Buerger’s Disease (Thromboangiitis Obliterans): Causes, Symptoms, and Treatment Options
It is also known as thromboangiitis obliterans or smoker disease.
A chronic recurring, inflammatory, vascular occlusive disease, chiefly of the peripheral arteries and veins of the extremities.
Burger’s Disease Classification
- Type I- Upper limb thromboangiitis obliterans.
- Type II- Involving leg and feet – crural/infrapopliteal
- Type III- Femoropopliteal
- Type IV- Aortoiliofemoral
- Type V- Generalized.

“What Happens If Buerger’s Disease Is Untreated”
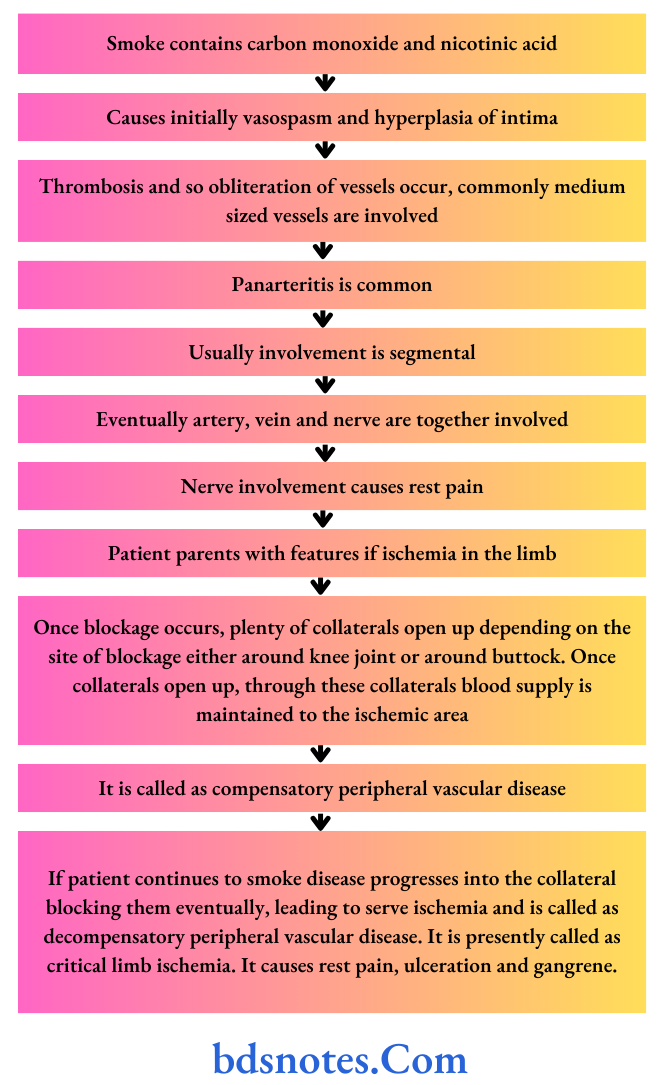
Burger’s Disease Pathogenesis
“Comprehensive Overview Of Buerger’S Disease Symptoms”
Read And Learn More: General Surgery Questions and Answers
Burger’s Disease Clinical Features
- It is common in male smokers between 20 to 40 years of age.
- Intermittent claudication in foot and calf progressing to rest pain, ulceration, and gangrene.
- It includes paresthesia of the foot or pain confined to one toe.
- Easy fatiguability and leg cramps. The leg fatigue quickly especially during walking.
- Ulceration or moist gangrene of hands and feet; amputation may be necessary.
- Recurrent migratory superficial thrombophlebitis
- Absence/Feeble pulses distal to proximal; dorsalis pedis, popliteal and femoral arteries.
Burger’s Disease Diagnosis
Burger’s Disease Criteria of Olin (2000)
- It occurs typically between 20 and 40 years of age in males, although females are also diagnosed.
- History of tobacco use.
- Presence of distal extremity ischemia indicated by claudication, pain at rest, ischemic ulcers, or gangrene. This is documented by noninvasive vascular testing, i.e. ultrasound.
- Exclusion of other autoimmune diseases such as hypercoagulable states and diabetes mellitus by laboratory tests.
- Exclusion of proximal source of emboli by echocardiography and arteriography.
- Consistent arteriographic findings in clinically involved and non-involved limbs.
No laboratory test should confirm the diagnosis of Burger’s disease.
The main goal of various investigations is to exclude other diseases in differential diagnoses.
“Understanding The Causes Of Buerger’S Disease“
Burger’s Disease Treatment
Smoking is strictly stopped.
Burger’s Disease Drugs
- Vasodilators, i.e. nifedipine should be given.
- Pentoxifylline should be given since it increases the flexibility of RBCs so they reach easily in microcirculation.
- Aspirin 75 mg OD is given.
- Analgesics, often sedatives, and antilipid drugs like atorvastatin may be needed.
Burger’s Disease Care of the Limbs
Buerger’s position and exercise: Regular graded exercises up to the point of claudication improve the collateral circulation.
In Buerger’s position, the head end of the bed is raised; the foot end of the bed is lowered to improve circulation. In Buerger’s exercise leg is elevated and lowered alternatively, each for 2 minutes several times at a time.
“Step-By-Step Guide To Managing Buerger’S Disease“
Care of feet: It is better to wear socks with footwear. Heel raise by raising the heels of shoes by 2 cm decreases the calf muscle work to improve claudication.
Burger’s Disease Chemical Sympathectomy
The sympathetic chain is blocked to achieve vasodilatation by injecting a local anesthetic agent (xylocaine 1%) paravertebrally beside the bodies of L 2, 3, and 4 vertebrae in front of lumbar fascia, to achieve temporary benefit.
Long-term efficacy can be achieved by using 5 mL phenol in water.
It is done under C-Arm guidance. The feet will become warm immediately after injection.
Burger’s Disease Surgery
- Omentoplasty to revascularize the affected limb.
- Profundaplasty is done for blockage in profunda femoris artery to open more collaterals across the knee joint.
- Lumbar sympathectomy to increase the cutaneous perfusion to promote ulcer healing. But it may divert blood from muscles towards the skin causing muscles more ischemic.
“Tips To Prevent Complications In Buerger’S Disease”
- Amputations are done at different levels depending on the site, severity, and extent of vessel occlusion. Usually either below—knee or above-knee amputations are done.
- Ilzarov’s method of bone lengthening helps in improving rest pain and claudication by creating neo-osteogenesis and improving the overall blood supply to the limb.
Leave a Reply