Neoplasm Notes
“What is a neoplasm and why does it matter?”
Procarcinogens
Procarcinogens are also called indirect-acting carcinogens.
Procarcinogens are chemical substances that require prior metabolic activation before becoming potent ‘ultimate’ carcinogens. This group includes the vast majority of carcinogenic chemicals,
It includes the following 4 categories:
1. Polycyclic aromatic hydrocarbons: These consist of the largest group of common procarcinogens which, after metabolic activation, can induce neoplasia in many tissues in experimental animals and are also implicated in a number of human neoplasms.
They cause different effects by various modes of administration. The main sources of polycyclic aromatic hydrocarbons are the combustion and chewing of tobacco, smoke, fossil fuel (e.g. coal), soot, tar, mineral oil, smoked animal foods, and industrial and atmospheric pollutants.
neoplasm notes
Important chemical compounds included in this group are anthracenes (Benza-, dibenzo-, dimethylbenza-), benzopyrene, and methylcholanthrene. The following examples have evidence to support the etiologic role of these substances:
“Understanding the role of neoplasms in health and disease”
- Smoking and lung cancer: There is a 20 times higher incidence of lung cancer in smokers of 2 packs (40 cigarettes) per day for 20 years.
- Skin cancer: Direct contact of polycyclic aromatic hydrocarbon compounds with skin is associated with a higher incidence of skin cancer.
- Tobacco and betel nut chewing and cancer oral cavity: Cancer of the oral cavity is more common in people chewing tobacco and betel nuts.
“How do neoplasms develop and affect the body?”
“Importance of studying neoplasms for better healthcare outcomes”
2. Aromatic amines and azodyes: This category includes the following substances implicated in chemical carcinogenesis:
- β-naplithylarnine in the causation of bladder cancer, especially in aniline dye and rubber industry workers.
- Benzidine in the induction of bladder cancer.
- Azo-dyes are used for coloring foods (for example, butter and margarine to give them yellow color, scarlet red for coloring cherries, etc.) in the causation of hepatocellular carcinoma.
3. Naturallyoccurringproducts: Some of the important chemical carcinogens derived from plant and microbial sources are aflatoxin B1, actinomycin D, mitomycin C, safrole, and betel nuts. Out of these, aflatoxin Bl implicated in causing human hepatocellular carcinoma is the most important, especially when concomitant viral hepatitis B is present.
4. Miscellaneous: A variety of other chemical carcinogens having a role in the etiology of human cancer are as under:
“Common challenges in diagnosing and managing neoplasms”
- Nitrosamines and nitrosamines are involved in gastric carcinoma. These compounds are actually made in the stomach by nitrosylation of food preservatives.
- Vinyl chloride monomer derived from polyvinyl chloride (PVC) polymer in the causation of haemangiosarcoma of the liver.
- Asbestos in bronchogenic carcinoma and mesothelioma, especially in smokers.
- Arsenical compounds in causing epidermal hyperplasia and basal cell carcinoma.
- Metals like nickel, lead, cobalt, chromium, etc in industrial workers cause lung cancer.
- Insecticides and fungicides (For example, Aldrin, dieldrin, chlordane) in carcinogenesis in experimental animals.
- Saccharin and cyclamates in cancer in experimental animals.
“Steps to identify common types of neoplasms”
Burkitt’s Lymphoma
Burkitt’s lymphoma is also known as African jaw lymphoma. It is a high-grade tumor and is a very rapidly progressive human tumor.
Burkitt’s Lymphoma Etiology:
It is caused by Epstein-Barr Virus (EBV) infection in B lymphocytes. EBV stimulates B lymphocytes to proliferate.
Burkitt’s Lymphoma Types:
Three subgroups of Burkitt’s lymphoma are recognized, i.e. African endemic, Sporadic, and immunodeficiency-associated.
