Orthodontic Diagnosis
Enumerate diagnostic aid. Discuss any two in detail.
Or
Write short note on essential diagnostic aids.
Answer.
Diagnostic Aids
Essential Diagnostic Aids
- Case selection
- Clinical examination
- Study models
- Certain radiographs:
- Periapical radiograph
- Bitewing
- Panoramic.
- Facial photographs
“Understanding the role of orthodontic diagnosis in treatment planning: Q&A explained”
Read And Learn More: Orthodontics Question And Answers
Nonessential or Supplemental Diagnostic Aids
- Specialized radiographs:
- Cephalometric radiographs
- Occlusal intraoral films
- Selected lateral jaw view
- Cone shift technique.
- Electromyographic examination of muscle activity.
- Hand and wrist radiographs to assess bone age.
- Endocrine tests.
- Estimation of basal metabolic rate.
- Diagnostic set-up.
- Occlusograms
- Sensitivity (Vitality) test
- Biopsy.
“Importance of studying orthodontic diagnosis for better outcomes: Questions explained”
Essential Diagnostic Aids
Following are the essential diagnostic aids
- Case history
- Clinical examination
- Study models
- Certain radiographs
- Periapical radiographs
- Bitewing
- Panoramic
- Facial photographs
“Common challenges in performing orthodontic diagnosis effectively: FAQs provided”
Case History
It consists of information which is gathered from the patient and parent or guardian which aid in complete diagnosis of the case. Case history has various personal details, chief complaint, present and past dental as well as medical history and the associated family history.
Personal Details
- Name: Name of the patient should be recorded for communicating and identifiation the patient and also addressing patient by his/her name which has positive beneficial psychological effct on patient.
- Age: The chronological age of patient helps in both i.e. diagnosing and treatment planning. Various treatment protocols are directed by the age of patient such as growth modification by using functional and orthopedic appliances which are best to be done at growth period while surgical procedures are carried out aftr completion of growth.
- Sex: This is very important as the timing of growth is different in both males and females.
- Address and occupation: They are very useful in communication and evaluation of socioeconomic status of patient.
Chief Complaint
- This should be recorded in patient’s own words.
- It helps clinician to identify priorities and desires of patient which helps in settng the treatment objectives which can satisfy patient as well as their family.
Medical History
- Few of the medical conditions contraindicate use of orthodontic appliances.
- Some of the physical conditions need various precautionary measures to be taken before to or during orthodontic therapy. E.g. antibiotic coverage is required in patient with rheumatic fever or cardiac diseases.
Dental History
- Past dental history helps to assess the parent’s and parent’s atttude towards dental health as well as dental treatment.
- Dental history consists of information on age of eruption of deciduous and permanent teeth, history of extraction, decay restoration and trauma to dentition.
“Steps to explain different types of orthodontic diagnosis: Clinical vs radiographic: Q&A guide”
Prenatal and Postnatal History
- It consists of information on condition of the mother at the time of pregnancy and the type of delivery.
- Usage of certain teratogenic drugs such as thalidomide, some infections such as German measles at the time of pregnancy lead to congenital deformities of child.
- Forceps delivery leads to TMJ injuries and mandibular growth retardation.
- Postnatal history includes type of feeding, presence of habits.
Family History
This record the details of malocclusion which occur in other members of the family, which provide the clue of inherited conditions e.g. Skeletal Class II and Class III malocclusion, congenital conditions such as clef lip and clef palate.
Clinical Examination
It consists of following points:
- General examination
- Extraoral examination
- Intraoral examination
General Examination
It consists of general assessment of the patient and begins as soon as patient enters the clinic. It consists of
- Height and weight: Both height and weight of the patient should be noted. They give a clue to physical growth and maturation of patient which have dentofacial correlation.
- Gait: This is the manner in which patient walks. Abnormalities of the gate are associated with neuromuscular disorders which have dental correlation.
- Posture: It refers to the way a person stand. Abnormal postures predispose to malocclusion because of alteration in maxilla – mandibular relationship.
