General Surgery Practical Exam Question And Answers
General Surgery Practicals Long Cases
Ulcer:
Ulcer History:
Mode of onset – ask whether developed following trauma or spontaneously; initially swelling and then ulcerated (LN masses, tumors); and varicose veins, vascular insufficiency; developed over the rear of a burn, post-irradiation.
“Understanding general surgery practical exams through FAQs: Key concepts explained”
Ulcer Duration:
- Pain – only inflammatory ulcers are painful; syphilitic and trophic ulcers resulting from nerve diseases (tabes dorsalis, transverse myelitis, peripheral neuritis) are painless, malignant ulcers initially are painless but later become painful due to infiltration.
- Ulcer Discharge:
- Serous callous, healing ulcer
- Sero sanguineous
- Bloody
- Purulent – spreading ulcer.
“Importance of studying general surgery practical exam notes for medical students: Questions explained”
- H/o complications – bleeding, deformity, malignant transformation etc.
- Progress of the ulcer
- Associated diseases T. Dorsalis, syringomyelia, Transverse myelitis, peripheral neuritis, Tb, Nephritis, DM, syphilis (primary stage – chancre), Leprosy, RA; Blood dyscrasias like sickle cell anemia.

“Common challenges in mastering general surgery practical exams effectively: FAQs provided”
Ulcer General Examination:
- Nutritional status – evidence of anemia, hypoproteinemia, Avitaminosis, and obesity.
- Syphilitic stigmata.
- Evidence of Tb, atherosclerosis, and peripheral nerve thickening.
Ulcer Local Examination:
Local Examination Inspection:
- Size and shape
- TB oval or circular but coalescence to irregular
- Syphilitic circular or semilunar which later becomes serpiginous
- Varicose ulcer- oval
- Malignant – irregular.
- General Surgery
- Number – Tb. Ulcers, gummatous, varicose, and soft chancres are often in multiple positions.
“Why are practical exam Q&As critical for general surgery success? Answered”
Local Examination Edge (PURSE):
- Punched out – gummatous, tropie ulcers (do not intend to spread to the surroundings)
- Undermined – Tb (due to relatively more rapid destruction of subcutaneous tissue than the overlying skin).
- Raised and pearly white – rodent ulcer (feature of invasive ulcers)
- Sloping Healing, traumatic, venous (signifies the ulcer is healing and epithelium is approaching from sides).
- Everted (Rolled out) – Squamous cell carcinoma (because of abnormally fast tissue growth, overhangs over the normal epithelial margin).
Local Examination Floor:
- Red granulation tissue
- Pale and smooth granulation tissue – is a feature of very slow healing ulcer.
- Wash leather slough – gummatous ulcer.
- Black mass-malignant melanoma.
- Surrounding area, see for features of inflammation, eczema, pigmentation and scars.
- Affected lymph nodes are usually enlarged and may be tender.
Local Examination Palpation:
- Tenderness – acutely inflamed ulcers are usually tender; chronic ulcers like Tb, syphilitic etc are slightly tender; varicose ulcer may or may not be tender; neoplastic ulcers are non tender.
- Edge and margin – see for degree of induration.
- Base.
- Depth – trophic ulcers are usually deep to reach the bone.
- Bleeding – on touch – malignant ulcer.
- Relation with deeper structures – try to move the ulcer over the structures; in case of gummatous and neoplastic the ulcer is fixed.
- Surrounding skin – see for temp and tenderness, fixity, sensation.
- Peripheral nerve thickening or tenderness.
- Peripheral arteries.
- State of veins.
“Factors influencing success with general surgery practical exam knowledge: Q&A”
Lymph nodes:
Lymph nodes In TB:
- In hunterian chancre discrete, firm
- In gummatous and rodent ulcer
- In malignant – stomy hard and fixed.
- Examination for vascular insufficiency
- Examination of nerve lesion.
Lymph nodes General examination:
- Involvement of liver, lungs etc in malignancy
- Peripheral pulses – in trophic ulcers
- Source of infection
- Diabetes.
Lymph nodes Investigations:
- Routine blood tests
- Urine – for sugars and ketone bodies (DM)
- Smear of discharge, discharge for C/S
- Skin test montoux
- Chest X-ray-Tb, rule out metastasis
- Biopsy.
Lymph nodes Important points:
- An ulcer is a breach or discontinuity of an epithelial surface due to gradual but progressive destruction of the tissue cell.
- Margin of an ulcer denotes the junction between the normal and the ulcerated area; can be round, oval or irregular.
- It has three different zones
- Red-healing zone and reflects gr. Tissue
- While – area of fibrous tissue
- Blue – junction between the two.
- Floor- exposed part; feature of inspection.
- Base – is the structure on which ulcer lies; feature of palpation.
- Edge – part of the ulcer between the floor and the margin.
“Steps to explain general surgery practical exams: Anatomy vs techniques vs procedures: Q&A guide”
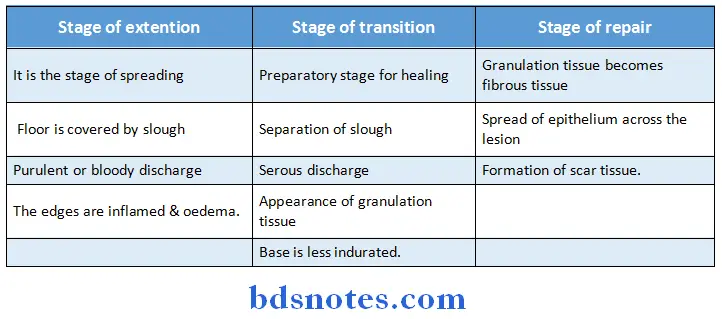
Question 1. What are the stages in an ulcer development and healing?
Answer:
An ulcer passes through three stages:
Question 2. What are the zones of healing epithelium?
Answer:
- White zone – outer epithelium
- Bluish zone – middle zone
- Red zone – inner epithelium covering the granulation tissue.
“Role of surgical instruments in practical exam scenarios: Questions answered”
Question 3. What are the ulcers that can occur over the leg?
Answer:
- Venous ulcer
- Varicose ulcer
- Post Thrombotic ulcer – inverted beer bottle deformity of leg due to oedema
- Marjolin’s ulcer
- Arterial ulcers:
- Hypertensive ischaemic ulcer
- Post. Arteriosclerotic
- Following a.v. fistula
- Ulcer associated with erythrocyanosis frigida
- Complicating blood diseases
- Sickle cell anaemia
- Acholuric jaundice
- Felty’s syndrome
- Artifact ulcer or factitious ulcer
- Self induced
- Neurotics
- Inaccessible place
- Unusual shape
- Appears pink and clean
- Gummatous ulcer
- Miscellaneous
- Foot Baller’s ulcer
- Meleney’s ulcer
- Of ulcerative colitis
- In rheumatoid arthritis
- Associated with Paget’s disease of bone
- Tropical ulcers
- Diabetic foot ulcer
- Yaws
- Diphtheritic sore.
“How does surgical knot-tying feature in practical exams? FAQ explained”
Question 4. What are the precursors of varicose ulceration?
Answer:
- Ankle flare
- Dermatitis
Question 5. What is ankle flare?
Answer:
- Fine veinules that course from medial malleolus and spreads out to be lost beneath the skin of the heel are known as ankle flare
- Seen at the level of ankle
- Due to the presence of direct communicating veins.
Question 6. What is the management proper?
Answer:
Conservative:
- Rest to the part
- Avoiding the local irritation
- Treat the cause
Tuberculous:
- Anti Tuberculous treatment
- Treatment of venous disorders
- D.V.T
- Varicote. V.
- Treatment of diabetes
- Separation of slough and regeneration of granulation tissue
- Hypochlovite sol
- 0.5% silver nitrate
- 1% zinc sulfate
- Topical antibiotic ointments
- Normal saline soaks
- Diabetic foot ulcer – control B-S levels.
Coverage of the ulcer:
- Amnion
- Silver foil
- Splint skin grafting
- Sofratulle etc.
Chronic and indolent ulcer:
- Infra red radiation
- Short wave therapy
- Ultraviolet therapy.
Trophic ulcer:
- Protective and soft padding
- If bone involvement – may require an amputation
Role of amputation:
- Penetrating ulcers
- Malignant ulcer not fit for local therapy
Excessive granulation – removed:
- Excision
- Curettage
- Application of copper sulfate crystals
Antibiotic after C/S:
Improve the nutrition:
- Protein supplementation
- Vitamin supplementation.
