Ludwig’s Angina: Causes, Symptoms, and Treatment
Describe briefly Ludwig’s Angina.
Or
Write a short note on Ludwig’s Angina.
Or
Define, and describe clinical features and principles of treatment of Ludwig’s Angina
Or
Write a short answer on Ludwig’s Angina.
Answer.
Ludwig’s Angina Definition
It is a rapidly progressive polymicrobial cellulitis of the sublingual and submandibular spaces involving the floor of the mouth and suprahyoid area on both sides of the neck.
The most common cause is dental infection of second or third molar teeth
Read And Learn More: General Surgery Question And Answers
“Understanding Ludwig’s angina through FAQs: Causes, symptoms, and treatments explained”
Ludwig’s Angina Precipitating Factors
- Tooth extraction
- Submandibular sialadenitis
- Trauma
- Peritonsillar abscess
- Upper respiratory infection
- Interventions like endotracheal intubation.
Ludwig’s AnginaPredisposing Factors
- Diabetes mellitus
- Chemotherapy
- Oral cancer
- Alcohol
- Neutropenia.
“Importance of studying Ludwig’s angina for medical professionals: Questions explained”
“Common challenges in diagnosing and treating Ludwig’s angina effectively: FAQs provided”
Ludwig’s Angina Microscopic organisms
- As Ludwig’s angina is of dental origin streptococci or mixed oral flora are the most commonly reported microorganisms.
- The presence of staphylococci, E. coli, Pseudomonas, and anaerobes including Bacteroides and Peptostreptococcus, Prevotella species have also been isolated.
- The role of anaerobes as primary or synergistic organisms should not be omitted in the culture.
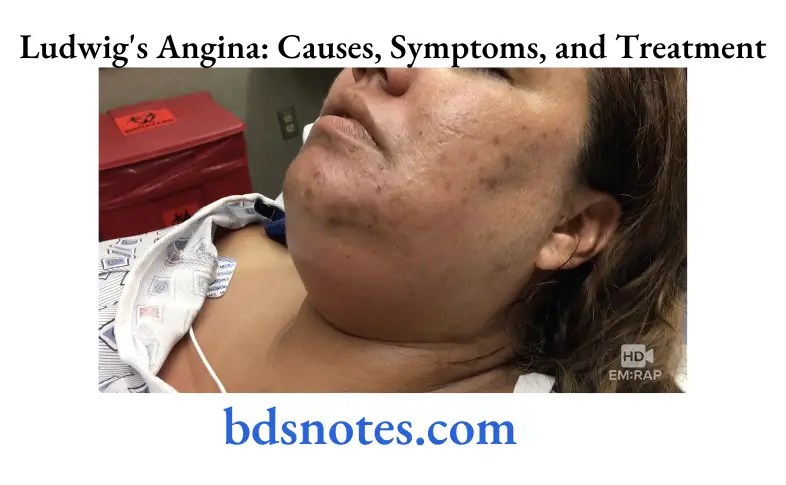
Ludwig’s Angina Clinical Features
- Presence of diffuse painful swelling with woody brawny induration of the mouth and anterior neck.
Swelling is non-fluctuant but with redness and tenderness. Bilateral submandibular edema with marked tenderness on palpation at the suprahyoid area with bull’s neck appearance. - Toxic features such as fever, tachycardia, and tachypnea is common.
- Difficulty in speech, earache, drooling of saliva, and putrid halitosis.
- Involvement of connective tissues, muscles, and fascial spaces but not glandular structures.
- The infection spread via fascial planes in continuity not by lymphatics; no lymph node enlargement.
- Edema of the tongue with pushing against the palate (elevation) upwards and backward causing airway obstruction, dysphagia, and odynophagia.
- Stridor, respiratory distress, and cyanosis may develop due to edema of the tongue and larynx.
“Factors influencing success with Ludwig’s angina knowledge: Q&A”
Ludwig’s Angina Investigations
- CT scan or MRI is useful to identify airway block, fluid collection, and the presence of gas.
- Ultrasound neck is a simpler method to identify the same.
Total count, blood sugar, chest X-ray, and often blood gas analysis (in severe cases) are done.
Ludwig’s Angina Differential Diagnosis
- Angioneurotic edema
- Sublingual hematoma
- Sialadenitis
- Lymphadenitis.
“Steps to explain Ludwig’s angina: Causes vs symptoms vs treatment: Q&A guide”
Ludwig’s Angina Complications
- Laryngeal edema can occur due to the spread of inflammation to the glottis submucosa via a stylohyoid tunnel. It may require an emergency tracheostomy to maintain respiration.
- Mediastinitis due to the spread of infection into mediastinum; aspiration pneumonia.
- Septicemia.
- Spread of infection into the parapharyngeal space leads to thrombosis of the internal jugular vein which may extend above into the sigmoid sinus which may be fatal.
Ludwig’s Angina Treatment
The main principles of treatment of Ludwig’s angina are:
- Airway maintenance
- Parenteral antibiotics
- Surgical decompression of tissues
- Hydration of patient
- Removal of cause
Ludwig’s Angina Airway Maintenance
- Edema of the glottis is what leads to airway obstruction and death of the patient, if untreated. Maintaining a patent airway is thus of prime importance.
- Intubation is done by an experienced anesthetist.
- Bulging of the posterior pharyngeal wall makes intubation difficult. Perforation may lead to aspiration of pus if an endotracheal tube is forced in blindly.
- A tracheotomy or cricothyroidotomy may be advisable.
Tracheostomy is usually difficult because the anatomical landmarks on the neck are not easily identifiable with the swelling.
“Role of dental infections in causing Ludwig’s angina: Questions answered”
Ludwig’s Angina Parenteral antibiotics
- Penicillin is the antibiotic of choice.
- Others such as amoxicillin and cloxacillin may also be used.
Metronidazole is given against anaerobic organisms. - Gentamycin can also be given along with penicillin for coverage of Pseudomonas.
Ludwig’s Angina Surgical Decompression
- It is usually preferred under LA instead of GA. The main aim is to relieve the pressure within the tissues for the edema to reduce.
Also, the pressure within the tissues compresses the blood vessels preventing the penetration of antibiotics in the area of interest.
Thus decompression improves vascularity and potentiates the action of antibiotics. - If there is pus, it provides a channel for the drainage of pus.
- Pus obtained from a drainage may be sent for culture and sensitivity testing.
- A decrease in edema reduces respiratory embarrassment.
- Ethyl chloride spray may be used or LA may be injected locally in the area of incision.
“Asymptomatic vs symptomatic effects of ignoring Ludwig’s angina principles: Q&A”
- Bilateral submandibular incisions with a midline submental incision may be placed.
- Blunt dissection through the skin, superficial fascia, platysma, deep fascia, and mylohyoid muscle is done to reach the sublingual space.
The sublingual space may alternatively be drained intraorally by an incision in the floor of the mouth of the mouth opening is adequate. - A drain is inserted through all these layers and stabilized.
- There may be no pus at all in most cases of Ludwig’s angina. Pus may only be seen at later stages.
- A loose dressing is placed which is changed every day after careful cleaning of the drain.
“Differential applications of Ludwig’s angina vs other neck infections: Questions answered”
Ludwig’s Angina Hydration of the Patient
- Pyrexia and dysphagia may lead to dehydration of the patient.
- It is necessary to put the patient on IV fluids.
Ludwig’s Angina Removal Of Cause
- Once the patient is stabilized and the trismus relieved to an extent, the offending tooth may be removed.
Leave a Reply