Diabetes Mellitus Question And Answers
Discuss etiopathogenesis, clinical features, diagnosis, and complications of diabetes mellitus.
Or
Write a short note on complications of diabetes mellitus.
Or
Discuss etiopathogenesis and complications of type 2 diabetes mellitus. Enumerate its complications.
Or
Write in short on diabetes mellitus.
Or
Write a short note on diabetes mellitus.
Answer:
“Understanding the role of diabetes mellitus in overall health”
Diabetes mellitus is a heterogeneous metabolic disorder characterized by the common feature of chronic hyperglycemia with disturbance of carbohydrate, fat, and protein metabolism.
Diabetes mellitus questions and answers
Diabetes mellitus is classified into two types:
- Type 1 Diabetes Mellitus: It is also called insulin-dependent or juvenile-onset diabetes.
- Type 2 Diabetes Mellitus: It is also called non-insulin-dependent diabetes mellitus or maturity-onset diabetes mellitus.
“Importance of studying diabetes mellitus for better healthcare outcomes”
“Common challenges in diagnosing and managing diabetes mellitus”
Etiopathogenesis
Type 1: Diabetes Mellitus
The basic phenomenon is the destruction of a cell mass, usually leading to absolute insulin deficiency.
- Genetic Susceptibility:
- Identical twins: If one twin has type I diabetes mellitus, there is about a 50% chance of the second twin developing it.
- Susceptibility gene on HLA region in chromosome 6.
- Autoimmune Factors:
- Presence of Islet cell antibodies against insulin.
- Occurrence of lymphocytic infiltrate in and around pancreatic islets termed insulitis.
- CD8 +T cell-mediated selective destruction of b cells.
- Autoimmune diseases like Graves’ disease, Addison’s disease, and Hashimoto’s thyroiditis.
Diabetes mellitus viva questions
Read And Learn More: Pathology Questions and Answers
Environmental Factors:
- Certain viral infections, i.e., Mumps, measles, etc.
- Experimental induction with chemicals.
- Geographic and seasonal variations.
“Steps to identify common types of diabetes mellitus”
Type 2: Diabetes Mellitus
- Genetic Factors:
- Identical Twins: 80% chance of developing diabetes if one twin has diabetes mellitus.
- If both parents are diabetic, the risk in offspring rises to 50%.
- Constitutional Factors:
- Obesity
- Hypertension
- Low physical activity.
- Insulin resistance
- Impaired glucose utilization
- Receptor and post-receptor defects
- Decreased insulin secretion
- Due to amylin
- Due to the glucose toxicity of islets.
- Due to lipotoxicity.
“Role of type 1 diabetes in autoimmune conditions”
These above factors lead to increased hepatic glucose synthesis and cause hyperglycemia, mia which leads to Type 2 diabetes mellitus.
Clinical Features of Diabetes Mellitus
Type 1: Diabetes Mellitus
- It occurs at an early age, generally below the age of 35 years.
- The onset of symptoms is often abrupt.
- Patient has polyuria, polydypsia and polyphagia.
- Patients are not obese and have generally progressive loss of weight.
- Patients are prone to develop metabolic complications such as ketoacidosis.
“Early warning signs of untreated diabetes mellitus”
Type 2: Diabetes Mellitus
- It occurs in middle age or beyond, usually above the age of 40.
- The onset of symptoms is slow.
- Patients are asymptomatic.
- Patients are obese and have unexplained weakness and loss of weight.
- Metabolic complications such as ketoacidosis are present.
Complications of Diabetes
Both types of diabetes mellitus may develop complications which are divided into two major groups:
- Acute metabolic conditions
- Late systemic complication.
Acute Metabolic Complications
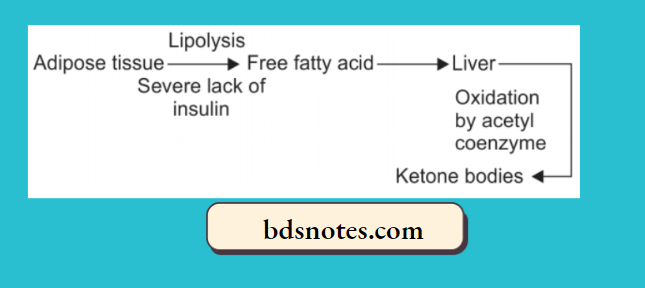
- Diabetic ketoacidosis: Ketoacidosis is almost exclusively a complication of type I diabetes mellitus. It can be developed in severe insulin deficiency.