Hernia
Hernia History:
- Age – indirect inguinal hernia is usually seen in young individuals while direct in order individuals.
- Mode of onset – since birth, spontaneous, following heavy work.
- Most of the herniae are usually and straining.
- Where first appeared – if appeared in grain and extended into the scrotum inguinal hernia; if appeared below the groin crease and ascends above it – femoral hernia.
- Size and extent of the swelling when first seen – large enough to reach the bottom of scrotum in the beginning itself – congenital hernia; initially small to start with a gradually increasing – acquired hernia.
- H/o reducibility on lying down or on manipulation (indirect).
- H/o irreducibility in the part
- H/o pain initially dragging and arching type of pain, which increases as the day progresses due to stretch of the nerves.
- Pain ceases when hernia is fully formed H/o diffuse pain in abdomen (strangulation) due to drag on the mesentery or omentum.
- H/o features of the obstruction – (usually with irreducibility); Vomiting, distention, constipation, colicky pain.
- H/o Cr. Pulmonary pathology – Cr. Bronchitis, Br. Asthma, emphysema.
- H/o lower urinary tract obstruction – straining at micturition, phimosis, BPH, meatal stenosis.
- Treatment history-
- Application of any truss and belt.
- H/o lower abd. Surgery lower ureteric stone removal. appendicectomy, LSCS, lumbar sympathectomy,
- Family history – Genetic – protein and collagen diseases – prune belly syndrome.
- Past history-H/o similar complaints in the past (recurrent hernia).
“Early warning signs of gaps in understanding general surgery practical basics: Common questions”
Hernia General Examination:
- General built of the patient.
- Chest examination for evidence of COPD, asthma.
- Rectal examination for Cr. Constipation, enlarged prostate.
- Abdominal examination to extrude presence of intestinal obstruction.
Hernia Local Examination:
Hernia Position and Prequisites:
- Examine first in standing position for size, site, shape, surface, surrounding extent.
- Examine in supine position for reducibility and other tests as mentioned.
- Expose the clothes from the level of umbilicus to mid thigh level.
Hernia Inspection:
- Swelling
- Size and shape – Pyriform – indirect
- Spherical – direct, femoral.
- Position and extent – Ing. H – extends from above the inner part of the ing. Lig to scrotum. Fem. H extends from below the ing. Lig and ascends over it.
- Visible peristalis – seen in recurrent hernia.
- Skin over the swelling – Normal in uncomplicated hernia; reddened in strangulated H; discoloration and pigmentation in Cr. Trus operated sear in recurrent hernia.
- Impulse on coughing – ask the patient to cough and look at superficial inguinal ring for expansile cough impulse.
- Position of penis – important in case of a large inguinal hernia (may be displaced to opp. Side).
Hernia Palpation
- Position and extent
- An ing. H is positoned above the ing. Lig and med. To pubic tubercle wile femoral hernia vice versa.
- To get above the swelling – differentiates a serotal swelling from an inguino-serotal swelling.
- Hold the root of the serotum between the thumb in front and other fingers behind in an attempt to reach above the swelling.
In case of inguinal hernia – one cannot get above the swelling, while in scrotal swelling it is positive.
Hernia Consistency:
- Doughy and granular – omentum
- Elastic – Intestines
- Tenderness – incase of strangulated hernia.
- Relation of the swelling to spinal cord
- Impulse on coughing- always perform in standing position.
- Stand at the corresponding rites and employ corresponding hands for the rides to be examined.
- Ask the patient to hold the nose and blow or cough.
- Has to be performed only after the hernia is completely reduced.
An impulse is felt on one of the fingers placed.
- Index finger – direct
- Middle finger – indirect
- Ring finger femoral
Hernia Ring occlusion test:
- Occlusion of deep ring
- Surface mark the deep ring.
- Identify the anterior superior iliac spine – thee first bony prominence felt when traced from medial to lateral side along the inguinal ligament.
- Identify the pubic symphysis – midline.
- Mark the midpoint – mid inguinal point.
- 1⁄2 inch above this point of inguinal ligament, midpoint between anterior superior iliac spine and pubic tubercle.
- Deep ring-1/2 inch above and medial to mid point of inguinal ligament.
- Reduce the swelling.
- Block the ring with the thumb with above downward direction.
- Ask the patient to cough
- Swelling appeared
- Swelling didn’t appear.
“Asymptomatic vs symptomatic effects of ignoring practical exam principles: Q&A”
Hernia Equation:
- Ring blocked – swelling appeared = direct hernia
- Ring blocked – swelling didn’t appear indirect hernia.
Hernia Finger invagination test:
- Little finger is employed to invaginate the scrotum and enter the inguinal canal through external ring.
- Possible only in males and not in females.
Hernia Finger invagination test:
- Hold the root of the scrotum between the thumb and index finger and axe the patient to cough or blow out, contents of the hernia wide force out through superficial inguinal ring expansible cough impulse.
Hernia Reducibility:
- Either by self or has to reduced.
- Taxis – Patient in supine position flexion at thigh, adduct and internal rotation – relaxes the pillows of superficial inguinal ring and oblique muscles of the abdomen.
- Hold the fundus of the hernial sac; push the contents with one hand and direct with other hand must be performed very gently.
- In enterocele – first part is difficult to reduce but last part slips in easily and vice versa in omentocele.
Hernia Percussion:
- Resonant – enterocele, strangulated hernia
- Dull-omentocele.
Hernia Auscultation – Peristalsis.
Hernia Regional examination:
- Examine the testis, epididymis and spermatic cord.
- Examine the tone of abdominal muscles – loss of tone by
- Under protrusion of lower abdomen.
- Malignances bulging: if the patient is asked to get up against the resistance – muscle bulging appears over the anterior part of lower abdomen; represent the weakened segments of muscles
- Operation scars – eg: Mc. Burneys
- P.R. Examination – BPH and stenosis.
“Can targeted interventions improve outcomes using practical exam Q&As? FAQs provided”
Varicose Veins
Varicose Veins History:
- Age can affect any age but usually more middle-aged individuals.
- Occupation more common in jobs requiring prolonged standing, individuals involved in excessive muscular contraction, soldiers, doctors.
- H/o associated symptoms – tiredness and aching sensation in the limb, feeling of heaviness, cramps, localized pain in the course of the vein pain increases when the patient stands up for a long time and is relieved when he lies down.
- Bursting pain and right cramps indicate DVT.
- H/o swelling of ankle towards the end of the damp and itching.
- H/o any operation-like pelvic surgery (ovarian tumor, retroperitoneal tumor), surgery in the course of blood vessel.
- H/o pregnancy, long usage of OC – DVT.
- H/o any visural malignancies – DVT.
- H/o any vascular malformations- superficial thrombophlebitis; bleeding, ulceration, local gigantism, deformity (cong. A-V fistulae).
Varicose Veins General Examination:
- Built
- General diseases
- Infections
- PAD
- Abd. Tumors
- Pallor
- Evidence of any portal HTN.
Varicose Veins Local Examination:
Varicose Veins Inspection:
Both front and back of lower limb from umbilicus to toes is inspected for:
- Anatomical distribution of varicose veins.
- Colour and shape of the limb.
- Flare sign (Blow out of perforating veins at malleolus due to high pressure reflux).
- Skin conditions like eczema, pigmentation, ulceration etc.
- Skin infections like tinea interdigitialis.
- Joint movements.
- Presence of flat foot.
- Presence of faulty muscle development.
Palpation: For
- Course of varicose veins.
- Blowouts and perforators (which feel like button hole gap in deep fascia).
- Arterial pulsations.
- Features of ulcer, carcinoma etc.
Varicose Veins Clinical tests:
Varicose Veins These are done to find out:
- The competence of valves in
- Long saphenous vein.
- Short saphenous vein.
- The competence of communicating veins.
- Patency of deep venous system.
“Differential applications of open vs laparoscopic techniques in practical exams: Questions answered”
Varicose Veins Cough impulse test:
- This tests competence of valves in long saphenous vein I (A). The valve at sapheno femoral junction is incompetent if a fluid thrill is felt on the fingers below saphenous opening when patient coughs.
- Percussion sign: This is for 1 (A). With patient erect percussion of main bunch of varicose veins imparts a thrill to the palpating fingers at the saphenous opening.
