Epidemiology, Etiology, And Prevention Of Oral Cancer
Question 1. Write a short note on Oral Cancer.
Answer. Cancer is a disease caused by many factors, and it can occur in any site or tissue of the body and may involve any type of cell.
Factors Responsible for Causing Cancer
Oral Cancer Agent Factors
- Physical agents: UV-light, radiation, continuous heat
- Chemical agent: Dyes, liquor or alcohol, arsenic, and nickel.
- Nutritional agent: Deficiency of protein, folic acid deficiency, increased consumption of red chili, deficiency of vitamin A and B, etc.
- Mechanical agent: Chronic irritation, chronic friction, malposed tooth, sharp edge of the tooth, ill-fitting dentures, clasp of partial dentures.
- Biological agents: Viral (HSV and HIV), fungal (Candida).
“Understanding oral cancer: Causes and prevention methods”

“Importance of early detection in preventing oral cancer”
Oral Cancer Host Factors
- Age: The Prevalence of cancer rises with age above 50 years.
- Sex: There is a sex difference in the prevalence of cancer, for example, cancer of the lip is more common in women; cancer of the tongue and buccal mucosa is more common in males.
- Race: White, fair-complexioned individuals have an excessive incidence of cancer of the skin on to face and neck.
- Hereditary: Genetic influence has been suspected in the causation of cancer.
- Occupation: Occupational carcinogens pose a great threat to humans in various industries. A high incidence of cancer has been noticed in textile workers.
- Socioeconomic status: The Majority of patients with oral cancer belong to a socioeconomic group.
Read And Learn More: Public Health Dentistry Question And Answers
- Oral Cancer Custom habits:
- Chewing of tobacco and betel nut, either alone or with lime, causes oral cancer.
- Alcohol consumption may not function as a single factor, may be infect related to other carcinogenic agents.
- Heavy drinking and smoking are frequently associated and may lead to oral and esophageal cancer.
- Smoking increases the likelihood of developing cancer by 2.3 times than nonsmokers.
- Reverse smoking causes leukoplakia and cancer of the palate.
“Common risk factors for oral cancer and how to avoid them”
Oral Cancer Environmental Factors
- Climate: Increased and prolonged exposure to radiation from the sun has been associated with cancer of the skin.
- The actinic rays of the sun may serve as the carcinogenic agent for the cancer of the lip.
- Air Pollution: Oral cancer may be associated with a high degree of industrialization, automobiles and factories, they release number of gases like carbon dioxide, benzopyrene, and polycyclic hydrocarbon-containing fuel.
- Radiation: Increased role of leukoplakia between the dentist and the physician due to overexposure of X-rays.
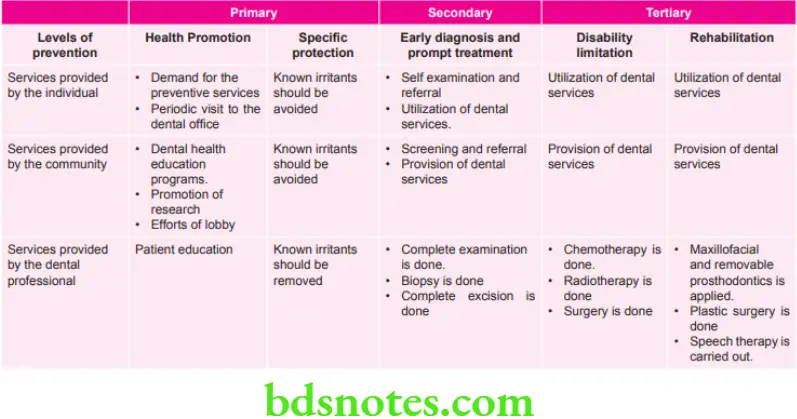
Question 2. Write short note on the prevention of oral cancer.
Answer.
Prevention of Oral Cancer
“Signs that tobacco use increases oral cancer risk”
Question 3. Write short note on importance of social environment in prevention of oral cancers.
Answer. Following is the importance of social environment in prevention of oral cancer
Build Healthy Public Policy
- Tighten restriction on tobacco and alcohol advertising and promotion.
- Subsidize the cost of healthier choices, Example fruits and vegetables.
- Improve labeling on betel quid products.
Create Supportive Environment
- Smoke free public spaces, Example cinemas.
- Increase availability of fresh fruits and vegetables [in school canteen and tuck-shop].
