of CSF
Typical CSF fidings in acute bacterial meningitis: - Raised WBC count (usually 100–60,000 cells/mL (predominantly neutrophils)
- Reduced CSF glucose (30–40% serum glucose level)
- Raised CSF protein (0.5–5 g/L)
- Gramstaining of CSF is positive in over 90% of cases of hematologically acquired meningitis.
- Blood culture should be performed in all patients with suspected meningitis, and latex agglutination bacterial antigen test or polymerase chain reaction analysis (to detect bacterial DNA) may be performed on blood or CSF to try to obtain a diagnosis.
Such tests remain positive for several days after administration of antibiotics.
Laboratory markers of poor prognosis include low peripheral WBC count, thromobocytopenia, absence of CSF pleocytosis and high CSF protein levels.
Management
- For adult patients penicillin G 5 to 10 million units IV 6 hourly.
- Cephalosporins, i.e. cefotaxime 2 gm IV or ceftriaxone 2 gm IV OD is also effctive.
- Patients allergic to penicillin are treated with chloramphenicol 1 gm IV 6 hourly
- Treatment is continued for 7 to 10 days.
- For raised intracranial tension IV mannitol is given which is accompanied by high doses of dexamethasone 4 mg IV 6 hourly.
The supportive treatment is to maintain nutrition, flid and electrolytic balance.
Question.39.Enumerate fie causes of headache.
Or
Enumerate causes of headache.
Answer. Following are the causes ofheadache:
Intracranial and local extracranial
- Trauma
- Intracranial inflmmations
- Vascular headaches: Hypertension, cerebral or subarachnoid haemorrhage, intracranial aneurysm, vasodilator drugs like nitrites and histamine, adrenaline.
- Traction headache: Pain produced by intracranial arterial displacement and distortion of the dura
- Postlumbar puncture headache: Low CSF pressure headache.
- Cough headache: A benign syndrome of severe headache which accompanies coughing,straining or sneezing can be due to posterior fossa tumor.
- Cranial neuritis and neuralgias of sensory nerves of scalp, e.g. orbital neuralgia, neuralgia of auriculotemporal, posterior auricular or great occipital nerves.
General or systemic causes:
- Anoxemia: Anaemia, carbon monoxide or carbon dioxide poisoning.
- Toxic: Fever, uremia, metallic poisoning,“alcoholic” hangover etc
- Metabolic factors: Hypoglycemia, alkalosis oracidosis
- Hemopoietic factors: Essential polycythemia,thrombasthenia.
Referred pain
- Eyes: Errors of refraction, glaucoma, iritis, etc.
- Ears: Otitis, mastoiditis, vestibular nerve lesions,
Teeth: Impacted teeth, infected tooth sockets and dental roots - Paranasal sinuses: Infection of paranasal sinuses may cause localised pain
- Neck: Diseases of upper cervical spine may be associated with both occipital and frontal pain.
Psychogenic:
- Common Cause Of Headache In Depression.
- Tension (muscle contraction) headache: Pain resulting from sustained contraction of skeletal muscles of the neck, frontalis, occipital muscles due to emotional tension.
- Exertional headache: Headache may come on during exertion and persist for few hours afterwards.
Question.40. Write in brief sign, symptoms and treatment of bacterial meningitis.
Answer.
Following are the causes of meningitis:
- Neonates: E.coli
Children:
- H. inflenzae
- S. pneumoniae
- N. meningitidis.
Adults:
- Young people: Meningococcus
- Older people: S. pneumonia.
Elderly and immunocompromised persons:
- Pneumococcus
- Listeria
- Tuberculosis
- Gramnegative organism
- Cryptococcus.
Viral:
- Enterovirus
- Herpes simplex virus
- Mumps virus
- Inflenza virus
- Japanese encephalitis virus
- Arbo viruses
- Rabies virus
- HIV.
Nosocomial and post-traumatic meningitis:
- Klebsiella pneumonia
- E.coli
- Pseudomonas aeruginosa
- S. aureus.
Meningitis in special situation:
- CSF shunts staphylococcal
- Spinal procedurespseudomonas.
