Stomach Important Question And Answers
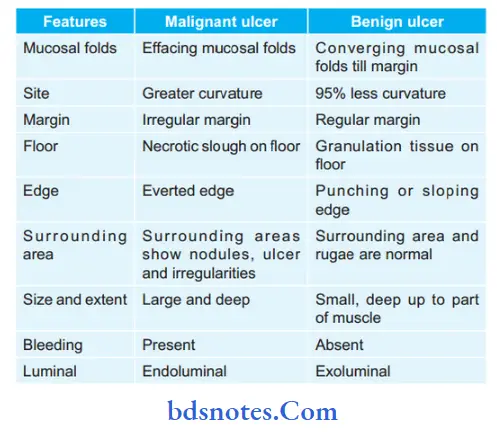
Question 1. How we differentiate between malignant and benign ulcers and management?
Answer. Benign ulcers and malignant ulcers are the types of gastric ulcers.
“Understanding The Causes Of Stomach Pain“
Management of Benign ulcer
Drugs like H2 blockers, proton-pump inhibitors, and carbenoxolone (biogas trone, sucralfate, and prostaglandins which coat the ulcer and so create a mucosal barrier) help in reducing or eliminating the symptoms of benign ulcer.
Management of Malignant ulcer
- However asymptomatic ulcers may exist silently and may turn into malignancy. So surgery is the preferred line of treatment.
Partial gastrectomy and Billroth I gastroduodenal anastamosis is done. - Type IV proximal gastric ulcer is difficult to manage.
Read And Learn More: General Surgery Questions and Answers
“Effective Ways To Manage Stomach Bloating At Home”
- It is treated by subtotal gastrectomy. Often distal gastrectomy
with a selective sleeve-like extension cut along the lesser curve to remove the ulcer is done—Pauchet’s procedure. - Other surgical procedures:
“Step-By-Step Guide To Managing Acid Reflux”
- de Miguel’s antrectomy: Distal antrectomy, pleurectomy with excision of ulcer along with gastroduodenal anastomosis is done.
It preserves gastric reservoir function, shows less recurrence rate, and less operative morbidity. - Maki’s pylorus-preserving gastrectomy: Hemigastrectomy with excision of the pyloric ulcer but retaining 2 cm pre-pyloric stomach. It is only used in type l gastric ulcers.
Even though it has fewer incidences of postoperative diarrhea and dumping, it has got high recurrence rate.
“Tips To Prevent Stomach Ulcers Naturally”
- HSV with excision of the ulcer
- Kelling Madlener procedure: It is an antrectomy and excision of proximal gastric ulcer Type IV.
- Csendes procedure: It is subtotal gastrectomy with sleeve extended resection along the lesser curve for type IV proximal gastric ulcer.
Leave a Reply