Varicose Veins Differential tourniquet test:
- This is to differentiate between long and short saphenous incompetence when there is a bunch of varicose veins in calf.
- Elevate the limb to drain the blood, tie two tourniquets – one at groin, other below and ask patient to stand up. Press short saphenous opening at popliteal fossa and release tourniquets.
- If varicosities fill up with pressure continued – Long saphenous veins.
- If varicosities fill up only on release of pressure – short saphenous system.
Varicose Veins Elastic bandage test:
This is done to find out patency of deep veins. Tie an elastic bandage from toe to knee and patient walks for 10 minutes. If there is severe bursting pain – deep venous system is severely impaired (Perthes test).
Varicose Veins Treatment:
- Conservative treatment:
- Elastic support.
- Exercises.
- Postural drainage.
- Self massage.
Varicose Veins Prophylaxis:
- Subcutaneous low dose heparin 5000 units 2 hours before and 24 hours after
- Dextran – 70 inhibits sludging of RBC and platelets
- Aspirin along with dipyramidole.
Varicose Veins Inspection:
- Swelling may be localized as in case of vv’s affecting a segment of superficial vein, superficial thrombophlebitis; generalized swelling is due to DVT.
Varicose Veins Skin:
- Colour – local redness – due to superficial thrombophlebitis.
- Generalized white leg (Phlegmasia ulba /donens) – swollen limb from excessive edema or lymphatic obstruction.
- Phlegmasia circular dolens – limb becomes congested and deep blue due to severe venous obstruction.
Varicose Veins Regional examination:
- Examination of abdomen.
- P.V. and P.R examination – for any pelvic tumor.
- Examination of peripheral pulsation.
Varicose Veins Tests:
- Modified perthes test – To know whether the deep veins are normal or not.
- Schwartz test.
“Steps to master general surgery practical exams: Study plans vs mock tests: Q&A guide”
Question 7. What are the sites of varicosities?
Answer:
- Lower limb v.
- Pampniform plexus of v. Vulval v.
- Lower end of oesophagus.
- Sites of porto systemic anastomosis.
- Around umbilicus – caput medusae.
- Retro peritoneum.
- Bare area of liver.
- Lower end of ano rectum -haemorrhoids.
Question 8. What are the secondary varicose, veins?
Answer:
They are secondary to a cause:
1. Ext. pressure.
- Tumor
- Pregnancy
- In renal, malignancy……… left sided varicocele.
2. Increased venous pressure……………..Porto systemic anastomatic sites.
- Oesophageal varices.
- Caput medusae.
- Haemorrhoids.
3. Due to surgery on veins.
- Pelvic surgery
- Ligation.
4. Due to internal blockade.
- Thrombosis D.V.T.
5. Due to increase in the inflow of blood.
- A.V. fistula.
Question 9. Why varicosities are common in lower limb?
Answer:
- Because of erect posture.
- General Surgery
- Long columns of blood has to be supported and can lead to weakness and incompetency of valves and loss of surrounding connective tissue.
Question 10. What are the components of venous systems of lower limb?
Answer:
It comprise of
- Deep systems
- Muscular veins.
- Venae committacne.
- Superficial system with its tributaries – long saphenous short saphenous.
- Communicating systems between deep and superficial systems.
“Role of diagrams in understanding surgical procedures for practical exams: Questions answered”
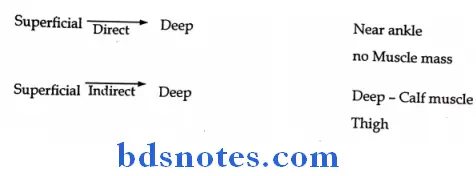
Question 11. What are the types of communicating veins or perforating veins?
Answer:
There are two types:
- Direct
- Indirect
Question 12. What are the factors responsible for venous rectum?
Answer:
- Negative pressure in thorax.
- Peripheral pump – calf muscle.
- Visa – tergo of adjoining arterial pulsation.
- Non-refluxing valves in the course of a vein.
Question 13. How will you manage the case?
Answer:
Management consists of
- Establishing the nature of varicosities by doing clinical exam and tests.
- Incompetency of S.F.valves.
- Incompetency of perforators.
- Secondary varicosities due to D.V.T.
- Increased input like A.V. fistula.
Management proper.
Question 14. What investigations are helpful in diagnosis?
Answer:
Investigations
- Noninvasive
- Doppler study for venous flow patterns.
- Invasive
- Ascending
- Descending venograms.
“How do case studies enhance comprehension of practical exam scenarios? FAQ explained”
Question 15. What are the modalities of treatment available?
Answer:
The modalities of treatment that are available are:
- Conservative – Bed rest and elevation.
- Sclero therapy
- Surgical.
Complications of varicose veins:
- Eczema and dumatitis
- Thrombophlebitis
- Haemorrhage
- Varicose ulcer
- Calcification in walls of veins.
Question 16. What are the conservative methods of management?
Answer:
Conservative management is indicated:
- During pregnancy.
- When other modalities of treatment are contra indicative.
Support is given by graduated compression by elastic stockings.
Question 17. What is sclerotherapy?
Answer:
- Sclerotherapy is a method of management in whichr the lumen of the vein is obliterated by injecting chemicals or scleosants.
Question 18. What are the methods of sclerotherapy?
Answer:
Two types
- Intra variceal
- Lower limb
- Oesophagus
- Gastric
- Peri variceal
- Haemorrhods
Question 19. What are the agents used?
Answer:
- Ethoxy sclerol.
- Ethanalamine – 5% Ethanalamien oleate.
- Sodium tetra decyl sulphate 3%.
“Early warning signs of poor performance in general surgery practical exams: Common questions”
Question 20. What is the mechanism of action?
Answer:
- It produces aseptic inflammation leading to thrombosis.
- Causes approximation of intima to intima leading to obliteration injection.
- Causes perivenous fibrosis leading to block – perivenous injection.
Question 21. What are the indications for sclerotherapy?
Answer:
- Short segment of venous dilatation.
- Leg V. Varicosities – Cosmetic.
- Small multiple telangectic veins.
- Following ligation of veins for short segments.
Question 22. What is the method of sclerotherapy?
Answer:
- Make the veins prominent.
- Take sclerosant and put the needle into the vein.
- Patient is asked to lie down – venous collapse – and then injected.
- intraluminal
- Pressure bandage at the end of the procedure and stockings for six weeks from the lat injection.
- Dosage is 1 ml at any one point.
Question 23. What are the side effects of sclerotherapy?
Answer:
- Can cause deep V. thrombosis.
- Skin tanning.
Question 24. What are the advantages of sclerotherapy?
Answer:
- Cosmetically good result.
- Ideally suited for
- Small segments of leg veins.
- Telangiectatic veins.
Question 25. What are the contraindications of sclerotherapy?
Answer:
- Presence of acute inf. Thrombophlebitis.
- Deep vein thrombosis.
- Pregnancy, Pelvic tumour,
- Pill Pregnancy, pelvic tumour, pill.
Question 26. What is the surgical treatment for S.F. incompetency?
Answer:
The treatment is flush ligation of the S.F junction followed by either.
- Phlebectomy.
- Stripping of the V.
Question 27. What is Flush ligation?
Answer:
- Flush ligation means ligating the saphenous. V. right at the junction with the femoral. V without leaving any tributary.
- If it is ligated distal to any tributary, as this tributary will become varicose because f the leak if left behind unligated.
“Asymptomatic vs symptomatic effects of outdated study methods: Answered”
Question 28. What is phlebectomy?
Answer:
- If the dilated segment is a short one with multiple small incisions, the dilated. V is removed and is called as phlebectomy.
Question 29. What is stripping?
Answer:
- Here the entire dilated and tortuous long saphenous. V is stripped and removed after flush ligation.
- After flush ligation – A Meyer’s stripper is passed from bellow after making an incision over the ankle through long. Saph, V.
- The acorn shaped head is firmly tightened to the venous wall.
- With interrupted jerky movements from below the vein is stripped off and a compressive bandage applied from above.
- Stripping avoided in the lower 1/3 of the leg to prevent injury to saphenous nerve. Done upto the level of middle 1/3 or upper 1/3.
Question 30. Is stripping always indicated?
Answer:
- No. if the long saphenous vein appears normal, stripping is to be avoided. In future it may be required for CABG.
Question 31. What is the stripper now used?
Answer:
- Oesch Pin stripper.