- Body built: Sheldon classifid it as:
- Ectomorphic: Tall and Thin physique
- Mesomorphic: Average physique
- Athletic: Short and obese physique
“Role of cephalometric analysis in orthodontic diagnosis: Questions answered”
Extraoral Examination

“Early warning signs of issues detected through orthodontic diagnosis: Common questions”
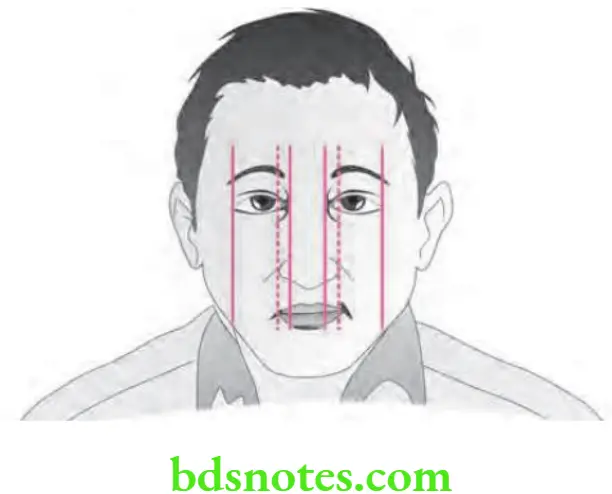
Assessment of facial symmetry
- For facial symmetry the examination is carried out in frontal and lateral views.
- In frontal plane intercanthal width is equal to width of nose.
- Proportionwise the ideal face is divided into central, medial and lateral equal fits. Nose and chin lies in center in central fit.
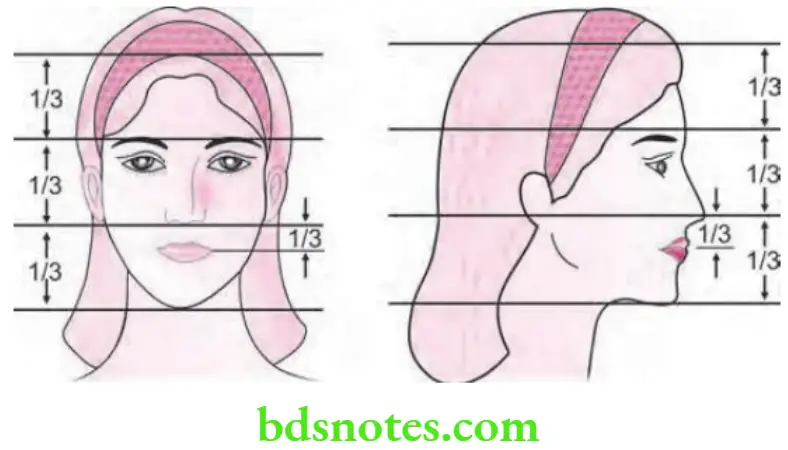
- In vertical plane the nasal length is one-third of the complete facial height.
- Nasal contour can be straight and convex.
- Vertical height of midface is equal to height of lower face.
- In lower face mouth is equal to one-third of the distance between nose and chin.
- Height of forehead is measured from hairline to glabella. Forehead is of two types, i.e. flt and steep.
- If face is normally balanced it consists of equal upper face height, middle face and lower facial height.
“Asymptomatic vs symptomatic effects of ignoring orthodontic findings: Q&A”
Facial profile
- Facial profile is examined by viewing the patient from the side.
- Facial profile helps in diagnosing gross deviations in the maxillomandibular relationship.
- The profile is assessed by two reference lines and three landmarks:
- Three landmarks are used which are: sof tissue nasion, nasion and sof tissue pogonion.
- Two reference lines are
- First line is dropped from sof tissue nasion to subnasale
- Second line is dropped from subnasale to soft tissue pogonion
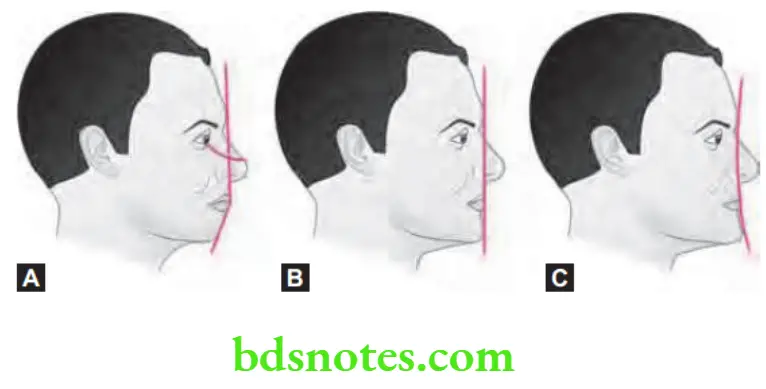
- So, based on the relationship of two lines and the three landmarks the facial profie exists as:
- Straight profie: Two lines form a nearly straight line.
- Convex profile: Two lines form an angle with the concavity facing the tissue.
- Concave profie: Two reference lines form an angle with the convexity towards the tissue.
“Can targeted adjustments improve outcomes based on orthodontic diagnosis? Answer provided”
Facial divergence
Facial divergence is defied as an anterior or posterior inclination of the lower face relative to the forehead.
