Understanding Shock: Classification, Causes, Clinical Features, and Management Strategies
Answer. Shock is defined as an acute clinical syndrome characterized by a significant, systemic reduction in tissue perfusion, resulting in decreased tissue oxygen delivery and insufficient removal of cellular metabolic products, resulting in tissue injury and severe dysfunction of vital organs.
Read And Learn More: General Surgery Questions and Answers
Classification of Shock
Following is the classification of shock:
- Hypovolemic shock
- Cardiogenic shock
- Distributive shock:
“Understanding The Classification Of Shock“
- Septic shock
- Anaphylactic shock
- Neurogenic shock
- Obstructive shock.
Hypovolemic Shock
- Hypovolemic shock occurs due to loss of blood plasma or bodyfluidd and electrolytes, usually caused by massive hemorrhage, vomiting, diarrhea, and dehydration.
- Hypovolemic shock is the most common type of sho,ck which is characterized by a loss in circulatory volu me, which leads to decreased venous return, decreased filing of the cardiac chambers, and so therea is decreased in cardiac output, which leads to an ncrease in systemic vascular resistance.
Cardiogenic Shock
- Cardiogenic shock occurs due to the dysfunction of one ventricle or another.
- This type of shock is seen in myocardial infarction, chronic congestive cardiac failure, cardiac arrhythmias, pulmonary embolism, etc.
Resulting in inability of the heart to pump the adequate amount of blood into the lungs and decreased cardiac output. - Myocardial infarction is the most common cause of cardiogenic shock.
“Step-By-Step Guide To Managing Shock”
Distributive Shock
Distributive shock occurs when the afterload is excessively reduced due to extensive vasodilatation and is associated with not
only with poor vascular tone in the peripheral circulation but also with maldistribution of blood flow to organs within the body.
- Septic shock: This type of shock is mostly due to the release of endotoxins in blood, which causes widespread vasodilation of blood vessels, resulting ina fall in the cardiac output.
Bacteria responsible for the release of endotoxins are E. coli, Pseudomonas proteus, etc. It is the most common shock among
all the distributive shocks.
“What Are The Complications Of Untreated Shock”
- Neurogenic shock: This type of distributive shock is caused by the suppression or loss of sympathetic tone caused by any disruption of the sympathetic nervous system, like spinal injury, spinal anesthesia, and drugs.
- Anaphylactic shock: This type of shock is a result of type I hypersensitivity reaction and is caused when the body’s antibody-antigen response is triggered by something the person is allergic to drugs, like penicillin, cephalosporins, iodinated contrast media, serum, etc., are common causes of this type of shock.
“Tips To Stabilize A Patient In Shock”
Obstructive Shock
- This type of shock is associated with physical obstruction of the great vessels or the heart itself.
- Most commonly, obstructive shock is due to cardiac tamponade, tension pneumothorax, and pulmonary embolus.
Causes of Shock
Hypovolemic shock—due to reduction in total blood volume.
It may be due to:
- Hemorrhage:
- External from wounds, open fractures
- Internal from injury to the spleen, liver, mesentery, or pelvis.
- Severe burns, which results in loss of plasma
- Peritonitis, intestinal obstruction
- Vomiting and diarrhea of any cause
Shock Cardiac causes:
- Acute myocardial infarction, acute carditis
- Acute pulmonary embolism wherein embolus blocks the pulmonary artery at bifurcation or one of the major branches
- Drug-induced
- Toxemia of any causes
- Cardiac surgical conditions like valvular diseases ,congenital heart diseases
- Cardiac compression causes:
- Cardiac tamponade is due to the collection of blood, pus, and fluid in the pericardial space,e which prevents the heart from expanding, leading to shock.
- Trauma to heart.
- Septic shock—is due to bacterial infections which release toxins leading to shock.
- Neurogenic shock—due to sudden anxious or painful stimuli causing severe splanchnic vessel vasodilatation.
Her, thee patient either goes for cardiac arrest and dies or recovers fully spontaneously—spinal cord injury/anesthesia
can cause neurogenic shock. - Anaphylactic shock—is due to a type I hypersensitivity reaction
“Comprehensive Overview Of Shock Types”
Shock Respiratory causes:
- Atelectasis (collapse) of the lung
- Thoracic injuries
- Tension pneumothorax
- Anesthetic complications.
Shock Other causes:
- Acute adrenal insufficiency (Addison’s disease)
- Myxedema.
