Hemodynamic Changes Question And Answers
Write a short note on the mechanism of edema.
Or
Write in short on the pathophysiology of edema.
hemodynamic changes questions and answers
Answer:
The word edema means swelling.
“Understanding the role of hemodynamic changes in cardiovascular health”

“Importance of studying hemodynamic changes for better healthcare outcomes”
“Edema may be defined as abnormal and excessive accumulation of fluid in interstitial tissue spaces and serous cavities”.
Mechanism of Edema
“Common challenges in managing hemodynamic instability”
Read And Learn More: Pathology Question And Answers
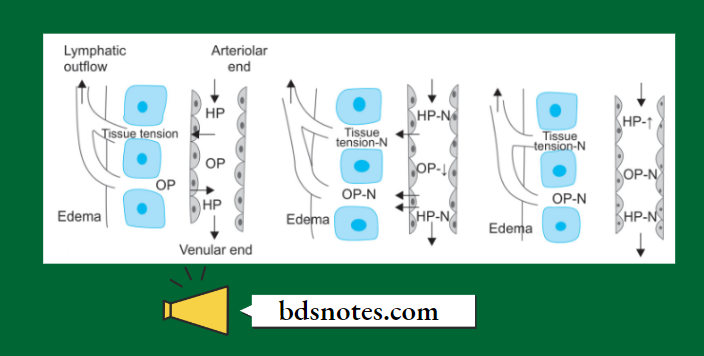
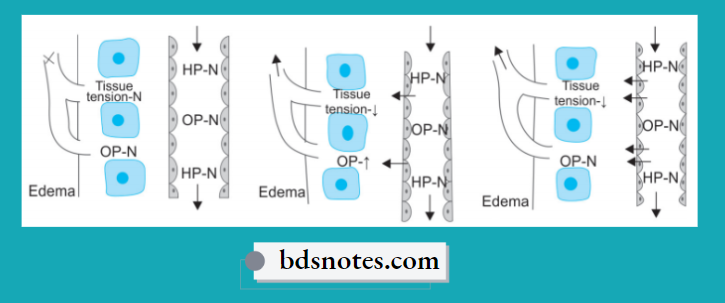
The following six mechanisms may be operating singly or in combination to produce edema:
1. Decreased plasma oncotic pressure: Plasma oncotic pressure is exerted by the total amount of plasma proteins that tend to draw fluid into the vessels normally. A fall in the total plasma protein level (hypoproteinemia of less than 5 g/dl, mainly hypoalbuminemia), results in a lowering of plasma oncotic pressure in a way that it can no longer counteract the the effect of the hydrostatic pressure of blood. This results in the increased outward movement of fluid from the capillary wall and decreased inward movement of fluid from the interstitial space causing edema. Hypoproteinemia usually produces generalized edema. Out of the various plasma proteins, albumin has four times higher plasma oncotic pressure than globulin; thus it is mainly hypoalbuminemia (albumin below 2.5 g/dl) that generally results in edema.
2. Increased capillary hydrostatic pressure: The hydrostatic pressure of the capillary is the force that normally tends to drive fluid through the capillary wall into the interstitial space by counteracting the force of plasma oncotic pressure. A rise in the hydrostatic pressure at the venular end of the capillary which is normally low to a level more than the plasma oncotic pressure results in minimal or no reabsorption of fluid at the venular end, consequently leading to edema.
3. Lymphatic obstruction: Normally, the interstitial fluid in the tissue spaces escapes by way of lymphatics. Obstruction to the outflow of these channels causes localized edema, known as lymphedema.
“Steps to identify common types of hemodynamic changes”
4. Tissue factors: The two forces acting in the interstitial space—oncotic pressure of the interstitial space and tissue tension, are normally quite small and insignificant to counteract the effects of plasma oncotic pressure and capillary hydrostatic pressure respectively. However, in some situations, the tissue factors in combination with other mechanisms play a role in the causation of edema.
5. Increased capillary permeability: An intact capillary endothelium is a semipermeable membrane that permits the free flow of water and crystalloids but allows minimal passage of plasma proteins normally. However, when the capillary endothelium is injured by various ‘capillary poisons’ such as toxins and their products (For Example. histamine, anoxia, venoms, certain drugs, and chemicals), the capillary permeability to plasma proteins is enhanced due to the development of gaps between the endothelial cells causing leakage of plasma proteins into the interstitial fluid. This, in turn, causes reduced plasma oncotic pressure and elevated oncotic pressure of the interstitial fluid, consequently producing edema.
“Role of hypotension in causing hemodynamic instability”
6. Sodium and water retention: The mechanism of edema by sodium and water retention in the extravascular compartment is best described in relation to derangement in the normal regulatory mechanism of sodium and water balance. Normally about 80% of tubules are under the influence of either intrinsic renal mechanism or extra-renal mechanism while retention of water is affected by the release of antidiuretic hormone. The possible factors responsible for causing edema by excessive retention of sodium and water in the extravascular compartment via stimulation of intrinsic renal and extrarenal mechanism as well as via release of ADH are:
“Early warning signs of knowledge gaps in patient understanding”
- Reduced glomerular filtration rate in response to hypovolemia.
- Enhanced tubular reabsorption of sodium and consequently decreased renal excretion.
- Increased filtration factor, i.e. increased filtration of plasma from the glomerulus.
- Decreased capillary hydrostatic pressure is associated with increased renal vascular resistance.
Leave a Reply