- Facial divergence can be of three types:
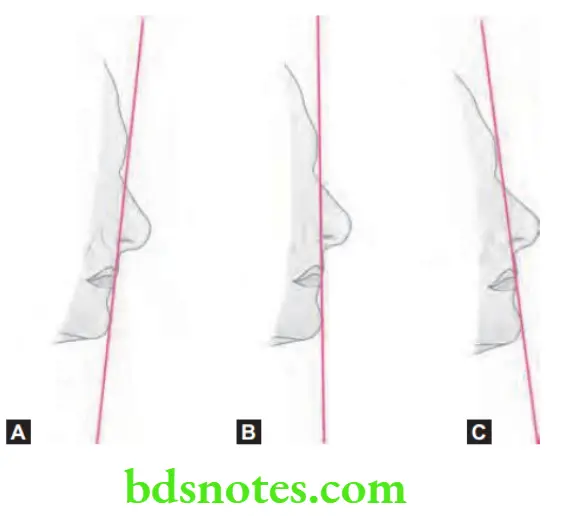
- Anterior divergent: A line drawn between the forehead and chin is inclined interiorly seen in class III cases.
- Posterior divergent: The line stands posterior towards chin seen in class II cases.
- Straight or orthognathic: The line between the forehead and chin is straight seen in class I cases.
- It uses two soft tissue landmarks, i.e. soft tissue nasion and soft tissue pogonion.
Examination of lips
- In a balanced face upper lip is protruded slightly in relation to lower lip.
- When upper lip is at rest the 2 mm of incisal edges of maxillary incisors is seen at rest.
- Lip should be examined for the habits such as lip thrust, lip competency, lip insuffiency, abnormal lip habits.
- Lip competency is confiured as:
- Competent lips: Lips are in slight contact when the musculature is relaxed.
- Incompetent lip: They are morphologically short lips which do not form a lip seal in a relaxed state.
- Potentially incompetent lips: They are normal lips that fail to form a lip seal due to proclaimed upper incisors.
- Everted lips: They are hypertrophied lips with weak muscular tonicity.
“Early warning signs of knowledge gaps in patient understanding of orthodontic diagnosis: Common questions”
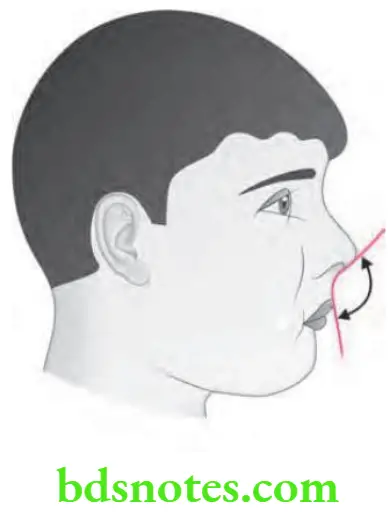
Nasolabial angle and incisor protrusion
- Nasolabial angle (NLA) is the angle which is formed by the tangent to base and to upper lip.
- Normal nasolabial angle is 110°.
- With proclination of maxillary incisors angle NLA decreases.
- With retroclination of maxillary incisors angle NLA increases.
“Steps to educate patients about orthodontic diagnosis and its importance: Q&A format”
Clinical Frankfort mandibular plane angle
- Inclination of mandibular plane angle to the Frankfort horizontal plane is measured.
- It is done by, over the patient’s face a scale is kept over Frankfort plane. Second scale is kept along the lower border of mandible.
- Area where the posterior parts of two scales meet should be recorded.
- If the posterior ends of angle meet behind auricle or in occiput it means angle is high.
- In cases with long face and open bite, the mandibular plane angle become steep.
- In cases with short faces and skeletal deep bite the mandibular plane angle become flt.
Examination of nose
It contributes to the aesthetic appearance of the face:
- Nose size: Normally the nose is one third of the total facial height.
- Nose contour: Shape of nose can be straight, convex or crooked due to nasal injuries.
- Nostrils: It is oval and bilaterally symmetrical.
“Asymptomatic vs symptomatic effects of poor communication about orthodontic diagnosis: Answered”
Examination of chin
- Mentolabial sulcus: It is concavity seen below lower lip. Deep mentolabial sulcus is seen in Class II division 1 malocclusion but is shallow in bimaxillary protrusion.
- Mentalis activity: Normally mentalis muscle shows no contraction when at rest. Hyperactive mentalis is seen in Class II division 1 cases. It leads to puckering of chin.
- Chin position and prominence: Prominent chin is associated with Class III malocclusion while recessive chin is common in class II malocclusion.
Intraoral examination
- Mouth opening: Intraoral examination begins with measurement of the mouth opening. Normal mouth opening is 45 to 55 mm for adults and less than 45 mm for children.
