Tissue Changes During Orthodontic Tooth Movements
The histological or tissue changes incidental to orthodontic treatment are explained under the following headings:
- Tissue changes at the pressure zone.
- Tissue changes at the tension zone.
- Tissue changes in other areas, i.e. pulp, dentin, cementum, gingiva, and TMJ.
“Understanding the role of tissue changes in orthodontic treatment: Q&A explained”

“Importance of studying tissue changes for better orthodontic results: Questions explained”
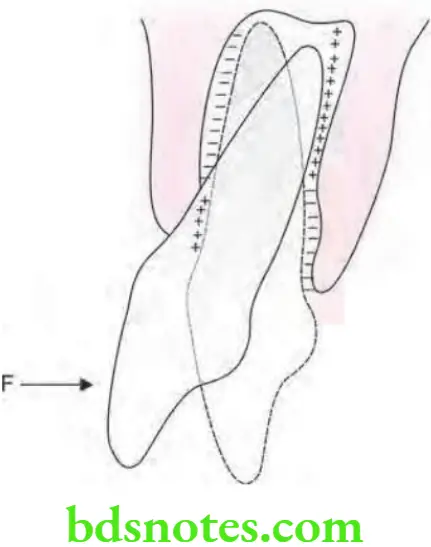
Tissue Changes at Pressure Zone
- If light forces are applied frontal resorption will occur.
- If heavy forces are applied hyalinization and undermining resorption will occur.
“Common challenges in monitoring tissue changes during orthodontic treatment: FAQs provided”
Frontal Resorption
- As orthodontic tooth movement starts osteoclasts get activated.
- Osteoclasts are derived from local population or blood supply.
- Activated osteoclasts start resorption by resorbing adjacent lamina dura. This process of bone resorption is also known as frontal resorption.
- Resorption starts from the PDL side of the alveolar bone.
- Frontal resorption takes place after two days of orthodontic force application.
Frontal Resorption In Orthodontics
Hyalinization
- If the orthodontic force increases more than the capillary pulse pressure, i.e. 20–26 gm/cm2 blood vessels get compressed or occluded.
- As PDL gets compressed the blood supply of the compressed area gets cut off
- Now the cells that become activated osteoclasts remain inactive.
- The sterile necrotic area is visible in compressed PDL.
- This is when seen in a light microscope appears as an area devoid of cells and this is known as a hyalinized area and the process is known as hyalinization.
- Hyalinization is a reversible process.
- The effect of hyalinization is that it does not allow the tooth to move.
- In hyalinization, the tooth can be moved in the condition in which bone beneath the hyalinized area undergoes resorption.
- Hyalinization lasts for one to two weeks after which resorption occurs by undermining resorption.
“Steps to explain different types of tissue changes during orthodontic tooth movements: Bone vs soft tissue: Q&A guide”
Undermining Resorption
- Resorption is also known as indirect resorption.
- As there is the occurrence of hyalinization, chances of frontal resorption are diminished.
- After some days hyalinized zone is invaded by the cells from adjacent normal areas of PDL.
- With this osteoclasts also appear in adjacent marrow spaces.
- These osteoclasts resorb bone adjacent to the hyalinized PDL zone from the underside. This is known as undermining resorption as bone resorption occurs from the underside of lamina dura.
- Resorption of bone occurs from the endosteal part.
- Hyalinization and undermining resorption lead to delayed tooth movement while tooth movement is efficient with frontal resorption.
- Bone deposition occurs at the rate of 15µm/day
“Role of bone remodeling in orthodontic tooth movements: Questions answered”
Tissue Changes at Tension Zone
- In areas of tension cellular activity becomes delayed as compared to the pressure zone.
- In the tension zone, 30 hours are required for increased cellular activity.
- Macrophages are abundant in the tension zone.
- Inflammation and remodeling of fibrous elements over evident in the tension zone.
- A new unmineralized matrix is laid down in the fibers which are close to the alveolar wall.
- Later on osteoid which is synthesized by osteoblasts is laid down on the complete alveolar wall over the tension zone.
- Bone deposition occurs at the rate of 30µm/day.
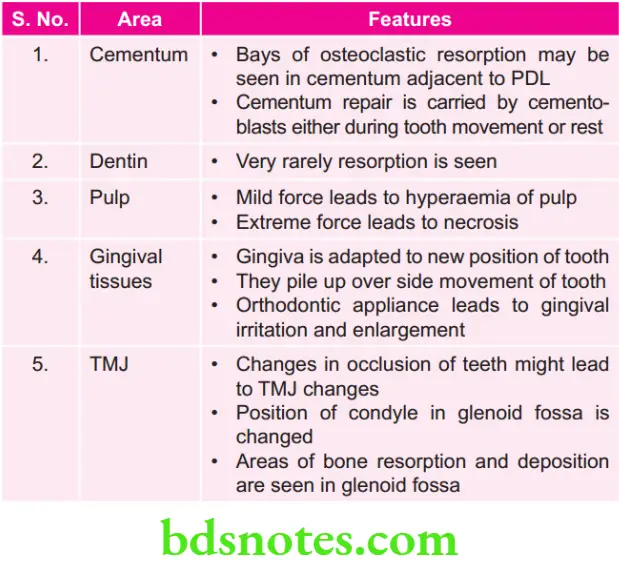
Tissue Changes in Other Areas
Leave a Reply