- Oesch hook.
Question 32. What is the approach for perforating incompetency?
Answer:
- Perforators are marked.
- Local exposure and subfascial ligation of cockett and Dodd or Linton’s operation.
- Localized segment of dilated vein.
- Phlebectomy.
- Sclerotherapy.
- Endoscopic ligation of perforators beneath the deep fascia.
Question 33. How will you manage variceal bleeding?
Answer:
- Ruptured veins bleed profusely.
- Managed by elevation of the limb followed by firm pad and bandage and subsequently.
- Sclerotherapy.
- Ligation + excision.
- Intravariceal injection of sclersants – Oesophageal. Varices
- Banding
- Oesophgeal. Varices
- Piles.
“Can advanced tools supplement practical exam preparation? FAQs provided”
Question 34. Why that site is common for venous ulcer?
Answer:
- Because of the presence of direct perforating. V, which transmits the pressure changes directly to sup. System.
Question 35. What are the features of a venous ulcer?
Answer:
- Classical site.
- Well circumscribed.
- Punched out and sharp edges.
- Floor usually formed by deep. Fascia and may extend upto periosteum.
Question 36. What is the conservative method of management is called?
Answer:
- It is called as Bisgaard’s method
- It comprises of
- Elevation of the limb.
- Crepe bandaging-compressive bandaging.
- Exercise
- Active movement of calf. M.
- Lifting of the heel for-spring action.
- Teaching correct walking.
- Elevation of root end of bed.
- Bandaging and elevation.
Mc. collum approach
- Wool
- Elastic compression bandage
Coband dressing.
“Differential applications of traditional vs digital study resources: Q&A”
General Surgery Practicals Short Cases
Surface Swelling:
Surface Swelling History:
- Duration – short duration with pain – inflammatory, traumatic, malignant.
- Long duration with slight pain – neoplastic, chronic inflammatory swellings.
- Since birth congenital swellings – eg: cystic hygroma, meningocele, hemangioma, branchial cyst, Dermoid cyst, thyroglossal cyst.
- Mode of onset spontaneous, posttraumatic, in any pre existing lesion like keloid, pigmented mole – melanoma.
- Associated symptoms – depends on location, size etc., pain, dysphagia, disfigurement, difficulty in movement.
- Pain most prominent feature of a swelling ask for nature, site, aggravating or relieving factors, disturbance to sleep, time of onset.
- Mostly pain precedes in inflammatory swelling but in tumors swelling appears long before the patient complains of pain.
- If swelling first and pain later – indicates pressure effects, deep infiltration, associated inflammation, complications like hemorrhage, ulceration, fungation etc.
- Progress of the swelling
- Gradually growing – simple neoplastic swelling.
- Gradual to stand with, but recent history of rapidity – indicates complications
- like hemorrhage, malignant transformation.
- Rapidly growing-malignant neoplasia.
- Regression post inflammatory, post treatment.
- Presence of other lumps – sebaceous cysts, neurofibrometosis, diaphyreal actasis, Hodgkin’s disease show multiple glandular swellings.
- H/o secondary/local change – softening, ulceration fungation, inflammatory changes, discharge of purulent material, sulphur granules, bone spicules.
- Recurrence of the swelling malignant swelling pagets recurrent swelling, incompletely excised cystic swelling.
- H/o associated symptoms.
- Treatment history – medical, surgical; only H/o application of counter irritants, which may result in local ulceration, inflammation.
- Past history H/o trauma, radiation, tuberculosis, syphilis, endemicity of any particular disease.
- Personal history – habituation (eg: chutta cancer, khaini cancer), appetite, sleep etc.
- Family history – H/o Tb, Von reckling hausens disease, malignant tumors.
Surface Swelling General Examination:
Apart from the routine general examination note for
- Built of the patient.
- Pallor.
- Attitude.
- Any other swellings elsewhere in the body.
- Recording of vitals.
Surface Swelling Local Examination:
Local Examination Inspection:
- Size
- Shape round, oval, irregular, piriform
- Surface smooth, uneven, nodular, and lobulated
- Skin – normal, features of inflammations any pigmentation (hyper or hypo)
- Other swellings
- Surroundings features of inflammation, prominence f veins, wasting, edema.
- Extent of the swelling – always describe in relation to bony points in tow planes.
- Colour
- Any pulsations – aneurysms, vascular growths like carotid body tumor.
Peristalsis – eg: cong. Pylori stenosis. - Edge – well defined (Bening and chronic inflammatory swellings); ill defined (malignant and acute inflammatory swellings).
- Movement with respiration – swellings arising from upper abdominal viscera; also hepatic and splenic colon flexures.
- Impulse on coughing – swellings, which are in continuity with abdominal, pleural and cranial cavity.
- Movement on deglutition – thyroid gland.
- Movement with protrusion of tongue-T-cyst.
- Any pressure effect:
- Scars
Surface Swelling Palpation:
Confirm the findings of inspection, but follow the systematic order
- Temp – due to increased vascularity like in infection or vascularised tumor-sarcoma.
- Tenderness – Be gentle in approach; see for facial expression.
- Surface:
- Smooth – cyst
- Nodular – lymph nodes
- Lobular – lipoma
- Irregular/rough – carcinoma
- Edge/margin
- Neoplastic/Cr. Inf – well defined
- Be. Infill defined
- Malignant – irregular.
- Consistency
- Cystic – cyst, abscess
- Soft – lipoma
- Firm – fibroma
- Hard-choadroma
- Bony hard – osteoma
- Stony hard – carcinoma.
- Fluctuation
- Fix the swelling
- Perform in two planes
- Keep the examining fingers for apart
- Pagets test:
- Performed in only small swellings; place a finger on the centre of the swelling and see for fluctuation.
- Slip sign – solid swelling slips to the examining finger while cystic one yields.
- Slip sign – lipoma +ve.
Surface Swelling Tumors And Cysts:
Surface Swelling Some important definitions:
- Lump is a vague mass of the body tissue.
- Swelling is a vague term, which denotes any enlargement or protuberance in the body.
- Tumor is an abnormal mass of tissue, whose growth is excessive and uncoordinated with that of the rest of the body and is progressive.
- Wound – is a loss of continuity in skin or mucous membrane caused by violence with varying involvement of surrounding or deeper tissues.
Surface Swelling Lipoma:
Lipoma is a benign connective tissue tumor arising from adipose tissue.
- Anatomical (according to the site)
- Subcutaneous
- Subserous
- Subsynovial (knee)
- Submucous
- Subperitoneal
- Intermuscular
- Subperisteal.
Surface Swelling Clinical:
- True Lipoma.
- It is a simple tumour (encapsulated).
- Pseudo-lipoma.
- Diffuse lipomatosis- fatty infiltration of subcutaneous tissue, eg: abdominal wall, neck and chin.
- Character – adherent to skin, diffuse margin and always symmetrical.
“Difference between general surgery practical exams and theory exams: Q&A explained”
Surface Swelling Cause:
- Lack of exercise.
- Excess calorie intake.
- Hormonal.
- Multiple painful Lipoma or neurolipoma (Adiposa Dolorosa or Dercum’s disease).
- Naevo-lipoma (Lipoma mixed with haemangiomatous tissue).
Surface Swelling Diagnosis:
- Alteration of skin colour (Slight bluish hue).
- Slightly compressible.
- Soft or lobulated at places.
- Fibro-lipoma
- (Contains excessive amount of fibrous tissue). Diagnosis – Firm with
knotty feel at places.
Surface Swelling Diagnosis:
- Oval or rounded.
- Pedunculated or sessile.
- Margin – well defined but margin slips under the examining finger-slip sign +ve.
- Surface lobulated.
- Consistency – soft but often with pseudo-fluctuation.
- Overlying skin – may show dimpling.
- Free from deeper structures, fingers can be insinuated under the growth.
- Lipoma is differentiated from the normal fat by its lobulated character.
- The fibrous septi divide the fat cells and these are attached to the capsule.
Surface Swelling Treatment:
- Excision is the treatment of choice.
- Incision is the made straight over the tumour (following Langer’s line) but if there is a big lipoma (when overlying skin has to be excised), an elliptical incision may be required.
- May occur any where in the body (universal tumor) but most common sites are napes of neck, shoulder, back, gluteal region, retroperitoneum.
- Is the commonest subcutaneous swelling.
- Is a painless, slow growing, soft and lobulated swelling.
