Intraoral Radiographic Techniques
Question 1. Write short note on long-cone technique in Intraoral Radiographic
Answer. Long-cone technique is also known as Paralleling or right angle technique.
Intraoral Radiographic Long-Cone Technique
- The X-ray film is supported parallel to the long axis of the teeth and the central ray of the X-ray beam is directed at right angles to the teeth and film.
- To achieve parallelism between the film and the tooth, the film must be placed away from the tooth, towards the middle of the oral cavity.
“Understanding the role of intraoral radiography in dental diagnostics: Q&A explained”
Dental Radiography MCQs With Answers
- Because the film is placed away from the tooth, image magnification and loss of definition results. To compensate for image magnification, the target film distance must also be increased to ensure that only the most parallel ray will be directed at the tooth and the film. So this technique is also called as long cone technique.
- In this technique a long cone of 12 inches is used and kVp used is 85 to 90 kVp.
- Here X-rays are directed perpendicular to the film so there is less geometric distortion, less magnification and more definition.
Ideal Intraoral Radiograph Criteria
Read And Learn More: Oral Radiology Question And Answers
“Importance of studying intraoral radiographic techniques for better outcomes: Questions explained”
Intraoral Radiographic Long-Cone Advantages
- Accuracy:
- Image is dimensionally accurate.
- Radiographic image is free of distortion and exhibit maximum detail and definition.
- There is no overlap of related structures.
- Simplicity: The technique is simple and easy to learn and use.
- Duplication: This technique is easy to standardize and can be accurately duplicated or repeated.
- Facial screen can be used.
- There is decreased secondary radiation.
- The relative position of the film, teeth and X-ray beam are always maintained so useful for handicapped and compromised patient.
- The periodontal bone level is well represented.
- The periapical tissues are accurately shown with minimum foreshortening or elongation.
“Common challenges in applying intraoral radiographic techniques effectively: FAQs provided”
Intraoral Radiographic Long-Cone Disadvantages
- Film placement with film-holding device is difficult in child patient.
- Patient discomfort: The holding device may impinge oral soft tissues and causes discomfort and gagging.
- Object film distance is increased so more chances of image magnification.
- The long cone is more spacious.
- Positioning of film is difficult in third molar region.
“Factors influencing success with intraoral radiographic techniques: Q&A”
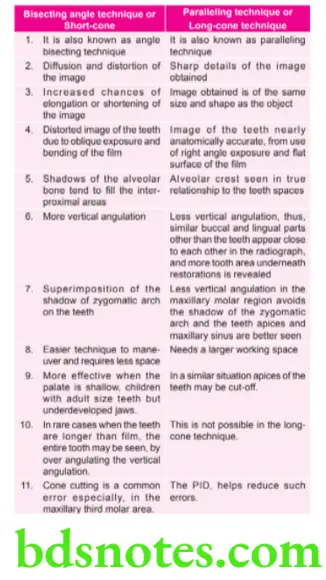
Question 2. Write Short Note On Difference Between Long-Cone And Short-Cone Technique.
or
compare and contrast bisecting angle technique and paralleling technique
Answer. Comparison between short-cone and long-cone techniques.
For advantages and disadvantages refer to Ans 1 of same chapter.
“Steps to explain different types of intraoral radiographic techniques: Periapical vs bitewing: Q&A guide”
Question 3. What is intraoral radiography? discuss in detail about bisecting angle technique. Give two differences between paralleling and bisecting angle technique.
Answer. Intraoral radiography is of three types, i.e.
- Periapical: It shows complete tooth as well as surrounding bone.
- Bitewing: It shows crowns of all maxillary and mandibular teeth as well as adjacent alveolar crest.
- Occlusal: It display images of incisal edges of anterior teeth and occlusal surfaces of posterior teeth as well as cross section of dental arches.
For angle bisecting technique refer to Ans 6 of same chapter.
For two differences refer to Ans 3 of same chapter.
“Role of paralleling technique in intraoral radiography: Questions answered”
Question 4. Write short note on Focal Length.
Answer. Focal length of an X-ray system is a measure of how strongly the system converges or diverges X-rays.
- For an X-ray system in air, it is the distance over which initially collimated rays are brought to a focus.
- An X-ray system with a shorter focal length has greater optical power than one with a long focal length; i.e., it bends the X-rays more strongly, bringing them to a focus in a shorter distance.
“Early warning signs of issues addressed by intraoral radiographic techniques: Common questions”
Question 5. describe the production of X-ray. discuss in detail the principle and method of paralleling technique of intraoral periapical radiology.
Answer. For production of X-ray refer to Ans 2 of chapter PRODUCTION OF X-RAY.
Principle of Paralleling technique of intraoral Periapical Radiology
Central principle of paralleling technique is that the X-ray receptor is supported parallel to the long axis of teeth and central ray of the X-ray beam is directed at right angles to the teeth and receptor. This orientation of the receptor, teeth and central ray minimizes geometric distortion and presents the teeth and supporting bone in their true anatomic relationship.
Leave a Reply