Infections Of Oral Cavity And Oral Sepsis Question And Answers
Question 1. Write short note on radiographic diagnosis of chronic suppurative osteomyelitis of mandible.
Answer. Chronic osteomyelitis is persistent abscess of bone, i.e. characterized by usual complex inflammatory process including necrosis of mineralized and marrow tissues, suppuration, resorption, sclerosis and hyperplasia.
Chronic Suppurative Osteomyelitis Of Mandible Radiographic Diagnosis
- There is presence of single or multiple radiolucencies of variable size.
- Outline is irregular and poorly defined borders are present.
- Moth-eaten appearance is present and become irregular in outline and separate by islands of normal appearing bone.
- Sequestra: Necrotic bone segments get detached and irregular calcified areas get separated from remaining normal bone which is known as sequestra. These are more dense and are well appreciated.
- Roots of teeth undergo external resorption.
- Lamina dura may become less apparent as it blends with surrounding granular sclerotic bone.
- Fistula tracts may appear on radiograph as radiolucent bands transversing body of jaw and penetrating cortical plates.
- In patients with extensive chronic osteomyelitis disease may spread to mandibular condyle and joint resulting in septic arthritis.
- Main radiographic feature of suppurative osteomyelitis is an expanding radiolucent osteolytic change instead of potential for peripheral sclerosis.
“Understanding oral cavity infections through FAQs: Q&A explained”
Read And Learn More: Oral Medicine Question And Answers
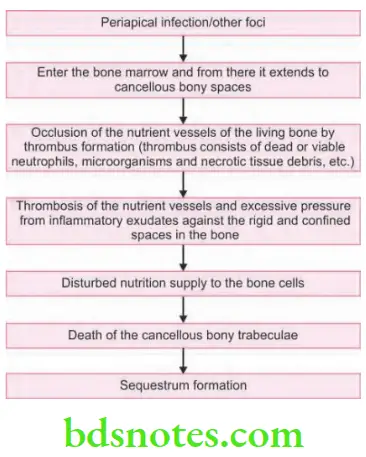
Question 2. Write note on sequestrum.
Answer. Sequestrum is a piece of necrotic bone.
- Sequestrum is avascular and consists of microorganisms.
- Sequestrum should be excised, or else if not removed they infect the surrounding tissue which leads to weakening of bone and can cause pathological fracture.
- Radiographically, it appears as necrotic bone which get detached from remaining bone. Sequestrum appears more dense as compared to normal bone.
“Importance of studying oral infections for better diagnostic outcomes: Questions explained”
Sequestrum Pathogenesis
“Common challenges in diagnosing oral cavity infections effectively: FAQs provided”
Question 3. Write short note on osteomyelitis.
Answer. Greek word “osteon” means bone “myelos” marrow and “itis” means inflammation.
Osteomyelitis may be defined as an inflammatory condition of bone that begin as an infection of medullary cavity and haversian system of the cortex and extends to involve the periosteum of the affected side.
Classification of Osteomyelitis
- Acute Osteomyelitis
- Acute suppurative osteomyelitis
- Acute subperiosteal osteomyelitis
- Acute periostitis
- Chronic Osteomyelitis
- Non-specific Type
- Chronic intramedullary osteomyelitis
- Chronic focal sclerosing osteomyelitis
- Chronic diffuse sclerosing osteomyelitis
- Chronic osteomyelitis with proliferative periostitis
- Chronic subperiosteal osteomyelitis
- Chronic periostitis
- Specific type
- Tuberculous osteomyelitis
- Syphilitic osteomyelitis
- Actinomycotic osteomyelitis
- Radiation induced osteomyelitis
- Idiopathic osteomyelitis.
“Steps to explain causes of oral cavity infections: Bacteria vs viruses: Q&A guide”
Osteomyelitis Clinical Features
Acute Osteomyelitis
- Onset is rapid and patient complaints of severe pain, Paresthesia or anesthesia of mental nerve.
