Benign And Malignant Tumors Of Oral Cavity Important Question And Answers
Question 1. Enumerate white lesions of orofacial region. Describe etiology, histopathology and clinical features of leukoplakia.
Or
Enumerate white lesions of oral cavity. Describe leukoplakia in detail.
Answer. The white lesions of oral cavity/orofacial region are as follows:
- Hereditary condition:
- Leukoedema
- White sponge nevus
- Hereditary benign intraepithelial dyskeratosis
- Keratosis follicularis
- Ptylosis syndrome.
- Leukoplakia and malignancies:
- Chronic cheek biting
- Friction or trauma-associated leukoplakia
- Tobacco associated leukoplakia
- Carcinoma in situ
- Squamous cell carcinoma
- Verrucous carcinoma.
“Understanding the role of tumors in oral health: Benign vs malignant Q&A explained”
Read And Learn More: Oral Pathology Question And Answers
- Dermatosis:
- Lichen planus
- Lupus erythematous.
- Inflammation:
- Mucous patches of syphilis
- Candidiasis
- Koplik spots of measles.
- Miscellaneous conditions:
- Oral submucous firosis
- Papilloma
- Lipoma
- Hairy tongue
- Geographic tongue
- Fordyce’s granules.
“Importance of studying benign and malignant tumors for better diagnostic outcomes: Questions explained”
Leukoplakia is defied as “a white patch or plaque that cannot be characterized, clinically or pathologically as any other disease and is not associated with any other physical or chemical causative agent except the use of tobacco”.
Axell et al, 1984 Leukoplakia is defied as a predominantly white lesion of the oral mucosa that cannot be characterized as any other defiable lesion. WHO (1997)
Leukoplakia should be used to recognize white plaques of questionable risk having excluded (other ) known diseases or disorders that carry no increased risk for cancer.
“Common challenges in diagnosing benign and malignant tumors effectively: FAQs provided”
Warnakulasuriya et al (2008).
Etiology Of Leukoplakia
The common predisposing factors of leukoplakia are:
- Tobacco: It is used by large number of people in various forms such as smoking of cigarett, cigar, biddies and pipes.
All these types of tobacco habits are important for development of leukoplakia.
It is believed that during smoking a large amount of tobacco end products are produced in oral cavity.
The products in association with heat cause severe irritation to oral mucus membrane and finally result in development of leukoplakia. - Alcohol: Alcohol leads to the entry of carcinogen into exposed cells and thus alters oral epithelium as well as its metabolism.
- Candidiasis: Chronic candidal infections are associated with leukoplakia.
- Dietary deficiency: Deficiency of vitamin A causes metaplasia and hyperkeratinization of epithelium which may result in development of leukoplakia.
- Syphilis: Syphilitic infections play minor role in causation of leukoplakia.
- Hormonal imbalance: Imbalance or dysfunction of both male and female sex hormones causes keratogenic changes in oral epithelium. These changes lead to the development of leukoplakia.
“Factors influencing success with treatment of oral cavity tumors: Q&A”
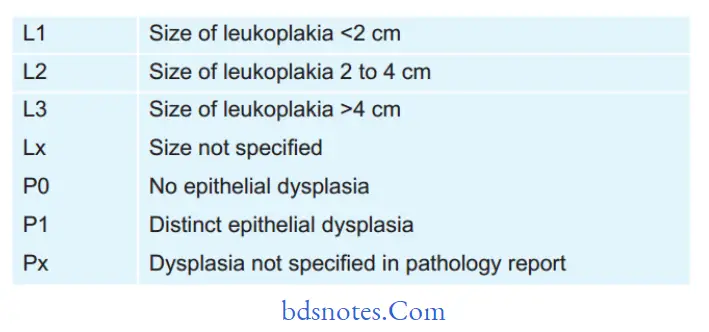
Modifid Classifiation of Leukoplakia
“Steps to explain the causes of benign and malignant tumors in the oral cavity: Genetics vs environmental factors: Q&A guide”
Oral Leukoplakia Staging System
Stage 1 L1P0
Stage 2 L2P0
Stage 3 L3P0 Or L1L2P1
Stage 4 L3P1
Histopathology
During leukoplakia variety of histologic changes are present which are related to:
- Keratinization pattern
- Changes in cellular layer
- Thickness of epithelium
- Alteration in underlying connective tissue stroma.
“Early warning signs of knowledge gaps in patient understanding of oral cavity tumors: Common questions”
Keratinization pattern
- Leukoplakia generally presents hyperorthokeratinization or hyperparakeratinization or both with or without the presence of epithelial dysplasia.
- In case of leukoplakia an abnormal increase in the thickness of orthokeratin layer is seen in area of epithelium which is usually keratinized.
- An important histological criterion of leukoplakia is presence of hyperkeratinization of normally keratinized epithelium or some amount of parakeratin deposition in area of epithelium which are usually not keratinized.
- Epithelium dysplasia is more frequently associated with hyperkeratinized lesion.
