Carbuncle: Causes, Symptoms, and Management in Diabetic Patients
The word meaning of carbuncle is charcoal. It is caused by extensive infectious gangrene of the adjacent hair follicle and subcutaneous tissue by Staphylococcus aureus.
- Carbuncle commonly occurs in diabetic patients.
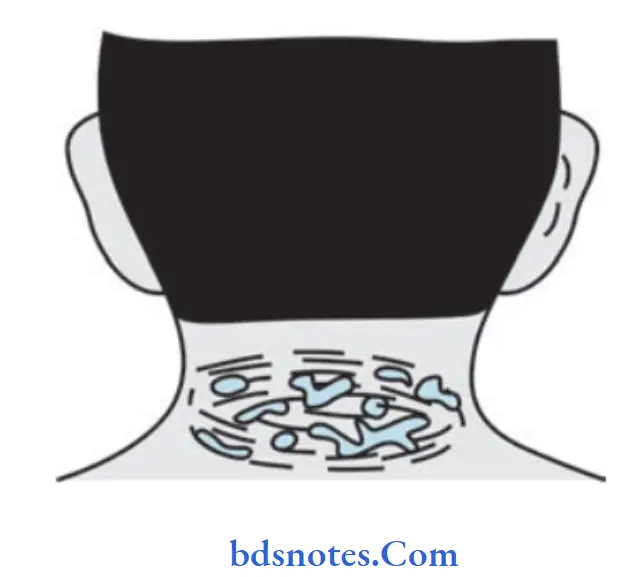
- The Nape of the neck is the most common site followed by the back and shoulder region. The skin of the site is coarse and has poor vascularity.
Carbuncle Pathology

“Does High Blood Sugar Cause Carbuncles“
Carbuncle Clinical Features
- Carbuncle is common in diabetics after 40 years of age
- The surface is red and looks like a red-hot coal.
- Symptoms like fever with chills.
- Severe pain and swelling in the nape of the neck and back.
- The surrounding area is indurated.
- The skin on the center of the carbuncle softens and a peripheral satellite vesicle appears, if rupture discharging pus and giving rise to a cribriform appearance.
- Later, a large crateriform ulcer was developed with a center slough.
“How To Care For A Carbuncle At Home With Diabetes”
Carbuncle Complications
- Worsening diabetic status resulting in diabetic ketoacidosis
- Extensive necrosis of skin overlying carbuncle. Hence, it is included under acute infective gangrene.
- Septicemia and toxemia.

Carbuncle Management
The principles of treatment of carbuncle are:
- Control of diabetes
- Parenteral antibiotics
- Surgical management:
- Diabetes control preferably with injectable insulin.
- Appropriate parenteral antibiotics are given till complete resolution occurs.
Most strains of Staphylococcus aureus are sensitive to cloxacillin, flucloxacillin, erythromycin, and some of the cephalosporins.
However, methicillin-resistant Staphylococcus aureus (MRSA) is resistant to the drugs mentioned above.
They are sensitive only to expensive drug vancomycin which has to be given intravenously. - Improve the general health of the patient
- If the carbuncle does not show any softening or if it shows evidence of healing, it is not incised. It can be left open to the exterior or saline dressings are applied to reduce edema. Complete resolution may take place within 10–l5 days.
“How To Avoid Carbuncle Infections In Diabetes”
Management Of Carbuncle
- Diabetes control preferably with injectable insulin.
- Appropriate parenteral antibiotics are given till complete resolution occurs.
Most strains of staphylococcal aureus are sensitive to cloxacillin, flucloxacillin, erythromycin, and some of the cephalosporins.
However, methicillin-resistant Staphylococcus aureus (MRSA) is resistant to the drugs mentioned above.
They are sensitive only to expensive drug Vancomycin which has to be given intravenously. - Improve the general health of the patient
- If the carbuncle does not show any softening, or if it shows evidence of healing, it is not incised.
It can be left open to the exterior or saline dressings are applied to reduce edema.
Complete resolution may take place within l0-l5 days.
” Carbuncle Care Tips For Better Diabetes Management”
Carbuncle Surgical Management
- Surgery is required when there is pus.
The cruciate incision is preferred because of multiple abscesses and extensive subcutaneous necrosis.
Edges ofthe skin flap are excised, pus is drained, loculi are broken down, the slough is excised, and the cavity is treated with antiseptic agents.
Once the wound granulates well, skin grafting may be required.
Leave a Reply