- Initially swelling is absent, teeth are not mobile and fistulae are absent.
- As its course advances there is presence of deep intense pain, fever, anorexia, malaise and regional lymphadenopathy.
- Patient complaints of loosened teeth and fetid odor.
- In its advance stage pus exudes around the gingival sulcus or via mucosal fistula.
“Role of poor oral hygiene in causing oral infections: Questions answered”
Chronic Osteomyelitis
- Its onset is insidious with slight pain, there is slow increase in size of jaw along with the development of sequestra without fistula.
- It is painless till acute or Subacute exacerbation occur.
- Necrotic bone can be visible in oral cavity.
- There is development of intraoral and extraoral sinus which drains pus and heals gradually.
- In the area of abscess, there is development of local tenderness and swelling.
- There is presence of regional lymphadenopathy.
Osteomyelitis Radiographic Features
Acute Osteomyelitis
- After 10 days of acute infection, density of trabeculae decreases and it appear blur and fuzzy. This is the earliest radiographic change.
- Multiple radiolucencies appear on the radiograph. These are enlarged trabeculae spaces due to foci of necrosis and frank bone destruction.
- There is presence of saucer shaped area of destruction having irregular margins with teeth along with the variable amount of supporting bone.
- Periosteal reaction is seen which appear as thin, faint, radiopaque line which is adjacent and almost parallel or slightly convex to surface of bone.
- Loss of continuity of lamina dura is present.
Chronic Osteomyelitis
For details refer to Ans 1 of same chapter.
Osteomyelitis Diagnosis
- Clinical diagnosis: There is presence of fever, malaise, swelling and pain on the affected region.
- Radiological diagnosis: Presence of saucer shaped defect, loss of lamina dura, moth eaten appearance and formation of sequestrum.
- Laboratory diagnosis: On microscopic examination, the medullary spaces are filled with inflammatory exudates. Main inflammatory cells present are polymorphonuclear leukocytes and occasionally lymphocytes and plasma cells can be seen.
- Investigations: Gram staining, Mantoux test, WBC count and complete hemogram, culture and sensitivity.
“How does untreated dental caries lead to oral sepsis? FAQ explained”
Osteomyelitis Management
- As early diagnosis is formulated, drainage of fluctuant areas is carried out in presence of antibiotics. As pus get evacuated, place the drains.
- Thorough debridement of the affected area is done by hydrogen peroxide and saline.
- Empiric therapy
- 1st Regimen: I.V. Aqueous penicillin 2 million units 4 hourly along with I.V. oxacillin 1 g 4 hourly.
- 2nd Regimen: If patient remains asymptomatic after 2 or 3 days, penicillin V 500 mg, 6 hourly along with dicloxacillin 250 mg 4 hourly for 2 to 4 weeks.
- Definitive therapy: Culture and sensitivity test should be done and antibiotic should be modified according to the results. If response is favorable do not undergo any change.
- Extraction: Carious teeth along with periapical infection should be extracted.
- Provide adequate rehydration along with rich nutritional diet and multivitamin therapy.
- Sequestrectomy: This is the removal of sequestra.
- Saucerization: Margins of the necrotic bone should be excised. It is done under local anesthesia after raising the buccal flap.
- Decortication: Here the removal of inferior cortical plates is done, 1 to 2 cm beyond the area of involvement.
- Hyperbaric oxygen therapy is widely used recently.
“Early warning signs of issues addressed by understanding oral infection pathogenesis: Common questions”
Question 4. Write short note on Garre’s Osteomyelitis.
Answer. It is also known as chronic osteomyelitis with proliferative periostitis.
Garre’s osteomyelitis represents a reactive periosteal osteogenesis in response to low-grade infection or trauma.
The condition was first reported in 1893 by German physician Carl Garre and it is characterized by focal gross thickening of the involved bone due to subperiosteal new bone deposition.
Garre’s Osteomyelitis Clinical Features
- Age: Children and young adults (mean age 13 years).