Strengthen Community Action
- Promote establishment of local community based smoking cessation support groups.
- Establish help lines which appeal to population groups with high rate of smoking.
- Support establishment of local food co-operatives selling cheap high quality fruit and vegetables.
Develop Personal Skills
- Expand personal and social education in school-life skills;empowerment, refusal and negotiation skills, etc.
- Incorporate tobacco and alcohol control within healthpromoting schools.
Reorient Health Services
- Expand health professionals education and training insmoking cessation and alcohol control.
- Increase numbers and range of health promotion professional, with expertise in smoking and alcohol support.
- Establish evidence-based smoking and alcohol preventive services with primary care setting.
“Role of smoking cessation in preventing oral cancer”
Question 4. Write in brief etiology and prevention of oral cancer.
Or
Write in brief on etiology of oral cancer.
Answer.
Etiology of Oral Cancer
Tobacco
Smoked and smokeless tobacco contains alkaloid nicotine. Tobacco contains thousands of chemical compounds. These chemical compounds are carcinogens. The most potent carcinogens in tobacco are tobacco-specific nitrosamines, polycyclic aromatic hydrocarbons and many others. For types of smoked and smokeless tobacco in detail, refer to Ans 5 of the same chapter.
Alcohol
Alcohol is the independent risk factor for oral cancer. Combined effect of tobacco and alcohol is greater as compared to their independent effects.
Mouthwashes
Mouthwashes with high alcohol content increase the risk of oral cancer.
Vitamins and Essential Minerals
- Risk of oral cancer is inversely associated with consumption of vitamin A.
- There is presence of association of vitamin C with protective effect against oral, pharyngeal and esophageal cancer.
- Vitamin E like β carotene is an antioxidant. Higher serum vitamin levels appear to be associated with decreased risk of oral cancer.
Ultraviolet Radiation
It is a risk factor for skin cancer of the face and other exposed areas particularly in white skinned individuals.
Chemical Agents
Exposure to chemical agents like aromatic amines, alpha toxin, polycyclic aromatic hydrocarbons are predisposing factors for oral cancer.
Viruses
Infection with human herpes virus-1 may also increase the risk of cancer. Herpes simplex virus-1 and HIV virus are associated with squamous cell carcinoma.
Trauma and Dental Irritation
Continued dental irritation from jagged teeth and dentures, poor oral hygiene are the risk factors for oral cancer.
Genetic Factors
Many gene alterations are implicated in the development and progression of oral squamous cell carcinoma. Expression of genes involved in DNA repair and stability of genome is frequently altered. Genetic changes commonly observed in oral cancer include loss of heterozygosity at the site of known or suspected tumor suppressor genes.
“Biomechanics of HPV infection and its role in oral cancer explained”
Question 5. Discuss the role of various etiological factors in prevalence of oral cancer in India.
Answer. In India tobacco in smoking and non-smoking form play a large role in causation of cancer in India. Alcohol along with tobacco provides synergistic effect in causation of cancer. The etiological factors which lead to prevalence of oral cancer in India are as follows:
Smoking Tobacco
- Bidi: It is the most popular form of smoking tobacco in India. Total production of tobacco in India about 34% is used in manufacturing of bidis. Bidi smoking is most common in rural areas of India. Tendu leaf is used for making bidi. In it 0.2–0.3 g of tobacco flakes kept and the Tendu leaf is rolled as well as tied by a thread. It consists of 1.7–3g nicotine and 45–50 g of tar.
- Cigarette: About 31% of tobacco grown in India is used for manufacturing of cigarettes. Cigarette smoking is most common in urban areas in India. 1 g of cured tobacco in sun or by artificial heat is covered with paper. It consists of 1–1.4 mg of nicotine and 19–27 g of tar.
- Reverse Chutta smoking: In this smoking of tobacco is done with lightened end inside the mouth. In India it is most commonly done in Vishakhapatnam and Srikakulum district of Andhra Pradesh. In Telgu language, this habit is known as “adda poga”. It is also consumed in parts of Odisha. Coarsely prepared cheroots are made by rolling tobacco leaf in cylindrical shape and one end is tied with a thread.
- Dhumti: This habit is most prevalent in Goa. In this tobacco leaf is rolled inside the leaf of jack fruit tree. It is used for reverse smoking.
- Hookli: It is most commonly used in district Bhavnagar Gujarat. It is a clay pipe which is 7–10 cm long with mouth piece and bowl.