1. African endemic: It was first described in African children. It predominantly presents as a jaw tumor that spreads to extranodal sites, i.e. bone marrow and meninges
2. Sporadic Burkitts lymphoma: In this tumor cells are similar to those of Burkitt’s lymphoma but are more pleomorphic and may sometimes be multinucleated. This variety has the propensity to infiltrate CNS and is more aggressive than true Burkitt lymphoma.
“Role of benign tumors in non-cancerous growths”
3. Immunodeficiency associated with Burkitt’s lymphoma: It includes cases seen in association with HIV infection.
Burkitt’s Lymphoma Clinical Features:
- Mostly occur in children from 6 to 9 years of age.
- Males are affected more often than compared to females.
- The growth of the tumor is very rapid and it grows double the time in 24 hours.
- Mostly extranodal sites are involved, i.e. jaw, gastrointestinal tract, and gonads.
- Peripheral lymphadenopathy is common.
- In African patients, there is the involvement of mandibular and maxillary bones which manifest with deformity, loosening of teeth, and proptosis with loss of vision.
- In the North American type abdomen is involved.
“How do malignant neoplasms differ from benign ones?”
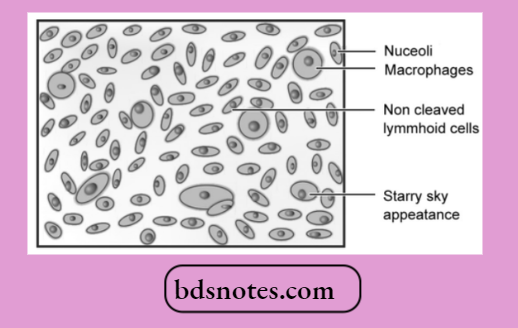
Burkitt’s Lymphoma Histopathology
- In Burkitts lymphoma tumor cells are intermediate in size, noncleaved, and homogeneous in size and shape.
- The nuclei are round or oval and contain 2-5 nucleoli.
- The cytoplasm is basophilic and contains lipid vacuolation.
- The tumor cells have a very high mitotic rate and therefore there is high cell death.
- There is the presence of numerous macrophages background of this tumor containing phagocytosed tumor debris giving a starry sky appearance.
- So the classical appearance of Burkitt’s lymphoma is of monomorphic medium-sized cells having round nuclei, frequent mitosis, multiple nucleoli, and basophilic cytoplasm with vacuoles.
“Early warning signs of untreated neoplasm conditions”
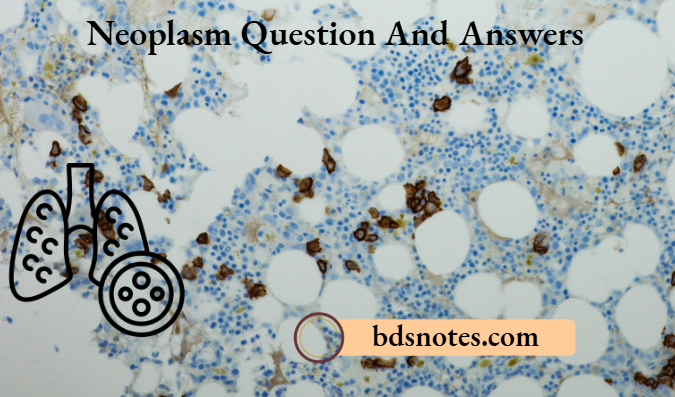
Burkitt’s Lymphoma Laboratory Findings
- Immunohistochemistry: Tumor cells are positive for CD19 and CD10 antibodies as well as surface immunoglobulin IgM.
- Chromosome analysis may show 8; 14 or 2; 8 or 8; 22 translocations. Most translocations fuse MYC with the IgH gene on chromosome 14 resulting in dysregulation and overexpression of the MYC protein.
DNA Oncogenic Viruses
Oncogenic viruses are associated with neoplasm.
- DNA oncogenic viruses have direct access to the host cell nucleus and are incorporated into the genome of the host cell DNA.