- It doe not occur in the palm, sole or in scalp because the fat is contained within the dense fibrous septae in these areas.
- A pedunculated subcutaneous lipoma is called lipoma arboresum.
Surface Swelling Diagnosis:
- Has free mobility; not getting restricted on stretching of deep fascia and contraction of muscle.
- Show dimpling when the swelling is pushed away (due to fibrous strands which transverses the lipoma and is attached to the overlaying skin).
- Transillumination – negative.
- Skin is pinchable (eg: Sebaceous cyst).
Surface Swelling Complications:
- Necrosis due to repeated trauma – the lump becomes hard and painful.
Myxomatous degeneration. - Hemorrhage.
- Common sites where lipoma undergoes malignancy retroperitoneal lipoma, lipoma in the high, subcutaneous lipoma of shoulder region.
Infection.
Surface Swelling Clinically:
- May be painless, painful when present in a narrow space, may produce pressure symptoms if large and may be a site of intussception of a small bowel loop.
Surface Swelling Differential diagnosis (ABCDS):
- Any cystic tumor.
- Baker’s cyst.
- Cold abscess.
- Dermoid cyst.
- Sebaceous cyst.
“Most common complications of poorly understood practical exam concepts: FAQs”
Surface Swelling Dermoid Cyst:
- A Dermoid cyst is a cyst lined by skin (squamous epithelium) and lies deep to the skin.
- They are considered to be occlusion cysts, taking their origin from an embryonic process.
- The contents are thick containing a mixture of sweat, sebum and desquamated epithelial cells and hair.
Surface Swelling Types:
- Congenital or Sequestration Dermoid – It is due to inclusion of ectodermal layer into the deeper tissues during the process of closure of embryonic clefts and sinuses by skin fusion.
- Acquired or Implantation Dermoid – Introduction of epithelial cells into the deeper tissues by mechanical trauma e.g., pin prick, needle puncture or during shaving. So they may not be in the midline, e.g. submandibular region, finger tips, deltoid region – after injection, etc.
- Tubulodermoi – They occur in the track of the ectodermal tubes, which are precursors of various tubular structures e.g., thyroglossal cyst, postanal Dermoid, etc.
- Teratomatous Dermoid (e.g., ovarian Dermoid or Testicular Dermoid) – Here all three embryonic layers may be found.
Surface Swelling Features:
- Site- line of fusion,
Surface Swelling Example:
- Midline.
- Pterion.
- Asterion.
- Face – Junction of outer and inner canthus.
- Postauricular.
- Number – single.
- Size variable.
- Shape – globular.
- Surface – smooth.
- Skin free – but adherent to underlying structures.
- Transillumination – negative.
- Guttering of base of bone may be present.
- Slightly turbed fluid on aspiration.
- It is a sub facial swelling but can also be a subcutaneous swelling.
- Skin is pinchable.
- Mobility is not as free as subcutaneous swelling.
- Sites of teratomatous dermoids – ovary, testis retroperitoneum, superior mediastinum, pre sacral area.
- Dermoids over scalp. Cause indentation over scalp, may have intracranial extension and have to be differentiated from sub epicranial lipoma.
- Cystic swelling – fluctuation positive.
- Not compressible.
“Why are practical exam mechanisms often misunderstood in practice? Questions answered”
Question 1. What are lingual dermoids?
Answer:
- Fluctuant swellings.
- Midline of tongue.
- Lined by –
- Squamous stratified epithelium with or without dermal appendages.
- Ciliated, mucous secreting epithelium with mucin.
- Filled with doughy mass of keratin.
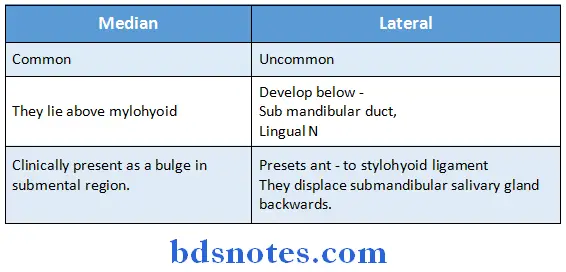
Question 2. What are sublingual dermoids?
Answer:
- They are a type of sequestration dermoid a causing due to sequestration of surface ectoderm at site of fusion of two mandibular arches.
They are two types:
Question 3. How will you confirm your diagnosis?
Answer:
- Clinically.
- Radiologically.
- X-ray skull – boney indentation.
- U.S. scans.
- Retroperitoneal, abdominal teratomatous dermoids.
- CT scan of brain – extension, intracranial.
Question 4. What are the complications?
Answer:
- Infection- Abscess formation.
- Intracranial extension.
- Malignant transformation – teratomatous.
- Calcification
Question 5. How will you manage?
Answer:
Intraoral approach in surgery
Management is by surgery
- Indication:
- Cosmetics.
- Pain and infection.
- Lump abdomen.
For sequestration dermoid.
- Radiological exclusion of intracranial extension:
- Local anesthesia.
- Xylocaine with adrenaline infiltration.
- Excision
- Skin, various layers of scalp, cyst, is excised from pericranium and excised in to toto.
- Suturing in layers.
- External angular dermoid.
- Swelling deep to muscle.
- Muscle divided and cyst excised and muscles sutured.
- Tubulo embryonic
- Excision of the cyst along with the track;.
- Sistrunk’s operation for Thyroglossal cyst.
- Implantation dermoid
- Local bock.
- Incision.
- Dissection and removed.
- Teratomatous
- Excision biopsy/follow up for malignancy.
“Cost of ignoring practical exam principles vs benefits of systematic approaches: Q&A”
Sebaceous cyst (Epidermoid cyst):
- It is a cutaneous swelling.
- It is a retention cyst due to accumulation of sebum resulting from obstruction to the duct of sebaceous glands.
- Also called epidermoid cyst (lined by squamous epithelium and situated in dermis).
- Microscopically consist of sebum, fat desquamated epithelial cells and rarely an organism called Demodex folliculorum.
- Multiple sebaceous cysts are called as wens (present on serotum).
Features:
- Site – Anywhere except palm or sole.
- Number – May be multiple, especially when it occurs in scrotum.
Size variable. - Shape rounded.
- Surface smooth.
- Presence of a bluish spot called puncta.
- Fixity to deep structures – nil, except at the puncta, even if later is absent.
- Transillumination – negative.
- Guttering of base of bone – absent.
- Aspiration – cheesy thick pultaceous material.
Complications:
- Infection and suppuration – common.
- Sebaceous horn – black horn like material due to drying up of inspissated sebaceous material coming out of the cyst.
- Calcification of wall.
- May produce ‘Cock’s peculiar tumor’. It is a sprouting chronic infected granulation tissue coming out through the mouth producing foul discharge.
- It is so called as it resembles an epithelioma. (Pott’s puffy tumour – It is an encysted oedema of scalp overlying an extradural abscess).
- Sebaceous adenoma.
- Malignancy.
- Rarely basal cell carcinoma.
Treatment:
- Excision is done after making an incision over the prominent part of the cyst.
- If the cyst is big overlying skin is excised.
- The punetum is adherent to the cyst on squeezing the cyst putty like or cheesy sebaceous material with an unpleasant smell may conc. out through it.
- Skin cannot be pinched (eg: Lipoma, Dermoid cyst).
- Not compressible.
- Because of its putty like consistency, the swelling can often be indented by a finger tip (sign of moulding) and sign of indentation.
- Consistency – cystic or tense cystic, hence fluctuation may be positive.
- Non-infected cyst.
- Local anaesthesia.
- Elliptical incision centering the punctum.
- Dissect it laterally by firm traction over the skin portion of the punctum and removed in toto.
- Infected cyst
- Dissection removal not possible due to firm adherance.
- Cruciate incision and excision and avulsion of the lining.
- Analgesics.
- Antibiotics.
- Multiple sebaceous cysts.
- Over the scrotum.
- Patches of skin along with the cysts excised and skin sutured.
“Success rate of interventions using modern practical exam techniques: FAQ”
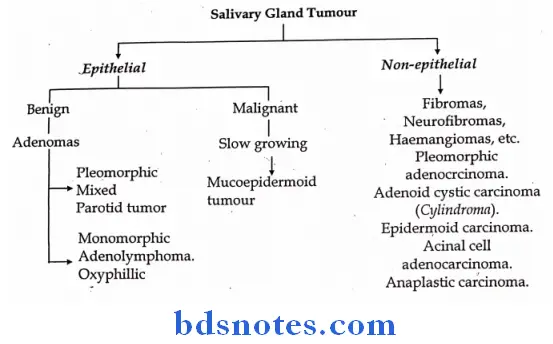
Parotid Swelling:
Parotid Swelling History:
- Swelling – ask for site, mode of onset and duration of onset.
