Developmental Disorders Of Teeth And Jaw Question And Answers
Question 1. Write short note on anodontia.
Answer. Anodontia is defined as the condition in which there is congenital absence of teeth in oral cavity.
“Importance of studying developmental disorders for better diagnostic outcomes: Questions explained”
“Understanding developmental disorders of teeth and jaw through FAQs: Q&A explained”
Anodontia Etiology
The causes of anodontia are:
- Hereditary factor.
- Environmental factor.
- Familial factor.
- Syndrome associated.
- Radiation injury to the developing tooth germ.
Developmental Disorders of Teeth and Jaw: Symptoms, Diagnosis, and Treatment
“Common challenges in diagnosing developmental disorders effectively: FAQs provided”
Types of Anodontia
- Complete anodontia: There is congenital absence of all the teeth.
- Partial anodontia: Congenital absence of one or few teeth.
Anodontia can also be divided into following types:
- True anodontia: It occurs due to failure of development or formation of tooth in jaw bone.
- Pseudo anodontia: It refers to the condition in which teeth are present within the jaw bone but are not clinically visible in the mouth, as they have not erupted, e.g. impacted teeth.
- False anodontia: It is the condition in which teeth are missing in the oral cavity because of their previous extraction.
“Early warning signs of issues addressed by understanding developmental disorder pathogenesis: Common questions”
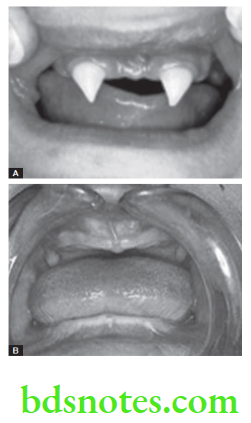
Complete Anodontia
- It is the condition in which there is neither any deciduous tooth nor any permanent tooth present in the oral cavity.
- It is usually seen in association with hereditary ectodermal dysplasia. A complete anodontia is a common feature of hereditary ectodermal dysplasia, however, in many cases cuspids are present in this disease.
- Complete anodontia occurs among children those who have received high doses of radiation to the jaws as infants for therapeutic reasons.
“Steps to explain causes of developmental disorders: Genetic vs environmental factors: Q&A guide”
Partial Anodontia
- It is a common phenomenon and is characterized by congenital absence of one or few teeth.
- In partial anodontia any tooth can be congenitally missing.
- Third molars are most frequently observed as congenitally missing teeth.
- Mandibular first molar and the mandibular lateral incisor are least likely to be missing.
“Role of gene mutations in causing developmental disorders of teeth and jaw: Questions answered”
Read And Learn More: Oral Medicine Question And Answers
Question 5. Write short note on differential diagnosis of supernumerary teeth.
Answer. Following is the differential diagnosis of supernumerary teeth:
- Cleidocranial dysplasia: When viewed radiographically, numerous supernumerary teeth present. Patients routinely have 10 or more supernumerary teeth that are producing crowding and preventing eruption of deciduous teeth. There is an obvious mixed dentition with this disorder.
- Gardner syndrome: The second differential diagnosis that is associated with numerous supernumerary teeth is Gardner syndrome (familial adenomatous polyposis). This syndrome involves multiple supernumerary teeth as well as osteomas. The presence of supernumerary teeth may not be as numerous as those found in cleidocranial dysplasia.
- Supernumerary teeth in non syndromic cases: These cases present without any known associated diseases or syndromes. The patients are thought to have a genetic propensity toward supernumerary teeth.
Leave a Reply