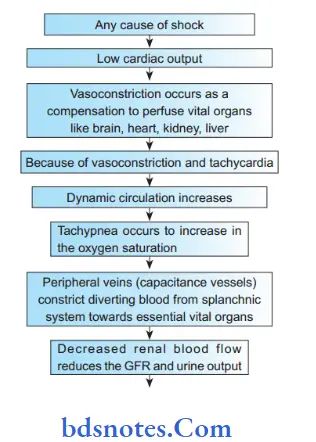
Pathophysiology of Shock
“Can Stress Cause Shock In The Body”

“Best Practices For Shock Treatment In Hospitals”
Stages of Shock
Stage l: Stage of compensatory shock—by the neuroendocrine response to maintain the perfusion of the vital organs like the brain, heart, kidney, and liver.
Stage 2: Stage of decompensatory shock—where there is progressive shock causing persistent shock with severe hypotension (with mean arterial pressure <65 mm Hg); oliguria, tachycardia.
Stage 3: Stage of irreversible shock – with severe hypoxia and Multi-organ dysfunction syndrome (MODS).
Clinical Features of Shock
- Presence of anxiety, restlessness, altered mental state due to decreased cerebral perfusion and subsequent hypoxia.
- Hypotension because of a decrease in circulatory volume.
- Due to decreased blood flow,w there is tachycardia and weak thready pulse.
- Cold and clammy skin due to vasoconstriction and stimulation of vasoconstriction.
- Rapid and shallow respirations (tachypnea) due to sympathetic nervous system stimulation and acidosis.
- Hypothermia due to decreased perfusion and evaporation of sweat.
- Thirst and dry mouth due to tfluidid depletion.
- Fatigue due to inadequate oxygenation.
- Cold amottled skin, especially extremities, due to insufficient perfusion of the skin.
- Pallor is present
- Fainting
- Oliguria/anuria due to decreased renal perfusion and afferent arteriolar vasoconstriction.
Investigations and Monitoring of Shock
- Regular monitor with blood pressure, pulse, heart rate, respiratory rate, and urine output measurement (hourly) should be done.
Urine output should be more than 0.5 ml/kg/hour.
Pulse oximetry should be used. - Central venous pressure (CVP) and ulmonary capillary wedge pressure (PCWP—an accurate assessment of left ventricular/function) monitoring should be done.
ICU care is needed during the monitor period.
However, both CVP and PCWP are not accuratemethodsd of assessing tissue perfusion. - Complete blood count, ESR, pH assessment, serum electrolyte estimation, and chest X-ray (to rule out acute respiratory distress syndrome/pulmonary problems).
- Pus/urine/blood/bile/sputum cultures depending on the focus and need in sepsis.
- Serum lactate estimation is an important prognostic factor.
Level >2 mEq/L suggests tissue ischemia. - USG of a part, CT/MRI of the location of the pathology of standard focus should be done; often, it may require repetition of this imaging to assess progress.
- Blood urea, serum creatinine, liver function tests, prothrombin time (PT), activated partial thromboplastin time (APTT), and ECG monitoring are also should be done.
- All these tests, including platelet count and arterial blood gas (ABG), should be repeated at regular intervals.
“The Role Of Fluids In Shock Management“
Treatment Of Shock
- Treat the cause, e.g., arrest hemorrhage, drain pus.
- Fluid replacement: Plasma, normal saline, dextrose, Ringer’s lactate, plasma expander (hemocoel).
The dosage is the maximum of l liter that can be given in 24 hours.
Initially, crystalloidsand then colloids are given.
Blood transfusion is done whenever required.
“Can Medications Reverse Shock Symptoms”
- Ionotropic agents: Dopamine, dobutamine, adrenaline infusions—mainly in distributive shock like septic shock.
- Correction of acid-base balance: Acidosis is corrected by using 8.4% sodium bicarbonate intravenously.
- Steroidsares often lifesaving. 500–l000 mg of hydrocortisone can be given. Itimprovese perfusion,and reducee capillary leakage and systemic inflammatory effects.
- Antibiotics in patients with sepsis; proper control of blood sugar and ketosis in diabetic patients.
- Catheterization to measure urine output (30–50 mL/hour or > 0.5 mL/kg/hour should be maintained).
- Nasal oxygen to improve oxygenation or ventilator support with intensive care unit monitoring has to be done.
- Central venous pressure line to perfuse adequately and to monitor fluid balance. Totalparenterall nutrition is given when required.
“Effective Strategies For Preventing Shock”
- Pulmonary capillary wedge pressure to monitor very criticapatientsnt.
- Hemodialysis may be necessarywithe en kidneys are not functioning.
- Control pain—using morphine (4 mg IV).
- Ventilator and ICU/critical care management.
- Injection ranitidine IV or omeprazole IV or pantoprazole IV.
- Activated protein, even though costly,y is beneficial as it prevents the release and action of inflammatory response.
- MAST(MilitaryAnti-shock Trouser) provides circumferential external pressure of 40 mm Hg.
Lt is wrapped around lower limbs and abdomen and iinflatedwith required pressure. It redistributes the existing blood and flid towards the center.
It should be deflated carefully and gradually.
Leave a Reply