- Oncogenic viruses are classified into five subgroups:
- Papova virus
- Herpes virus
- Adenovirus
- Poxvirus
- Hepadna virus.
“Asymptomatic vs symptomatic stages of neoplasm progression”
DNA oncogenic viruses Papova Virus (Human Papilloma Virus):
These viruses appear to replicate in the layers of stratified squamous epithelium.
It is responsible for:
- Skin warts (squamous cell papillomas)
- Invasive cervical cancer
- Condyloma acuminate
- Other squamous cell carcinomas.
DNA oncogenic viruses Herpes Viruses
- EbsetinBarr virus: EBV infects human B lymphocytes and stimulates them to proliferate and cause Burkitt’s lymphoma, Hodgkin’s lymphoma, and primary lymphoma in AIDS patients.
- HV8 (Human Herpes virus 8): It is responsible for Kaposi’s sarcoma, a vascular neoplasm common in patients with AIDS, and also responsible for B cell lymphoma.
DNA oncogenic viruses Adenovirus
The human adenovirus causes upper respiratory tract infection and pharyngitis. In humans, they are not known to be involved in any tumor.
DNA oncogenic viruses Pox Viruses
In humans, they cause molluscum contagiosum and may include squamous cell papilloma.
DNA oncogenic viruses Hepadna Viruses
The Hepatitis B virus comes into this category. It causes acute hepatitis and chronic hepatitis.
“Can targeted interventions reduce risks of severe neoplasms?”
Malignancies Related to Tobacco
Tobacco plays an important role in the development of oral cancer. It also causes cancer of the pharynx, larynx, esophagus, lungs, etc.
- Tobacco is used in smoking forms like cigarettes, cigars, pipes, bidis, etc.
- It can also be used in smokeless forms like snuff, tobacco sachets, and other forms.
- Several supportive pieces of evidence can establish the relationship between the use of tobacco and the occurrence of oral cancer.
- Studies indicate that the incidence of oral cancer is four times greater among pipe or cigar smokers as compared to non-smokers.
- Pipe and cigarette smoking has been linked with carcinoma of lips for many years.
- Different studies also indicate that people who are smoking 40 or more cigarettes per day have a significantly increased risk of oral cancer (about 10 to 20 times) more than that of non-smokers.
- The habit of reverse smoking (if the burning end of the cigarette is put inside the mouth while smoking) definitely increases the risk of oral cancer.
- Research indicates that tobacco contains polycyclic aromatic hydrocarbons in tobacco smoke which have serious carcinogenic effects.
- Other carcinogenic agents in tobacco are nitrosamine, nicotine, carbon monoxide, phenol, and benzopyrene.
- These carcinogenic agents play an important role in the transformation of normal mucosal epithelial cells to squamous cell carcinoma.
“Steps to educate patients about neoplasms and their risks”
Histopathological Changes of Malignant Tumors
The term ‘neoplasia’ or ‘tumor’ means new growth produced.
Definition: A mass of tissue formed as a result of abnormal, excessive, uncoordinated, autonomous, and purposeless proliferation of cells.
Malignant Tumors: Malignant tumors grow rapidly may ulcerate on the surface, invade locally in the deeper tissue, and may spread to distant sites.
Malignant Tumors Histopathological Changes:
Malignant cells show anaplasia (lack of differentiation). It is the characteristic feature of most malignant tumors.
Morphological and functional alteration in neoplastic cells
“Role of counseling in improving awareness of tumor types”
- Loss of polarity: In malignancy, the tumor cells lose their basal polarity so that the nuclei tend to lie away from the basement membrane.
- Pleomorphism: The tumor cells show variation in shape and size.
- Nuclearcytoplasmic ratio—nuclei are enlarged disproportionately to the cell size so that the nuclear: cytoplasmic ratio is increased from normal 1:5 to 1:1.
- Anisonucleosis: Nuclei also show variation in size and shape in malignant tumor cells.
- Hyperchromatism: The nuclear chromatin of malignant cells is increased and coarsely clumped.