Bacterial Meningitis
Pathophysiology Involves
- Transmission, colonization and invasion of nasopharyngeal epithelium.
- Survival in the blood stream by evading host immune response.
- Meningeal invasion. Bacteremia may be rapidly followed by seeding of meningeal pathogens and secondary infection of the meninges.
- CSF inflmmatory response.
- Cerebral edema and thrombosis.
- Bacterial meningitis causes loss of cerebrovascular anticoagulation.
Clinical Features
Symptoms
- Fever, malaise headache and vomiting.
- Pain over the neck
- Stiffess over the neck
- Confusion, delirium and coma.
Signs
- Kernig’s sign is positive.
- Neck rigidity, i.e. when neck is bended there is presence of pain and there is spasm of neck muscles.
- Brudzinski’s sign is also positive.
- Photophobia is present
- Cranial nerve palsies most commonly IIIrd, IVth, VIth and VIIth.
- Focal neurological defiits such as nystagmus, aphasia, ataxia and peripheral nerve palsies.
- Partial or generalized seizures tend to be more common in Strep. pneumoniae and HIV meningitis.
- Purpura or petechiae in meningococcal meningitis, with or without features of septic shock.
Diagnosis
- Examination of CSF
Typical CSF fidings in acute bacterial meningitis: - Raised WBC count (usually 100–60,000 cells/mL (predominantly neutrophils)
- Reduced CSF glucose (30–40% serum glucose level)
- Raised CSF protein (0.5–5 g/L)
- Gramstaining of CSF is positive in over 90% of cases of hematologically acquired meningitis.
- Blood culture should be performed in all patients with suspected meningitis, and latex agglutination bacterial antigen test or polymerase chain reaction analysis (to detect bacterial DNA) may be performed on blood or CSF to try to obtain a diagnosis.
Such tests remain positive for several days after administration of antibiotics.
Laboratory markers of poor prognosis include low peripheral WBC count, thromobocytopenia, absence of CSF pleocytosis and high CSF protein levels.
Management
- For adult patients penicillin G 5 to 10 million units IV 6 hourly.
- Cephalosporins, i.e. cefotaxime 2 gm IV or ceftriaxone 2 gm IV OD is also effctive.
- Patients allergic to penicillin are treated with chloramphenicol 1 gm IV 6 hourly
- Treatment is continued for 7 to 10 days.
- For raised intracranial tension IV mannitol is given which is accompanied by high doses of dexamethasone 4 mg IV 6 hourly.
The supportive treatment is to maintain nutrition, flid and electrolytic balance.
“Role of diagrams in understanding nervous system anatomy: Questions answered”
Question.41. Enumerate causes of meningitis and describe clinical features, complications and treatment of tubercular meningitis.
Answer.
Following are the causes of meningitis:
- Neonates: E.coli
Children:
- H. inflenzae
- S. pneumoniae
- N. meningitidis.
Adults:
- Young people: Meningococcus
- Older people: S. pneumonia.
Elderly and immunocompromised persons:
- Pneumococcus
- Listeria
- Tuberculosis
- Gramnegative organism
- Cryptococcus.
Viral:
- Enterovirus
- Herpes simplex virus
- Mumps virus
- Inflenza virus
- Japanese encephalitis virus
- Arbo viruses
- Rabies virus
- HIV.
Nosocomial and post-traumatic meningitis:
- Klebsiella pneumonia
- E.coli
- Pseudomonas aeruginosa
- S. aureus.
Meningitis in special situation:
- CSF shunts staphylococcal
- Spinal procedurespseudomonas.
Clinical Features
Symptoms
- Fever coming with rigors.
- Headache which is very severe (bursting in character) mainly in frontal region radiating down to back.
- Vomiting
- Convulsion in children
- Malaise
- Severe photophobia
- Ptosis: Due to raised intracranial tension
- Stiffess in neck and back
- Pain in neck
- Impairment of consciousness i.e. confusion, delirium and coma.
Signs
- Head retraction is present in infants and children.
- Neck rigidity, i.e. bending of neck causes pain and spasm of neck muscles or it is diffilt to bend the neck.
- Kernig’s sign is positive
- Brudzinski’s sign is also positive if patient is conscious.