- Acute parotitis – dehydration, poor oral hygiene, infectious disease (Typhoid), post op periods, secondary to obstruction of duct or stricture, mercury or iodine poisoning.
- Presents with sudden increase in both glands with fever, pain.
- Parotid abscess – presents with brawny edematous swelling with severe pain and high fever.
- Pleomorphic adenoma a very slow growing, tumor, initially painless and later becomes painful; may be unilateral or bilateral; may show malignant transformation.
- Adenolymphoma – presents similar to Pleomorphic adenoma, but arises in the lower part of parotid gland.
- Associated features
- Pain – Ac. Parotitis – Bilateral pain
- Parotid abscess – severe throbbing pain, with redness.
- Parotid duct obstruction – colicky pain during meals with increase of size of the gland.
- Fever
- Excessive salivation
- Pain referred to ear
- Any discharge.
- Features of facial nerve involvement.
Parotid Swelling General Examination:
Parotid Swelling Local Examination:
Parotid Swelling Swelling:
- Site- around the ear
- Lower part
- Middle part
- Size
- Shape
- Surface
- Smooth
- Irregular
- Skin – Normal
- Evidence of fixity
- Extent
- May extend on to the neck.
- Raised lobule of the ear.
Parotid Swelling Consistency:
- Soft
- Firm
- Hard
Parotid Swelling Mobility:
- Without masseter contraction
- With masseter contraction.
- Mobile.
- On contraction of masseter.
- No change
- Reduced mobility or fixity.
- Fixed from beginning.
Examination for Facial nerve involvement.
- Naso labial fold.
- Angle of mouth.
- Loss of wrinkling of forehead.
- Inability to close the eye.
- Inability to whistle.
Any other cranial nerve involvement.
“Is general surgery practical exam-related risk reversible if addressed promptly? Answer provided”
Parotid Swellingc Regional examination:
- Examination of oral cavity.
- Deep lobe enlargement – towards tonsil.
- Parotid duct opposite 2 upper molar teeth – any discharge.
- Examination of neck for any glands.
- Distant metastasis – pulmonary secondaries.
Parotid Swelling Clinical Features:
- Age 30-40 years.
- Painless swelling just behind and below the angle of the mandible – slow growing.
- Swelling is firm, lobulated and well defined and mobile even after contraction of the masseter. However, gland is placed deeply in relation to sternomastoid.
- Facial nerve is not involved in a benign tumour.
- Cervical lymph nodes must be examined as a routine.
Parotid Swelling Signs Of Malignancy:
- Tumour which was relatively slow growing starts progressing rapidly.
- Lump becomes relatively fixed and patient starts complaining of pain.
- Fixity to surrounding structures like skin superficially and towards deep to masseter and mandible (later).
- Consistency changes to hard from firm.
- Appearance of facial palsy.
- Involvement of cervical lymph nodes.
- Incase of suspicion of malignancy incision biopsy was practiced previously. But frozen or cryostat section makes it now possible for a competent pathologist to give opinion regarding its nature.
- Preoperative needle biopsy has the advantage of simplicity but eh disadvantage of tumour implants along the track of unpopularity.
- Now-a-days pertechnate scanning is very helpful where tumour shows as “Cold spot”.
“Treatment scope in adults vs children for practical exam evaluations: FAQs”
Parotid Swelling Treatment:
Parotid Swelling Paty’s operation:
- Incision is given in front of tragus of pinna vertically descends downwards curves around ear lobule up to mastoid process and descends down to neck.
Parotid Swelling Curative:
- Extracapsular excision can be tried in a smaller tumour but recurrence rate is high, because even in small growths there is always a chance of seedling growths. Inadequate excision often precipitates malignancy.
- So superficial parotidectomy is now the treatment of choice.
- The dissection is carried out superficial to facial nerve lying between superficial and deep parts of the gland.
- Total parotidectomy (removal of both lobes) is indicated in case of carcinoma with or without block dissection of cervical glands on the side of the tumour depending on the presence of operable lymphatic metastasis following successful treatment of the primary.
- Total parotidectomy is also advocated in any recurrence after superficial parotidectomy.
- Here facial nerve often cannot be saved as otherwise excision may be incomplete and in carcinoma one has to perform as total a removal as possible.
Parotid Swelling Palliative treatment:
- Radiotherapy for palliation has reasonably good outcome. If there is postoperative recurrence or the margin of excision is not complete radiotherapy with Cobalt helps considerably.
- Chemotherapy – Methotrexate and flurouracil have been tried but results are not encouraging.
- Complications after Parotidectomy
- Auriculotemoral (Frey’s) syndrome This follows injury to the auriculotemoral nerve with its subsequent regeneration and patient complains of
- Cutaneous hyperaesthesia above and in front of ear especially after shaving.
- Flushing, sweating and pain over parotid area during meal.
- Intractable cases are treated by avulsion of auriculotemporal nerve.
- Facial nerve paralysis – If the injury to the nerve has followed parotidectomy for benign conditions, suturing or nerve grafting can be tried.
- For malignant conditions, where nerve has to be sacrificed transfer of masseter to the paralysed corner of the mouth or fascial sling to prevent distortion of fascial contour can be tried.
- Sometimes modified tarsorrhaphy is required to prevent exposure keratitis.
“Steps to incorporate AI into analyzing general surgery practical exam cases: Questions and answers”
Question 6. What is deep parotid tumour?
Answer:
- Tumour arising from deep lobe.
- Seen through oral cavity.
- Pushes the tonsil and fauces medially.
- Bi manually palpable.
Question 7. What is the relationship of facial nerve to parotid?
Answer:
- It is intimately related.
- After it comes out of stylomastoid foramen it enters the gland t the upper part of post medical surface.
Question 8. What are the branches of facial nerve?
Answer:
It divides into
- Tempero facial.
- Temporal.
- Zygomatic.
- Cervical facial
- Buccal
- Mandibular
- Cervical.
Question 9. What are the effects of fascial nerve injury or involvement?
Answer:
- Loss of wrinkling of forehead.
- Inability to close the eyes.
- Tears from one eye.
- Deviation of angle of mouth.
- Inability to whistle.
- Pulling of the lower lip.
“Role of digital tools in improving precision with practical exam tracking: FAQs explained”
Question 10. What investigations you would like to do?
Answer:
Locally
- Radiology of the part.
- U.S. exam.
- Solid
- Cystic
- Extent
- C.T. scan
- Deep lobe tumour
- For metastasis
- Sialogram
- To study the duct
- Isotope scan – Tchin 99
- Cold spot – majority
- Hot spot – adeno lymphoma.
Question 11. What is the role of biopsy?
Answer:
- Biopsy is usually not indicated.
- Primary surgical therapy and subsequent examination is the policy.
Question 12. What is the danger of biopsy?
Answer:
- Incision biopsy – Danger of recurrence.
- F.N.A.C
- Danger of capsular injury and tumour implantation.
- Recurrence.
- Being practiced in special centers.
- Excision biopsy – amounts to primary surgical procedure.
Question 13. What is the definite line management?
Answer:
- Doing a superficial or super facial parotodectomy.
Question 14. What are the landmarks for sup. Parotidectomy?
Answer:
- Retro mandibular venous plexus.
- Branches of facial nerve.
Question 15. What is Patey’s facio venous plane?
Answer:
- It is the plane between sup. and deep lobe.
- Formed by – Retro mandibular V. and facial nerve.
Question 16. What is deep parotidectomy?
Answer:
- When the tumour is from deep lobe.
- Sup. Lobe is retracted and the deep lobe tumour delivered through the branches of facial nerve and removed.
Question 17. What is conservative total parotidectomy?
Answer:
- When total parotidectomy is performed along with preserving the facial nerve it is called as conservative parotidectomy.
Question 18. What is Mickulitz’s disease?
Answer:
- It is an asymptomatic enlargement of all salivary glands along with lacrimal glands.