- Hookah: It is used in the areas in India where strong Mughal culture influence is present. Tobacco which is smoked is withdrawn by water which lies in base of hookah, and it cools and filters the smoke.
Smokless Tobacco
- Khaini: It is the combination of powdered sun-driedtobacco and slaked lime paste. In India, the habit is most common in Maharashtra and in Bihar as well as some other states of North India too.
- Manipuri Tobacco: It is the combination of tobacco, slaked lime, finely cut areca nut, camphor and cloves. It is commonly used in India in villages of Uttar Pradesh.
- Mawa: It is the combination of tobacco, slaked lime and shavings of areca nut. In India, it is most commonly used in Bhavnagar district in Gujarat.
- Mishri: It is the roasted form of tobacoo. It is commonly used in Maharashtra state.
- Paan: It is the betel leaf which consists of areca nut, lime, catechu, and condiments. This habit is prevalent all over in Indian subcontinent.
- Gudakhu: It is in the paste form and consists of powdered tobacco, molasses and various other ingredients. It is most commonly used in Bihar.
- Snuff: It consists of finely powdered air-cured and firecured tobacco leaves. It can be dry or moist. In India it is commonly used in Bajjar district in Gujarat.
“Steps to reduce oral cancer risk through lifestyle changes”
Question 6. Write short note on laws for tobacco control.
Answer. A comprehensive tobacco control legislation titled “The Cigarettes and other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and Commerce, Production, Supply and Distribution) Act, 2003” was passed by the Parliament in April, 2003 and notified in Gazette of India on 25th Feb 2004. The important provisions the Act are:
- Prohibition of smoking in public areas.
- Prohibition of indirect and direct advertisement of cigarette and other products.
- Prohibition of sale of cigarette and other tobacco products to a person below age of 18 years.
- Prohibition of sale of tobacco products near the educational institutions.
- Mandatory depiction of statutory warnings (including pictorial warnings) on tobacco packs, and
- Mandatory depiction of tar and nicotine contents along with maximum permissible limits on tobacco packs.
The rules related to prohibition of smoking in public places came into force from 2nd October 2008. As per rules, it is mandatory to display smoke free signage at all public places. Labeling and packaging rules mandating the depiction of specified health warning on all tobacco product packs came into force from 31st May 2009.
“Role of a healthy diet in preventing oral cancer”
Question 7. Write short answer on epidemiology of oral cancer.
Answer. Oropharyngeal cancer is more common in developing as compared to the developed countries.
- Oral cancer is the eighth most common cancer worldwide.
- Prevalence of oral cancer is particularly high among men.
- Incidence rates for oral cancer vary in men from 1 to 10 cases per 1 lakh population in many countries.
- In south central Asian continent, oral cancer is among the three most common types of cancer.
- Age standardized incidence rate or oral cancer per 100,000population ranges from 0.7 in China to 4.6 in Thailand and 12.6 in India.
- It was also seen that there is sharp increase in the incidence rates of oral cancer have been reported in countries such as Denmark, France, Germany, Scotland, central and eastern Europe and to a lesser extent in Australia, Japan, New Zealand and USA.
- High incidence rate of oral cancer is related directly to risk behaviors i.e. smoking, use of smokeless tobacco and alcohol consumption.
- In studies it is estimated that over 47% of Indians whose age is 15 years or more use tobacco in one form or another.
- A wide variety of oral mucosal changes due to the usage of tobacco has been observed in more than 50% of tobacco users. A dose-response relationship has been shown between tobacco chewing habit and oral cancer. The risk among those who chewed less than 2 times a day was 8.4, among those who chewed more than 6 times a day was 17.6 and those who retained the quid overnight had a risk of equal to or less than 63.
- An increased risk of the oral cancer is seen in those who only chew as compared to those who only smoke. A greater risk is seen in those persons who have the habit of both chewing and smoking.
- Mainly oral cancer is seen in the older age group during 5th and 6th decade of life.
- In India, National Cancer Registry Programme (NCRP) was carried out by Indian Council of medical Research (ICMR) with network of cancer registries all around the country in December 1981. Coordinating unit of NCRP provide guidelines and quality control checkup to the current network of population which is based on hospital based cancer registries of NCRP. This data is helpful in planning National Cancer Control programme.
- Based on the available data, males in Bhopal have highest rate of Tongue cancer i.e. 8.8 per 1 lakh.
- Rates of oral cancer in both man and woman in urban registries are highest in the world.
Leave a Reply