Diseases Of Blood And Blood Forming Organs Important Question And Answers
Question 1. Write short note on pernicious anemia.
Answer. Pernicious anemia is a type of a chronic progressive, megaloblastic anemia of adults and is caused by a deficiency of intrinsic factors in stomach.
Etiology
- Due to impaired absorption of vitamin B12: This occurs due to the atrophy of gastric mucosa which results in lack of secretion of intrinsic factor.
- As autoimmune reaction to gastric parietal cells or intrinsic factor.
- Strict vegetariAns suffr from vitamin B12 deficiency as it is present only in eggs, meat, and milk.
- Malabsorption of vitamin B12 due to inadequate gastric production or defective functioning of intrinsic factor.
- Various other causes which lead to the deficiency of vitamin B12 are gastrectomy, celiac disease, Crohn’s disease, alcoholism, prolong usage of drugs, i.e. proton pump inhibitors, colchicines.
Clinical Features
- Generalized weakness, palpitation, nausea, vomiting, anorexia, diarrhea and dyspnea.
- Patients have smooth, dry, and yellow skin.
- Neurological manifestation includes tingling sensation in hand and feet, paresthesia of extremities due to peripheral nerve degeneration.
- Glossitis, glossodynia (painful tongue) and glossopyrosis (itching and burning tongue).
- Tongue appears beefy red in color.
- Sometimes loss of papilla produces a bald appearance of tongue.
- Sometimes hyperpigmentation occurs in mucosa.
- Inflmmation and burning sensation surround entire oral mucosa.
blood diseases questions and answers
Read And Learn More: Oral Pathology Question And Answers
Histopathology
- Oral epithelial cells become enlarged and show hyperchromatic nuclei with prominent nucleoli along with serrated nuclear membrane.
- Epithelium becomes atrophic.
- There is presence of subepithelial chronic inflmmatory cell infitration.
Laboratory Findings
hematology important questions
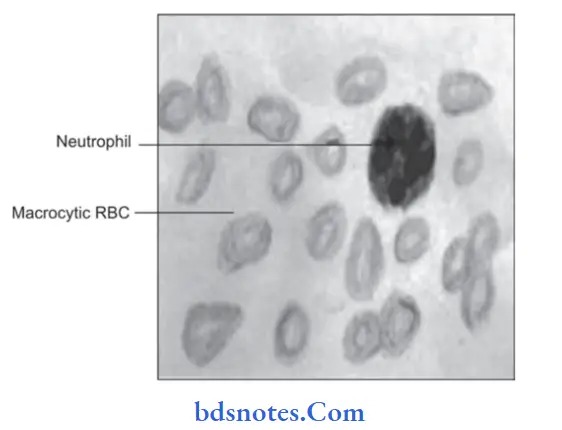
- Macrocytosis is commonly seen.
- Red blood cell count is decreased, at times it is 10 lakh/cubic mm of blood.
- Mild to moderate thrombocytopenia is also seen.
- MCV, MCH, MCHC concentration is normal
- Howell jolly bodies and cabot rings are present.
- Neutrophils are hypersegmented.
- Buccal scrapings show nuclear abnormalities
- Schilling test show vitamin B12 deficiency.
- Serum lactate dehydrogenase is markedly increased while serum potassium, cholesterol and skeletal alkaline phosphatase are often decreased.
- Bone marrow is hypercellular and show trilineage differentiation.
- Erythroid precursors are large and oval. Nucleus is large and contains coarse motley chromatin clumps giving checkboard appearance.
Treatment
IM injection of vitamin B12 is given.
Leave a Reply