“Role of carcinogens like tobacco and alcohol in causing malignant oral tumors: Questions answered”
Changes in Cellular layer
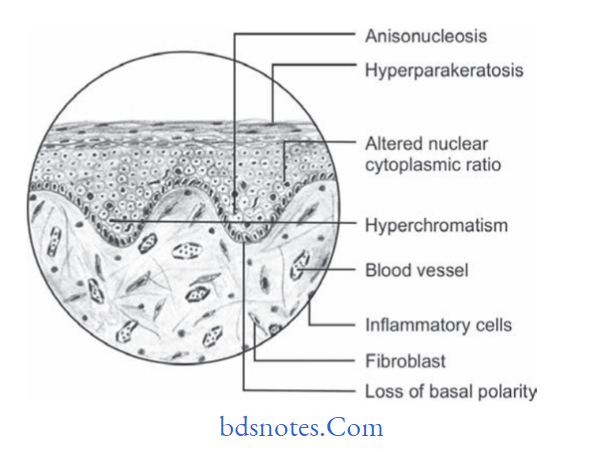
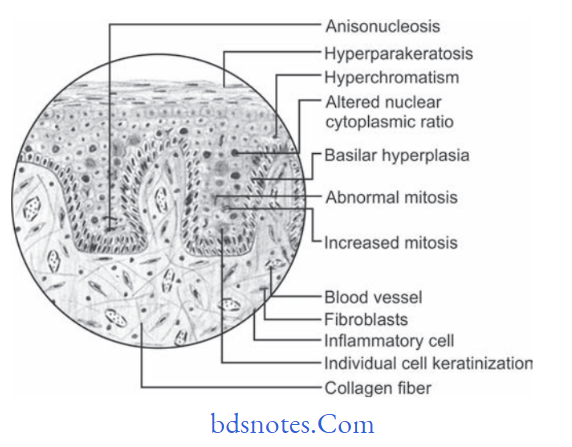
Epithelial dysplasia is the hallmark of histologic changes seen in epithelium in case of leukoplakia. The criteria for epithelial dysplasia are:
Architecture and Cytologic Criteria for Grading Epithelial Dysplasia Given by WHO (2005)
Architecture Criteria
- Irregular epithelial stratifiation
- Loss of polarity of basal cells
- Basal cell hyperplasia
- Drop shaped rete pegs
- Increased number of mitotic fiures
- Abnormally superfiial mitosis
- Dyskeratosis i.e. premature keratinization in the cell
- Keratin pearls within rete ridges
Cytologic Criteria
- Anisonucleosis: Abnormal variation in nuclear size
- Nuclear pleomorphism: Abnormal variation in nuclear shape
- Anisocytosis: Abnormal variation in cell size
- Cellular pleomorphism: Abnormal variation in cell shape
- Increased nuclear cytoplasmic ratio
- Increased nuclear size
- Atypical mitotic fiures
- Increase in the number and size of nucleoli
- Hyperchromatism
“Early warning signs of issues addressed by understanding tumor pathogenesis: Common questions”
Histopathology
- Classification of epithelial dysplasia is done on basis of its severity which is:
- Mild epithelial dysplasia: It refers to the alteration which is limited to basal and parabasal cell layers.
- Moderate epithelial dysplasia: It shows involvement from basal layer to mid portion of spinous cell layer.
- Severe epithelial dysplasia: It shows alterations from basal layer to the level above mid portion of epithelium.
- When complete thickness of epithelium, term carcinoma in situ is used.
- Histopathological report of leukoplakia should include a statement on absence or presence of epithelial dysplasia.
Thickness Of The Epithelium
In leukoplakia, the thickness of epithelium is altered and it occurs in epithelial atrophy or acanthosis.
Alteration In Underlying Connective Tissue
In leukoplakia there is often variable degree of destruction of collagen fiers and moreover chronic inflammatory cell infitrate is also present in underlying connective tissue stroma.
“Asymptomatic vs symptomatic effects of ignoring benign and malignant oral tumors: Q&A”
“Steps to educate patients about benign and malignant oral cavity tumors and their importance: Q&A format”
Clinical Features
- Usually the lesion occurs in 4th, 5th, 6th and 7th decades of life.
- Buccal mucosa and commissural areas are most frequent affcted sites followed by alveolar ridge, tongue, hard and soft palate, etc.
- Oral leukoplakia often present solitary or multiple white patches.
- Size of lesion may vary from small well localized patch measuring few millimeters in diameter.
- The surface of lesion may be smooth or fiely wrinkled or even rough on palpation and lesion cannot be removed by scrapping.
- Lesion is whitish or greyish or in some cases it is brownish yellow in color due to heavy use of tobacco.
- In most of the cases these lesion are asymptomatic, however in some cases they may cause pain, feeling of thickness and burning sensation, etc.
“Role of counseling in clarifying oral cavity tumor goals for patients: Questions answered”
Question 14.Defie premalignant lesion and condition. Describe etiology, clinical features, and histopathology of oral submucous firosis.
Or
Define precancerous condition and precancerous lesion. Discuss about etiology and histopathology of OSMF.
Answer. The premalignant lesions are defied as morphologically altered tissue in which cancer is more likely to occur then in its apparently normal counter part, e.g. leukoplakia, erythroplakia, nicotiana palati, stomatitis, dyskeratosis congenita, etc.
- The premalignant condition is defied as generalized state of body, which is associated with significantly increased risk of cancer, e.g. oral sub- mucus firosis, syphilis, lichen planus, etc.
Leave a Reply