- Nucleolar changes: Malignant cells frequently have a prominent nucleolus or nucleoli in the nucleus reflecting increased muscle protein synthesis.
- Mitotic figures: Parenchymal cells of poorly differentiated tumors often show a large number of mitosis. Abnormal or atypical mitotic figures are more important in malignant tumors.
- Tumor giant cells: Multinucleated tumor giant cells or giant cells containing a single large and bizarre nucleus, possessing nuclear characters of adjacent tumor cells.
- Functional (cytoplasmic) changes: Structural anaplasia in tumors is accompanied by functional anaplasia as appreciated by cytoplasmic constituents of tumor cells, for example, Keratin formation in well-differentiated squamous cell carcinoma.
- In more anaplastic tumors there is a fall in the product made by the tumor cells, i.e. keratin is absent in anaplastic squamous cell carcinoma.
Oncogenes and Antioncogenes in Carcinogenesis
Role of Oncogenes in Carcinogenesis The Mutated form of normal proto-oncogenes in cancer is called as oncogenes. Oncogenes differ from normal genes in the following respects:
- Mutation in the structure of the gene
- Lacking the normal growth-promoting signals of protooncogenes
- They act by over-expression to promote autonomous and excessive cellular proliferation.
“Can interactive tools improve adherence to neoplasm care plans?”
Activation of oncogenes in human tumors can occur by the following mechanisms:
- Point mutations and deletion: The most important example is RAS oncogene carried in many human tumors such as bladder cancer, and pancreatic adenocarcinoma.
- Chromosomal translocation: The mechanism of transfer of a portion of one chromosome to another is implicated in the pathogenesis of leukemias and lymphomas, for example, the Philadelphia chromosome is seen in 95% of cases of chronic myelogenous leukemia in which c-ABL proto-oncogene on chromosome 9 is translocated to chromosome 22.
- Gene amplification: Chromosomal alterations that increase the number of copies of a gene are found in some examples of solid human tumors, e.g. neuroblastoma having n-MYC HSR region.
The steps in signal transduction for cell proliferation by oncogenes are discussed about mitosis in the normal cell cycle:
- Growth factors:
- These are polypeptides elaborated by many cells and normally act on another cell than the one which synthesized it to stimulate its proliferation, i.e. paracrine action.
- However, a cancer cell may synthesize growth factor and respond to it as well; this way cancer cells acquire growth self-sufficiency.
- Receptors for growth factors:
- Many oncogenes encoding for growth factor receptors have been described which act more commonly by overexpression of normal growth factor than by mutation.
- For example, ERB1 is an EGF receptor that acts by overexpression of normal growth factor receptors in squamous cell carcinoma.
- Signal transduction proteins:
- The normal signal transduction proteins which transduce signals from the growth factor receptors on the cell surface to the nucleus of the cell mutated in some cancers.
- Examples of such oncogenes are mutated RAS genes. This is the most common form of oncogene in human tumors.
“Asymptomatic vs symptomatic effects of poor communication”
- Nuclear regulatory molecules:
- The signal transduction pathway that starts with growth factors ultimately reaches the nucleus where it regulates DNA transcription.
- Out of the various nuclear regulatory transcription proteins described, the most important is the MYC gene, seen most commonly in human tumors.
- Normally MYC protein binds to the DNA and regulates the cell cycle by transcriptional activation and its levels fall immediately after the cell enters the cell cycle.
- MYC oncogene, on the other hand, is associated with persistent or overexpression of MYC oncoproteins which, in turn, causes autonomous cell proliferation.
- An example of tumors carrying MYC oncogene is Burkitt’s lymphoma in which mutation in the MYC gene is due to translocation t(8;l4).
- Cell cycle regulatory proteins:
- The cell cycle is under the regulatory control of cyclins and cyclin-dependent kinases (CDKs) A, B, E, and D.
- Cyclins are so named since they are cyclically synthesized during different phases of the cell cycle and their degradation is also cyclic.