- Sex: There is no sex predilection.
- Site: Mandible is commonly involved in Garre’s osteomyelitis in its posterior part. Maxilla can be affected on rare occasion.
- The involved jaw bone often presents grossly carious, non-vital tooth.
- The tooth is always associated with periapical or sometimes other inflammatory foci.
- There is thickening and swelling of affected bone with little or no pain.
- The size of the swelling may be ranging from centimeters to a lesion spanning the entire length of the mandible.
- The thickness of the bone may be up to l cm.
- Occasionally, slight tenderness or a vague pain may be felt in the affected area of bone.
- Garre’s osteomyelitis is generally a solitary lesion, however multifocal lesions are sometimes reported.
- Slight pyrexia and moderate leukocytosis is present but the erythrocyte sedimentation rate (ESR) is normal.
“Role of counseling in clarifying goals for managing oral infections: Questions answered”
Garre’s Osteomyelitis Radiographic Features
- Garre’s osteomyelitis radiographically presents a central jaw lesion with a mottled, predominantly radiolucent appearance, the lesion often has few radiopaque foci.
- The affected periosteum forms several layers of reactive vital bone and as a result the expanded cortex of bone radiographically exhibits many concentric or parallel opaque layers, which often produce a typical “onion skin” appearance.
- These concentric bone laminations may be as many as 12 in numbers, these are roughly parallel to each other and the underlying cortical surface of bone.
- The standard occlusal radiograph reveals a smooth, convex, bony overgrowth on the outer cortex of the jaw. This is often called as ‘duplication’ of the cortex.
- Few newly formed bony trabeculae are often oriented perpendicular to the “onion skin” layers.
“Steps to educate patients about oral infections and their importance: Q&A format”
Garre’s Osteomyelitis Differential Diagnosis
- Osteosarcoma: Its radiographic appearance is of sunray type.
- Ewing’s sarcoma: Enlargement of bone by sarcoma is very rapid. Radiographic appearance is of Sun-ray type.
- Fibrous dysplasia: More commonly affected bone is maxilla.
- Infantile cortical hyperostosis: Expansion of cortices of many bones is seen.
- Caffey’s disease: This is seen at angle or ramus of mandible and present before the age of 2 years, and this develops in more than one bone.
Oral Sepsis: Symptoms, Causes, and Treatment Options
Treatment
- Removal of the causative agent.
- Extraction of offending tooth and antibiotic therapy
- Cortical swelling undergoes spontaneous physiologic remodeling and does not require any surgical intervention.
“Asymptomatic vs symptomatic effects of ignoring oral infection triggers: Q&A”
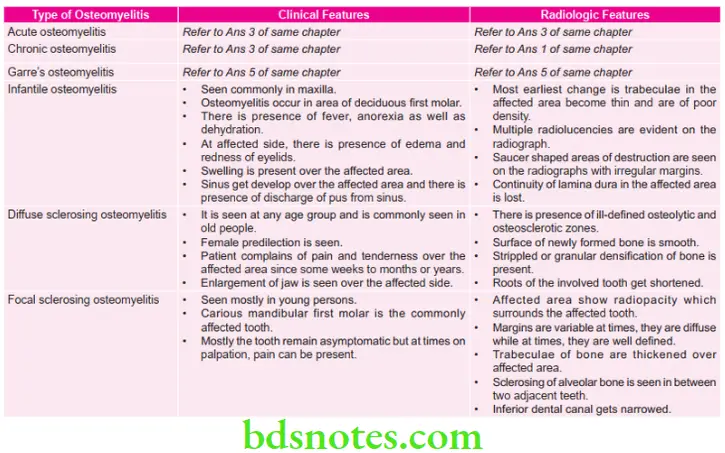
Question 5. Give clinical and radiologic features of osteomyelitis of jaws.
Answer. Following are the clinical and radiologic features of osteomyelitis of jaws:
Leave a Reply