Management Of Cleft Lip And Palate
Write short note on Veau’s classification of cleft lip and palate.
Answer. Veau proposed the most widely used classification.
Veau’s Classification of Cleft lip and cleft palate
Read And Learn More: Orthodontics Question And Answers
“Understanding the role of management in treating cleft lip and palate: Q&A explained”
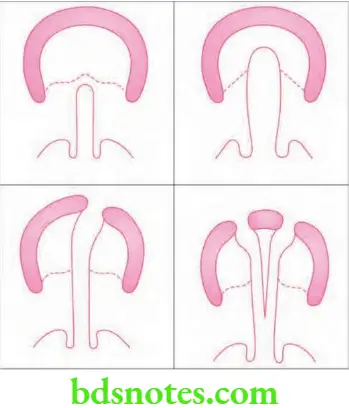
He classified cleft into four groups:
“Importance of studying cleft lip and palate for better outcomes: Questions explained”
- Group 1: These are the clef which involve soft palate only.
- Group 2: They are the clefts of hard and soft palate extending up to incisive foramen.
- Group 3: They are complete unilateral cleft which involve soft palate, hard palate, lip and alveolar ridge.
- Group 4: They are complete bilateral cleft affecting the soft palate, the hard palate, the lip and alveolar ridge.
“Common challenges in managing cleft lip and palate effectively: FAQs provided”

Leave a Reply