- Cyclins activate as well as work together with CDKs, while many inhibitors of CDKs are also present.
- Although all steps in the cell cycle are under regulatory control, the G1→S phase is the most important checkpoint for regulation by oncogenes as well as anti-oncogenes.
Role of Anti-oncogenes in Carcinogenesis
The mutation of normal growth suppressor anti-oncogenes results in the removal of the brakes for growth thus the inhibitory effect on cell growth is removed and the abnormal growth continues unchecked. In other words, mutated anti-oncogenes behave like growth-promoting oncogenes.
Major anti-oncogenes implicated in human cancers are as under:
- RB gene:
- It is located on the long arm (q) of chromosome 13. This is the first-ever tumor suppressor gene identified.
- Normally RB gene product is a nuclear transcription protein that is virtually present in every human cell. It exists in both an active and inactive form.
- Active RB gene protein acts to inhibit the cell cycle at the G1 → S phase.
- Stimulation of the cell by growth factors renders the RB gene protein inactive and thus permits the cell to cross the Gl → S phase. The mutant form of the RB gene is involved in retinoblastoma, the most common intraocular tumor in young children.
- TP53 gene (p53): Located on the short arm (p) of chromosome 17, the p53 gene is normally a growth suppressor anti-oncogene.
The two major functions of TP53 in the normal cell cycle are as under:
- In blocking mitotic activity: TP53 inhibits the cyclins and CDKs and prevents the cell from entering the G1 phase transiently. This breathing time in the cell cycle is utilized by the cell to repair the DNA damage.
- In promoting apoptosis: TP53 acts together with another anti-oncogene, the RB gene, and identifies the genes that have damaged DNA that cannot be repaired by an inbuilt system.
- TP53 directs such cells to apoptosis by activating the apoptosis-inducing BAK gene, thus bringing the defective cells to an end.
- This process operates in the cell cycle at Gl and G2 phases before the cell enters the S or M phase. Because of these significant roles in the cell cycle, TP53 is called a ‘protector of the genome’. In its mutated form, TP53 stops to act as a growth suppressor and instead acts like an oncogene, c-onc.
- The majority of human cancers have either a mutation in TP53 or its expression is up or, downregulated. Some common examples of human cancers having defective TP53 are cancers of the lung.
- Transforming growth factorβ (TGFβ): Normally TGF-b is a significant inhibitor of cell proliferation, mainly by its action onG1 phase of the cell cycle. Its mutant form impairs the growth-inhibiting effect and thus permits cell proliferation. Examples of mutated forms of TGF-b are seen in cancers of the pancreas.
- Adenomatous polyposis coli (APC) gene: The APC gene is normally inhibitory to mitosis, which is done by a cytoplasmic protein, b-catenin. b-catenin normally blocks the signal to the nucleus or activates mitosis. In colon cancer, the APC gene is lost and thus the cancer cells continue to undergo mitosis without the inhibitory influence of 5-catenin.
“Early warning signs of knowledge gaps in patient understanding”
Microscopic Features of Malignancy
Gross Features of Malignancy:
- Boundaries are poorly circumscribed and irregular.
- Surrounding tissue is usually invaded.
- The size of the tumor is larger.
- Secondary changes such as bacterial invasion, pus formation, hemorrhage, infarction, and ulceration occur more often.
- Sarcomas have fish-flesh-like consistency while carcinomas are generally firm.
Microscopic Features of Malignancy
- It has a poor resemblance to the tissue of origin.
- Basal polarity is often lost.
- Pleomorphism is often present.
- The nuclear-cytoplasmic ratio is increased.
- Anisonucleosis is generally present.
- Hyperchromatism is often present.
- Mitotic figures are increased and are generally atypical and abnormal.
- Tumor giant cells are present with nuclear atypia.
Predisposing Factors Involved in the Development of Neoplasia
The following are the predisposing factors involved in the development of neoplasia:
- Familial and genetic factors
- Racial and geographic factors
- Environmental and cultural factors
- Age
- Sex.