- Tongue: Presence of excessively large tongue is indicated by presence of imprints of teeth over the lateral margin of tongue giving it a scalloped appearance. Patient whose tongue reaches till tip of nose has long tongue. Lingual frenum is examined for tongue tie.
- Palate: Following findings should be examined on palate:
- Variation present in palatal depth occurs in association with the variation of facial form. Dolichofacial patients have deep palate.
- Presence of swelling in the palate indicates an impacted tooth, presence of cysts or bony pathology.
- Mucosal ulceration and indentations are the features of traumatic deep bite.
- Presence of cleft in palate is associated with discontinuity of palate.
- Third palatal rugae is in the line with canines which help in assessment of maxillary anterior proclination.
“Can interactive tools improve adherence to orthodontic-based plans? FAQs provided”
- Gingiva: It is examined for inflmmation, recession and other mucogingival lesions.
- Frenal attchment: Due to thick maxillary labial frenum, midline diastema may arise. High attachment of mandibular labial frenum causes gingival recession.
- Tonsils and adenoids: Size and degree of inflammation of any of the tonsils should be examined. Abnormally inflamed tonsils causes alteration in tongue and the jaw posture, upsetting the orofacial balance causing malocclusion.
- Dentition: It should be examined and following details should be recorded:
- Teeth present inside the oral cavity.
- Unerupted teeth
- Missing teeth
- Status of dentition i.e. erupted and non-erupted tooth
- Presence of dental caries, restorations, malformations, hypoplasia, wear and discoloration
- Ask the patient to close the jaws in centric occlusion and determine the molar relation which is described as Angle’s Class I, II and III.
- Overjet and overbite are recorded. If any variation is present, it should be recorded.
- Transverse malrelations i.e. crossbite and shif in upper and lower midline should be looked.
- Individual tooth irregularities i.e. rotations, displacement, intrusion and extrusion are noted.
- Maxillary and mandibular arches are examined to study their arch form as well as symmetry.
Study Models
Study casts are essential diagnostic aids.
- Orthodontic study models are accurate plaster reproduction of the teeth and their surrounding soft tissues.
- Study models are three dimensional view of the maxillary and mandibular dental arches.
“Role of counseling in clarifying orthodontic goals for patients: Questions answered”
Ideal requisite of study model
- Models should accurately reproduce the teeth and their surrounding sof tissue without any distortion.
- Models are to be trimmed in such a manner that they are symmetrical and pleasing to the eye. This enables instant identifiation of asymmetries in the arch form.
- Models are to be trimmed in such a way that when replaced on their backs, they accurately reproduce the occlusion.
- Study model should have a clean, smooth and nodule free surface.
- Study models should not only depict the teeth but should also reproduce as much of the alveolar process as possible.
Use of study models
- They enable the study of occlusion from all aspect.
- They enable accurate measurement to be made in a dental arch. They help in measurement of arch length, arch width and tooth size.
- They help in assessment of treatment progress by dentist as well as the patient.
- They help in assessing the nature and severity of malocclusion.
- They are helpful in motivation of the patient and to explain the treatment plan as well as progress to the patient and parents.
- Study models make possible to stimulate treatment procedure on the cast such as mock surgery.
- Study models are useful to transfer records in case the patient is to be treated by another clinician.
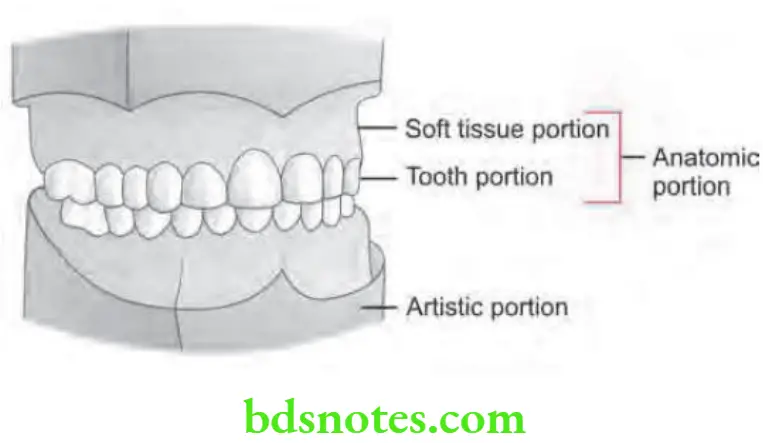
Parts of a study model
- Anatomic portion
- Artistic portion.
- Anatomic portion: The anatomic portion is that part of the study model which is the actual impression of the dental arch and its surrounding structures. Anatomic portion is usually made of stone plaster.
- Artistic portion: This part consists of a plaster base that supports the anatomic portion.
“How do educational materials explain complex orthodontic concepts? FAQ explained”
Leave a Reply