Diseases Of Skin Important Question And Answers
Question.1. Name the vesiculobullous lesions of oral cavity.
Describe etiology, histopathology, and clinical features of oral lichen planus.
Or
Write short answer on clinical features and histology of lichen planus
Answer.
“Understanding the role of skin diseases in overall health: Q&A explained”
Vesiculobullous Lesions
Fitzpatrick Classification
- According to Anatomical Plane:
- Intraepidermal Blister Granular Layer
- Pemphigus foliaceus
- Frictional blisters
- Staphylococcus scalded syndrome.
- Spinous Layer
- Eczematous dermatitis
- Secondary to heat and cold
- Herpes virus infection
- Familial benign pemphigus
- Intraepidermal Blister Granular Layer
“Importance of studying skin diseases for better diagnostic outcomes: Questions explained”
- Suprabasal
- Pemphigus vulgaris
- Pemphigus vegetans
- Darier’s disease
- Basal layer
- Erythema multiforme
- Toxic epidermal necrolysis
- Lupus erythematosus
- Lichen planus
- Epidermolysis bullosa simplex
- Suprabasal
“Common challenges in diagnosing skin diseases effectively: FAQs provided”
Read And Learn More: Oral Pathology Question And Answers
- DermalEpidermal Junction Zone:
- Lamina lucida
- Bullous pemphigoid
- Cicatrical pemphigoid
- Epidermolysis bullosa junctional
- Below basal lamina
- Erythema multiforme
- Epidermolysis bullosa dystrophica
- Lamina lucida
“Steps to explain causes of skin diseases: Allergies vs infections: Q&A guide”
Vesiculobullous lesions
- Primary Blistering:
- Pemphigus
- Bullous pemphigoid
- Cicatrical pemphigoid
- Epidermolysis bullosa acqusita.
- Secondary blistering:
- Contact
- Erythema multiform
- Toxic epidermal necrolysis.
- Infection:
- Varicella zoster
- Herpes simplex
- Bullous impetigo.
- Systemic disease:
- Infection cutaneous emboli
- Metabolic
- Diabetic with bullae
- Porphyria cutanea tarda.
“Role of autoimmune disorders in causing skin conditions like psoriasis: Questions answered”
Oral Lichen Planus
Lichen planus is also known as lichen ruber planus.
- It is a precancerous condition
- Lichen planus is a common mucocutaneous disease which arises due to an abnormal immunological reaction and the disease has some tendency to undergo malignant transformation.
Oral Lichen Planus Etiology
- Immunology:
- Due to cell-mediated immune response
- Due to autoimmunity
- Immunodeficiency.
- Genetic factors: Lichen planus is reported in families, twins, husband and wife.
- Infectious: By spirochete.
- Drugs and chemicals: It is responsible for the lichenoid reaction.
- Psychogenic factors: Stress results, nervousness with emotional upset, overwork and some form of mental strain.
- Habit: Chewing of tobacco, betel nut and smoking.
“Early warning signs of issues addressed by understanding skin disease pathogenesis: Common questions”
Clinical Features Of Oral Lichen Planus
- It occurs among middle-aged and elderly people.
- There is slight predilection for the females.
- Lichen planus can involve several areas of oral cavity.
Oral lesion: Mucosal surface of buccal mucosa, vestibule,tongue, lips, flor of mouth, palate and gingiva. - Patient may report with burning sensation of oral mucosa.
- Oral lesion is characterized by radiating white and gray velvety thread-like papules in linear, angular or retiform arrangement, tiny white elevated dots are present at the intersection of white lines known as “Wickhm’s striae”.
“Asymptomatic vs symptomatic effects of ignoring skin disease causes: Q&A”
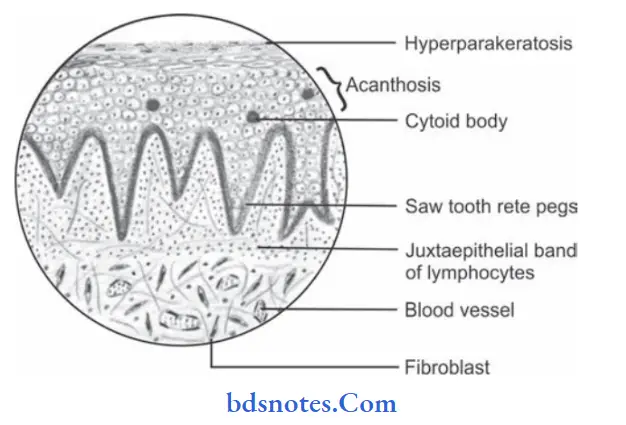
Histopathology Of Oral Lichen Planus
- Overlying surface epithelium exhibits hyperorthokeratinization or hyperparakeratinization or both.
- Acanthosis of spinal cell layer is present.
- Shortened and pointed rete pegs of epithelium which produces “Saw tooth” appearance.
- Intercellular edema in spinous cell layer is present.
- There is presence of necrosis or liquefaction degeneration of basal cell layer of epithelium.
- Few rounded or ovoid, amorphous eosinophilic bodies are present which are known as “Civatt bodies”.
- These civatt bodies represent dead keratinocytes or other necrotic epithelial components which are transported to connective tissue for phagocytosis.
- Chronic inflammatory cell infiltration is present in juxta epithelial lesion.
“Differential applications of congenital vs acquired skin diseases: Questions answered”
Leave a Reply