- Presence of papilledema
- Presence of cranial nerve palsies
Clinical Features Of Tuberculous Meningitis
Symptoms
- Headache
- Vomiting
- Low grade fever
- Lassitude, i.e. weariness or exhaustion
- Depression
- Confusion
- Behavior changes.
Signs
- Meningism may be present
- Occulomotor palsies
- Papilledema
- Depression of conscious level
- Focal hemisphere signs.
Management of Tubercular Meningitis
General management:
- Maintenance of nutrition, hydration and electrolyte balance.
- Case of bowel and bladder
- Nursing should be good
- If there are convulsions, anticonvulsants are given.
Complications
- Infection spreads in parenchyma of brain causing meningoencephalitis.
- Involvement of cerebral vessel causes obliterative endarteritis
- Thrombosis of cerebral vessels lead to cerebral infarction
- Delayed complications are development of hydrocephalus optic atrophy, spinal cord compression and cranial nerve palsy.
“Can advanced tools supplement nervous system disease exam preparation? FAQs provided”
Question.42. Write notes on facial pain.
Answer.
Various number of conditions are involved in the pain localized to face.
These may range from pain arising from diseases of teeth, gums, sinuses, temporomandibular joint to various causes.
Facial neuritis
- It is a form of inflmmation of the nerve of the face and scalp.
- It generally occurs as a complication of a septicemic estate or due to involvement by a neurotropic virus.
- Onset is usually acute and pain is confied to the face and scalp, occurring in paroxysms lasting for several hours and very often till the end of the day when the patient is exhausted.
- If the character ofpain is dull aching which is intensifid by exposure to cold and often occurs in the form of shooting pains in the distribution of the nerve.
Sometimes the pain is so severe that the patient is unable to sleep. - Physical examination shows presence of hyperalgesia in the distribution of nerves including face and scalp.
Nerve trunk is tender on pressure.
Myofascial Pain
- It is a form of dull constant pain with local tenderness of the muscles of jaw.
- There is often pain and diffilty in opening the mouth.
- This pain is related to bad and improper habits of clenching and grinding of teeth. This type of habit is present amongst hysterical persons especially women who often clench and grind their teeth.
- There is no physical fiding in such people except that these people have an emotionally labile personality and often suffr from depression.
- Treatment consists in giving them assurance, analgesics and tricyclic antidepressants.
Trigeminal Neuralgia
Trigeminal neuralgia is also called as Tic Douloureux.
A disorder characterized by the *paroxysmal attcks of neuralgic pain with affction of one or more division of trigeminal nerve.
The pain involves the third and second divisions equally and rarely the fist.

“Asymptomatic vs symptomatic effects of outdated study methods: Answered”
Differential Diagnosis Of Facial Pain
Symptomatic trigeminal neuralgia
- Neuralgia indistinguishable from the idiopathic variety may occur as a result of compression of trigeminal root or ganglion, e.g. meningioma, acoustic neuroma, aneurysm of basilar artery, arteriovenous malformations, basilar invagination, epidermoid cholesteatomas in the cerebellopontine angle, as a result of Paget’s disease or osteomalacia.
- Paratrigeminal neuralgia (Raeder’s syndrome): Severe pain in and around one eye accompanied by Horner’s syndrome on the affcted side.
It is continuous and progressive and is usually caused by a structural lesion, often malignant in the base of the skull involving the paratrigeminal region. - Multiple sclerosis: Diagnosis of multiple sclerosis should always be suspected in a young patient with trigeminal neuralgia.
- Syringobulbia.
- Painful superior orbital fisure syndrome (TolosaHunt syndrome) caused by granulomatous tissue involving nerves III, IV and VI. Pain with development of ocular palsies and loss of fist division trigeminal sensation.
- Referred pain: Paranasal sinuses, toothache, aural infection.
Temporomandibular joint dysfunction (Costen’s syndrome) - abnormality of bite and aggravated by chewing.
Vascular pain:
- Migraine: Episodes of severe and continuous pain,often burning in character in or behind one eye, or in cheek, forehead and temple.
Often suffsion of conjunctiva and blocking of nostril on that side. - Temporal arteritis: Pain of dull, throbbing nature with associated scalp tenderness.