Question 19. What is Sjogren’s syndrome?
answer:
- All the features like above with
- Kerato conjunctivitis sicca
- Dry mouth
- Rh. Arthritis
- Associated connective T. disease
- Lupus
- Scleroderma
- Raynaud’s phenomenon.
- Tests for Sjogren’s syndrome
- Rose Bengal dye test.
Question 20. Why it is called parotid?
Answer:
Para = near, around, otic ear (Greek).
Question 21. What are the contents of parotid compartment?
Answer:
- Nerve compartment – superficial
- Great auricular nerve.
- Auriculo temporal.
- Facial nerve.
- Venous-middle – Post. Facial vein, temporal vein.
- Arterial compartment – deep
- External carotid artery.
- Internal maxillary.
- Sup. Temporal artery.
“How do advancements in technology enhance practical exam research? Q&A guide”
Question 22. What is the lymphatic drainage of parotid?
Answer:
- Two sets of lymph nodes.
- Superficial-under the fascia.
- Deep – with in the gland.
- Drains into upper deep cervical – horizontal group.
Question 23. What is the nerve supply?
Answer:
- Secretomotor – otic ganglion – auriculo temporal.
- Sympathetic sup. Cervical ganglion.
- Sensory-auriculo temporal.
Question 24. What is accessory parotid?
Answer:
- It is the prolongation of the gland immediately above the duct is known as accessory or social parotids.
Malignant Melanoma
- It is a malignant tumor of the melanocytes (mainly found in epidermis and dermis), which originate from the neural crest and so ectodermal in origin.
- Nature of progress – recent rapidity of growth, increase in mole, increase in pigmentation.
- Role of hormones – Estrogens and steroids.
- H/o exposure to increased periods of sunlight.
- H/o secondary changes – like ulceration, bleeding, itching.
- Family history – Familial clustering of melanoma
- Personal history – loss of weight and appetite.
Malignant melanoma:
- Malignant melanomas represent 3% of all malignant skin tumours.
- Sex incidence – Males and females are equally affected.
- Maximal incidence 40-60 years. Incidence of malignancy is very rare before puberty.
- Injury appears to play a definite role in the aetiology but role of hormone is not ruled out.
- Rare in dark skinned individual.
- Lower half of the body is more commonly affected than the upper half.
50% occur from preexisting moles, ↑ incidence in immunosuppressed patients.
Malignant melanoma General Examination
- Pallor.
- Icterus.
- Hepatomegaly.
- Ascites.
- Satellite nodules.
- Lymphadenopathy.
- Evidence of albinism, xeroderma pigmentosa.
- Presence of any other pigmented moles.
- Melanoma containing cells are mainly found in the epidermis – (dentritic cells in basal layers) and dermis (spindle shaped cells around the blood vessels) – hence skin is the commonest site of affection.
“Early warning signs of outdated methods in practical exam studies: Common questions”
Malignant melanoma Features:
- Site
- Lower lip, nail fold and nail bed of big toe or other toes.
- Lateral side of sole.
- May occur in the anterior abdominal wall, forehead, etc.
- Rarely, in Eye, Leptomeninges, etc.
- Usually there is history of trauma after which growth starts.
- Rapidly progressing.
- Size variable.
- Sessile or ulcerative growth (Dark brown incolour) with a pigmented halo around.
- Bleeds profusely.
- Friable when sessile.
- Lymph gland – involved.
- Sometimes subcutaneous blackish satellite nodules are seen along lymphatics.
Malignant melanoma Sites of melanoma:
- Cutaneous of ocular commonly (90%) (Ocular sites – conjunctival or uveal or choroidal).
- Mucosal or Leptomeningeal rarely. (Nasal antrum, Mouth, Oesophagus, Rectum and anal canal, bronchus, genitalis, etc.) are mucosal sites.
Malignant melanoma Classification:
- Benign.
- Malignant.
Malignant melanoma Danger signs of malignancy:
Recent increase in size of an existing or recent appearance of a mole.
- Alteration in colour – increase in pigmentation or loss pigmentation (depigmentation) of an existing mole.
- Itching, weeping, crusting, scabbing, bleeding and ulceration.
- Loss of hair over a hairly mole.
- Induration at the base.
- Irritation or pain.
- Satellite lesions around existing mole (due to local intra dermal lymphatic spread).
- Halo formation – however this may also occur in benign tumours.
- Evidence of distal lymphatic or blood metastasis.
Malignant melanoma Commonest site
- Below knee in females.
- Back in males.
- Sole of foot in Negroes.
Malignant melanoma Differential diagnosis (Pigmented tumours):
- Pigmented acanthoma.
- Pigmented basal cell carcinoma.
- Pigmented papilloma.
- Kaposi’s sarcoma.
Malignant melanoma Spread:
- Direct By continuity and contiguity.
- Lymphatics – This occurs along lymphatic vessels (by permeation and embolism) to the regional lymph glands.
- Melanomas of limbs often give rise to secondary cutaneous deposites along the draining lymphatic vessels.
- Spread usually occurs in deep fascial plexus i.e. from superficial to deep fascia.
- Sometimes secondary in gland is proved by histology, but no primary is found clinically.
- This may be due to non-pigmented primary (amelanotic melanoma).
“Differential applications of traditional vs cutting-edge practical exam techniques: Questions answered”
Malignant melanoma Role:
Malignant melanoma Blood:
- It involves the liver, lungs, kidney or any bone containing red marrow.
- Liver secondaries characteristically take place years after even apparently successfully operated ocular melanomas.
- Secondaries in small intestine may present as acute abdomen (Intussusception, haemorrhage, perforamtion).
Malignant melanoma Histological classification:
Malignant melanomas are classified into five types (clark).
- Level I – In situ melanoma (above basement membrane).
- Level II – Involvement of basement membrane upto papillary dermis.
- Level III – Involvement of papillary dermis upto but not invading reticular dermis.
- Level IV – involvement of reticular dermis.
- Level V – Involvement of subcutaneous tissue.
Malignant melanoma Treatment of Primary:
Malignant melanoma Principles:
- No biopsy.
- No local excision and skin graft from the same leg because lymphatic spread may have already occurred at the donor’s site.
- Sufficiently wide and deep excision down to deep fascia (deep fascia is spared in presnt day concept of treatment) with at least 5 cm. Radius but more proximally.
- Deep fascia is spared because
- It has not got any lymphatic and only rarely, lymphatics pass through it (eg. Arm, Knee).
- Cosmetic result is better.
- No primary closure is done following excision. If skin margin can be approximated – excision is bound to be inadequate leading to invariable recurrence over the scar.
Malignant melanoma Treatment of Lymph nodes:
- If primary is close by, “Block dissection in continuity” is the treatment of choice, hence only applicable in proximal part of the limbs.
- If in the distal part of the limb.
- Primary is dealt by wide excision and glands are observed, and block dissection is performed later if glands become palpable.
- Primary is dealt first and glands even if not palpable are excised at the same time.
- Primary is dealt as before and then block dissection is performed after waiting for 3- 4 weeks.
- If the glands were palpable – it could either be due to infection of spread.
- If due to infection – glands would get smaller, still block dissection is indicated after 3-4 weeks because even though not palpable microscopic deposits may be found.
- If due to spread the case is advanced so waiting for 3-4 weeks probably wouldn’t matter in the ultimate result, but by waiting normal drainage of malignant cells from the neighbouring lymphatics will take place in the intervening period.
- This is now the standard method of treating lymphatic secondaries. Lymphangiography performed pre and post operatively helps to locate even clinically non-palpable glands. This also helps to detect the efficacy of block dissection.
- No palpable glands
- Endolymphatic irradiation
- Cytotoxic drugs
- Radiotherapy – Resistant in 80% cases, sensitive in 20% cases (specially in conjunctiva).
- Immunological therapy B.C.G (Vaccinia vaccine) – by intralesional injection (0.1 ml) is used
- Prior to excision or
- For recurrence after excision.
Papilloma
- It is a benign epithelial tumour having a central core of connective tissue containing blood vessels covered by a layer of epithelium, which may be squamous, columnar or transitional.
Papilloma Diagnosis:
- Usually pedunculated.
- Surface sometimes smooth, sometimes granular or villous.
- Well circumscribed.
- No ulceration of skin.
- No induration.
- Not fixed to deeper structure.
- Site – scalp, chest wall, axilla, medial side of groin.
Complications
- Ulceration.
- Haemorrhage.
- Sepsis.
- Keratinisation.
- Malignancy – papillary carcinoma or malignant papilloma.