Neoplasia Familial and Genetic Factors:
The risk of developing cancer in first-degree relatives of known cancer patients is three times as high as in control patients. Cancers with familial occurrence are colon, breast, ovary, brain and melanoma. Some of the common examples are:
- Retinoblastoma: It is an autosomal dominant inheritance. Carriers have a high risk of developing retinoblastoma. It is due to the missing portion of chromosome 13 where the RB gene is normally located. In the absence of the RB gene retinoblastoma develops.
- Familial polyposis coli: It is autosomal dominant. Polypoid adenomas are seen during birth or at an early age.
- Neurofiromatosis: There is presence of multiple neurofi bromas and café au lait spots. Patients have an autosomal dominant inheritance.
Neoplasia Racial and Geographic Factors
It is due to the differences in the environment and geographical areas due to which there is a change in climate, soil, water, diet, habits, customs, etc.
Various examples of racial and geographical variations in cancer are:
- White Europeans and Americans develop malignancy in the lungs, breasts,s, and colon. Breast cancer is common in Japanese women and more common in American women.
- Black Africans have cancers of the skin, penis, cervix, and liver.
- Indians of both sexes have a high incidence of oral cancer and upper aerodigestive tract cancer. In females carcinoma of the uterine cervix and the breast is common.
Neoplasia Environmental and Cultural Factors
We are surrounded by carcinogens that we breathe, inhale, drink, and touch. Examples are:
- Cigarette smoking causes oral cancer, cervical cancer, and cancer of the lungs, pharynx, pancreas, and urinary bladder.
- Alcohol abuse leads to cancer of the oropharynx, larynx, liver, and esophagus.
- Penile cancer is rare in Muslims and Jews as they are circumcised.
- Betel nut cancer of the cheek and tongue is common in some parts of India due to the habitual practice of keeping paan bolus at a particular place in the mouth over a long time.
Neoplasia Age
It is the most significant risk factor for cancer. Cancer occurs after 50 years of age. Some tumors have two peaks of incidence i.e. acute leukemia occurs in children and in old age. Besides acute leukemia, other tumors of infancy and childhood are neuroblastoma, retinoblastoma, rhabdomyosarcoma, etc.
Neoplasia Sex
Certain tumors are common in men as compared to women. Breast cancer is common in females throughout the world while lung cancer is common in males.
“How do educational materials clarify complex neoplasm concepts?”
Viral Oncogenes
Viral oncogenes are present in both types of viruses, i.e.
DNA oncogenic virus and RNA oncogenic virus.
Both viruses consist of three genes according to the coding pattern of each gene.
- Gag gene: It codes for group antigen
- Pol gene: It codes for the polymerase enzyme
- ENV gene: It codes for envelope protein.
- Molecular dissection of genomes of retroviruses revealed the presence of unique transforming sequences, i.e. viral oncogenes (v-oncs) not found in the genomes of non-transforming retroviruses.
- Viral oncogene sequences were almost identical to sequences found in the normal cellular DNA.
- Each viral oncogene is designated by a three-letter word that relates the oncogene to the virus from which it was isolated.
- Thus, the v-onc contained in the feline sarcoma virus is referred to as v-fes, whereas the oncogene in the simian sarcoma virus is called v-sis.
- Viral oncogenes are not present in several cancer-causing RNA viruses. One such example is a group, of so-called slow-transforming viruses that cause leukemias in rodents after a long latent period.
- Ras proteins were discovered initially in the form of viral oncogenes. Approximately 10 to 20% of all human tumors contain mutated versions of ras proteins.
- An acute transforming virus consists of retroviruses which transform all cells infected by them into malignant cells rapidly. All viruses of this group possess one or more viral oncogenes (v-once). All members of this group are defective viruses in which v-onc has substituted other essential genetic material i.e. gag, pol, and env. These defective viruses cannot replicate by themselves till the host cell is infected by another helper virus.
Leave a Reply