Thickened temporal arteries with reduced or absent pulsations.
Other neuralgias
- Post-herpetic neuralgia: Pain is continuous in nature.
Vesicles and scars of herpetic infection. - Glossopharyngeal neuralgia: Pain in tonsillar fossa, back of throat and larynx; may radiate to ear on affcted side. Swallowing is the stimulus most likely to produce pain.
Atypical facial pain
Intermittnt but long lasting pain of aching character which affcts the cheek and upper jaw, often bilateral and occurs almost exclusively in young and middle—aged women.
Generally believed to be a manifestation of depression or anxiety.
Miscellaneous
- Clonic facial spasm: Sometimes painful, usually associated with intermittent twitching of eyelid and face on one side.
- Platysma usually involved in twitching.
- Neuralgic pain: Occasionally associated with facial hemiatrophy.
- Idiopathic trigeminal neuropathy: It is commonly associated with muscle wasting of masseter.
“Early warning signs of poor performance in nervous system disease exams: Common questions”
Question.43. Write short note Grand-mal epilepsy.
Answer. It is a type of a primary generalized seizure.
- It is a true seizure.
- It is also known as tonic clonic seizure.
- Grand mal epilepsy comes suddenly without warning in some patients while in others it is preceded by various phases or symptoms.
- Following are the phases:
- Prodromal phase: In this phase patient become uneasy and irritable for some hours to days before an attck.
- Aura: It is seen when partial seizure become generalized so the symptoms of partial seizures such as flashing of light, hallucination of
hearing words or sounds, Tingling or numbness sensation, pain in epigastrium and unnatural sensations in some part of the body. Aura is
warning of an attack and is produce by an activation of epileptic discharge in brain. It remains for some seconds or minutes. - Tonic clonic phase: Tonic convulsions of two side of body occur with head and eyes rotated to one side. Tonic Phase occur for 10–30 seconds and there is presence of flxion of arms, tonic contraction of muscles, a cry due to spasm of respiratory muscles and extension of legs. Tonic phase is followed by clonic phase which last for 1–5 minutes. In clonic phase there is violent jerking of face and limbs, biting of tongue and passing of urine and stools. Clonic phase is followed by unconsciousness which lasts for few minutes to half an hour.
- Postictal phase: This phase last for few minutes to hours. There is presence of unconsciousness with flccid limbs, corneal reflxes are lost and plantar extensor response may occur during this phase. In this patient has severe headache,confusion and automatic behavior.
Diagnosis Of Grand Mal Epilepsy
- Diagnosis of grand mal epilepsy is made by careful assessment of patient’s history documented by the diagnostic studies.
- These include blood test to assess for the metabolic disarray, brain imaging using MRI or CT scan and EEG. Normally EEG shows series of small alpha waves about 10per second and occasionally small beta waves,but during attck in Grand mal epilepsy series of sharp spikes is present. Between the attcks 3 Hz 5W interictal epileptiform activity there is presence of intermittnt irregular slow waves in grand mal epilepsy.
- It also depends upon its onset and symptoms like biting of tongue, passing of urine in clothes, injury to the patient,loss of consciousness and postepileptic features.
Management
Immediate treatment of an attck of fit.
- Patient should be protected from the injury. He should be moved away from fie and sharp and hard object.
- Padded mouth gag is inserted between the teeth to avoid tongue injury.
- Clear airway should be maintained.
- Diazepam 5 to 10 mg slow IV injection is given.
“How do case studies enhance comprehension of nervous system disease complications? FAQ explained
Long-term drug therapy.
- Phenytoin sodium 200 to 400 mg daily.
- Carbamazepine 600 to 1800 mg daily in divided dose.
- Sodium valproate 0.25 to 1 mg daily.
- Phenobarbitone 60 to 180 mg daily.
- Primidone 750 to 1500 mg daily in divided dose.
Social and psychological aspects.
- Patients and relatives should be told about the illness,its precipitating factors and consequences.
- Restriction should be in children as they are more likely to be in danger. Cycling, driving and swimming is avoided.
- Patient should be advised to take occupation in which neither he nor the community is on risk.
Leave a Reply