“Asymptomatic vs symptomatic stages of diabetes mellitus progression”
“Steps to educate patients about diabetes mellitus and its risks”
Clinically, the condition is characterized by anorexia, nausea, vomiting, deep and fast breathing, confusion, and coma.
- Hyperosmolar non-kinetic comma: It is usually a complication of type 2 diabetes mellitus. It is caused by severe dehydration resulting from sustained hyperglycemic diuresis.
- Blood sugar is extremely high, and plasma osmolarity is high.
- Thrombolytic and bleeding complications are frequent due to the high viscosity of blood.
- Hypoglycemic episode: It may develop in patients with type 1 diabetes mellitus.
- It may result in excessive administration of insulin, missing a meal, or due to stress.
- It is harmful as it produces permanent brain damage and also results in worsening diabetic control and rebound hyperglycemia.
“Role of counseling in improving awareness of blood sugar control”
Diabetes mellitus exam questions
Late Systemic Complications
1. Atherosclerosis: Both Type 1 and Type 2 diabetes mellitus cause atherosclerosis. The process of atherosclerosis accelerated in patients with diabetes.
Various contributory factors for atherosclerosis are hyperlipidemia, reduced HDL levels, nonenzymatic glycosylation, increased platelet adhesiveness, obesity, and hypertension in diabetes.
Atherosclerosis can lead to coronary artery disease, silent myocardial infarction, cerebral stroke, and gangrene of the toe and feet.
2. Diabetic microangiopathy: This is characterized by the thickening of the basement membrane of small blood vessels and capillaries of different organs and tissues, i.e., skin, skeletal muscle, eye, and kidney.
A similar type of basement membrane-like material is deposited in non-vascular tissues, i.e.,. Peripheral nerves, renal tubules, and Bowman’s capsule.
Diabetic microangiopathy occurs due to recurrent hyperglycemia, which leads to increased glycosylation of hemoglobin and other proteins, which causes thickening of the basement membrane.
3. Diabetic nephropathy: Involvement of the renal system is an important complication of diabetes mellitus.
Renal complications develop early and frequently in Type 1 diabetes mellitus as compared to type 2 diabetes mellitus.
Various clinical syndromes are associated with diabetic nephropathy, i.,e. asymptomatic proteinuria, nephrotic syndrome, renal failure, and hypertension.
Cardiovascular diseases are 40 times more common in patients with end-stage renal disease in diabetes mellitus as compared to non-diabetics.
“Early warning signs of knowledge gaps in patient understanding”
4. Diabetic neuropathy: It affects all the parts of the nervous system. Peripheral neuropathy is more characteristic. Pathologic changes are segmental demyelination, Schwann cell injury, and axonal damage.
5. Diabetic retinopathy: It is an important cause of blindness. This complication develops in more than 60% of diabetic patients.
Other ocular complications of diabetes mellitus are glaucoma, cataract, and corneal disease. Risk is greater in Type 1 diabetes mellitus as compared to type 2 diabetes mellitus.
6. Infections: Diabetes leads to the susceptibility of infection,ons,i.e., tuberculosis, pneumonia, pyelonephritis, otitis, carbuncles, and diabetic ulcers. It occurs due to impaired leucocyte functions, reduced cellular immunity, poor blood supply, and hyperglycemia.
Diagnosis of Diabetes Mellitus
“Asymptomatic vs symptomatic effects of poor communication”
- Urine testing: Urine tests are cheap and convenient. They are tested for the presence of glucose and ketones.
- Glucosuria:
- Benedict’s qualitative test detects any reducing test in urine.
- Dipstick Test: A more sensitive and glucose-specific test, a med is based on an enzyme-coated paper strip that turns purple when dipped in urine containing glucose.
- Ketonuria: The test for ketone bodies in urine is required for assessing the severity of diabetes.
- Dipstick Test: A more sensitive and glucose-specific test, a med is based on an enzyme-coated paper strip that turns purple when dipped in urine containing glucose.
- Benedict’s qualitative test detects any reducing test in urine.
- Glucosuria:
- Single blood sugar estimation: For diagnosis of diabetes, blood sugar determination is necessary.
- A fasting plasma glucose value above 126 mg/dl is certainly indicative of diabetes.
- Oral glucose tolerance test:
- An individual with a fastening value of random glucose higher than 126 mg/dl and a 2-hour value after 75 gm oral glucose higher than 200 mg/dl is labeled as diabetic.
- In a symptomatic case, the random blood glucose value above 200 mg/dl is diagnosed as diabetes.
Leave a Reply