Environmental And Nutritional Diseases
Write a short note on scurvy.
Or
Discuss in short scurvy.
Or
Write in brief on vitamin C deficiency.
Answer:
Vitamin C deficiency in the food or as conditioned deficiency results in scurvy.
The lesions and clinical manifestations are seen more commonly in two ages, i.e. early childhood and very aged.
“Understanding the role of environmental and nutritional factors in disease development”
“Importance of studying environmental and nutritional diseases for better healthcare”
Read And Learn More: Pathology Question And Answers
The lesions are:
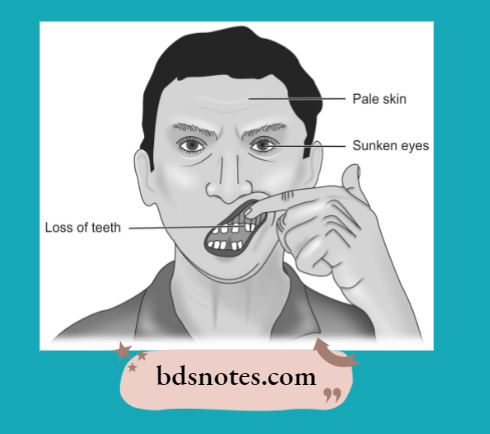
1. Lesions in teeth and gums: Scurvy may interfere with the development of dentin. The gums are soft, and swollen and may bleed readily and get infected commonly. The gums are called scorbutic gums.
“Common challenges in addressing environmental and nutritional diseases”
“Steps to identify common environmental diseases”
2. Hemorrhagic diathesis: A marked tendency to bleed is characteristic of scurvy. There may be hemorrhages of skin, mucus membranes, gums, muscles, joints, and under the periosteum.
3. Skeletal lesions: The most prominent change is the deranged formation of osteoid matrix and not deranged mineralization. Growing tubular bones and as well as flat bones are affected.
4. Delayed wound healing: There is a delay in healing wounds in scurvy due to:
- Deranged collagen synthesis
- Poor maturation and prevention of fibroblasts.
- Localization of infection in wounds.
environmental and nutritional diseases questions
“Role of air pollution in causing respiratory diseases”
5. Anemia: It is common in scurvy. It is most often Normocytic and Normochromic.
Scurvy Histopathology
The following are the histologic features of scurvy:
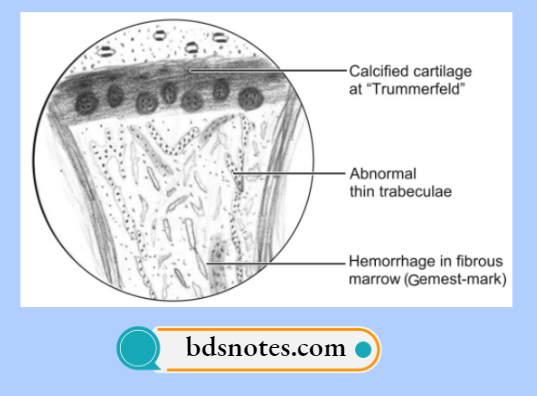
- In scurvy, osteoblasts fail to form osteoid on spicules of calcified cartilage matrix.
- Cartilage cells of the epiphyseal plate proliferate normally and salts are deposited in the matrix between columns of cartilage cells.
- A wide zone of calcified but non-ossified matrix known as scorbutic lattice develops in the metaphysics.
“Early warning signs of untreated environmental exposures”
- As the scorbutic lattice increases in width more fragile zone develops which leads to a complete fracture of spicules with separation and deformity of the cartilage shaft junction.
- Fractures of calcified matrix material lead to the classic picture of scurvy known as the Trummerfeld zone.
- The area beneath the Trummerfeld zone is free of hematopoietic cells and is formed of connective tissue cells known as Gemestmark.
environmental diseases question and answer
Leave a Reply