Signs of malignancy
- Rapidly growing with the surface becoming relatively smooth.
- Pedunculated growth becomes sessile.
- Consistency changing to hard inspite of the absence of keratinisation.
- Ulceration.
- Bleeding – profuse and frequent.
- Fixity due to invasion of underlying tissues.
Treatment excision.
False papilloma (Wart) – This occurs as a result of viral infection.
- Common sites – finger, face, etc.
- Oval in shape.
- Smooth surface.
- Pea like structure.
- Translucent.
Papilloma Treatment: Excision with or without diathermy coagulation.
Squamous Cell Carcinoma (Epitheloma)
Malignant epithelial tumour arising from the prickle cell layer is known as Epidermoid or Squamous cell carcinoma.
Squamous Cell Carcinoma (Epitheloma) Pre-malignant conditions:
- Exposure to sunlight for prolonged period – solar hyperkeratosis.
- Exposure to X-ray causing dermatitis.
- Exposure to chemicals and gas causing prolonged irritation, Kangri cancer, pipe smokers, chimney sweepers.
- Xeroderma pigmentosa.
- Epidermolysis bullosa cystica.
- Bowen’s disease.
- Paget’s disease of Penis or Nipple.
“Can bioinformatics revolutionize practical exam classification? FAQs provided”
Squamous Cell Carcinoma (Epitheloma) Clinical features:
- Common sites – sites of irritation – e.g. lips (lower-common), cheek, scalp, forehead, ear, trunk, oesophagus, lower extremity, penis, etc. (Head and Neck – 77%, Hand- 13% and others 10%).
- Starts (mode of presentation)
- As a nodule.
- As a cauliflower growth.
- As an ulcerative growth.
- Age usually above 40 years.
- Fairly rapid growth, hence there s shorter history than basal cells carcinoma.
- Ulcer:
- Squamous cell carcinoma produces surface keratinisation, which needs to be removed before examining the ulcer.
- Irregular, raised, thick and everted margin.
- Floor covered by grayish white slough.
- Base marked induration.
- Fixed to underlying structure.
- Early involvement of lymph gland – hard and discrete (except in Marjolin’s ulcer where lymph node enlargement is late as lymph vessels get occluded in the scar tissue).
Squamous Cell Carcinoma (Epitheloma) Treatment
- Growth
- Preliminary, biopsy taking a piece of the growth and normal skin must be done for histological confirmation and grading.
- Wide excision covering 2-2.5 cm of healthy tissues around the growth is the treatment of choice in all cases of squamous cell carcinomas especially if detected early.
- The area of excision is covered by skin graft.
- In case the lesion is small excision and biopsy can be combined.
- Amputation, may be tried only in limbs in advanced stages when there is involvement of bone.
- Irradiation is indicated when the tumour is at an inaccessible site or in late stage of the disease.
- Following irradiation biopsy from the margin of the irradiated portion must be sent to make sure disease has been properly treated.
- Glands – Block dissection is performed if glands are mobile and removable, but deep X-ray is given if they are fixed.
- An epidermoid carcinoma differs from a basal cell carcinoma in following respects –
- Origin from prickle cells.
- Site – it can start from anywhere in the skin.
- Rate of growth – Rapid.
- Metastasis to lymph nodes – early and constant.
- Presence of cell nests and round cell infiltration.
- Long standing granulomas
- Syphilis
- Lupus vulgaris
- Leprosy.
- Chronic ulcers
- Osteomyelitis
- Hidranitis suppurative
- Long standing venous ulcer.
- Main etiological factor for the development of Squamous cell carcinoma – Sunlight.
Important clinical features of Squamous cell carcinoma
- Irregular ulcer
- Everted edges
- Indurated base
Squamous Cell Carcinoma (Epitheloma) Types of biopsy
- Biopsy from the edge of the ulcer – edge.
- Biopsy of a wedge of the tissue – wedge biopsy.
Question 26. What are the advantages?
Answer:
Wedge biopsy
- It represents the pathology.
- The junction between pathology and normal.
- Edge biopsy disadvantage.
- The sample may contain only necrotic tissue and proper evaluation may not be possible.
Question 27. What are the characteristic pathological features?
Answer:
- Pathologically they are tumours from epidermal keratinocytes.
- Invasive nests of cells are seen with variable central keratinisation and horn cell formation – epithelial nests or epithelial pearls.
- Mitosis is prominent.
- The cells may show variegated appearance.
- Majority of the cells are large and well differentiated with vesicular nuclei, prominent nucleoli and abundant cytoplasm.
- Features of anaplasia.
- Evidence of local invasion may be present.
- Epithelial pearl formation may not be seen in
- Rapidly growing tumour.
- Oesophagus.
- Bladder.
Question 28. How will you manage the case?
Answer:
- Conformation of the diagnosis – Biopsy.
- Investigation:
- Radiology of the part.
- Involvement of periosteum of a bone.
- Chr. Osteomyelitis.
- C.B.P.
- Urine analysis.
Question 29. What are the methods of management?
Answer:
- Surgery
- Radiotherapy
- Chemotherapy.
Question 30. What is the role of surgery?
Answer:
- Small lesions – curative excision.
- Lesions adherent to cartilage, bone etc.
- When lymph nodal metastasis developed.
- Well differentiated tumours.
Question 31. What are the methods of surgical management?
Answer:
- Curative excision or wide excision.
- With 2 cm clearance all around.
- About 1 cm clearance in cosmetically important areas.
- Radical excision with block dissection of Lymph nodes.
- Amputation of the limb.
- When wide excision amounts to amputating the limb.
- When it is adherent to deeper structures like bone.
Question 32. What is the role of radiotherapy?
Answer:
- For poorly differentiated tumours.
- Tumours on head and neck.
- Post operative radiotherapy for residual tumour.
- When the patient is not for surgical excision.
Question 33. What is the role of chemotherapy?
Answer:
- Few tumours – Bleomycin – if small and superficial like penile lesions.
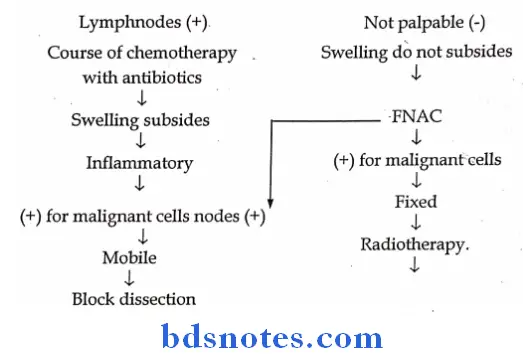
Question 34. How will you manage Lymphnodal enlargement.
Answer:
Basal Cell Carcinoma (Rodent Ulcer)
- It is called rodent ulcer as the tumour eats like a rodent.
Basal Cell Carcinoma (Rodent Ulcer) Features:
- Age – usually above 40 years.
- Sex – male predominantly affected.
- Common sites – situated over face above the line joining the angle of mouth and ear lobule. Unusually starts at the inner canthus of eye or in the nasolabial furrow, but may occur in jaw and tibia. (Head and Neck 95%, Trunk 3% and Limbs 2%).
- Very slowly progressing.
- Character:
- Irregular ulcer wit rolled out margin. Induration is marked.
- At places frequent attempt of healing by fibrosis may be found.
- Floor – covered by granulation tissue, sometimes deeper structures may be exposed e.g. bones or air sinus.
Basal Cell Carcinoma (Rodent Ulcer) Macroscopically following features may be seen:
- Ulcer with rolled edge – ulcerative type may be hypertrophic or atrophic.
- Cystic (classically pearly white with surface blood vessel).
- Pigmented (cf. malignant melanoma).
- Invasive.
- Lymph gland – not palpable.
- Painless.
Basal Cell Carcinoma (Rodent Ulcer) Origin:
- From the basal cells of epidermis.
- From the misplaced cells of epidermis.
- From the sebaceous and sweat glands.
Basal Cell Carcinoma (Rodent Ulcer) Treatment:
- Excision with at least 1 cm. margin followed by suturing of margins if possible. If the gap is big skin grafting is necessary.
- Alternative treatment Irradiation therapy either by radium or by deep X-ray. Usually low voltage is required but recurrence is common and after one recurrence deep X-ray usually fails. In these cases wide excision with skin grafting remains the only treatment.
- If the underlying bone is exposed – the bone is protected by some insulating material (e.g. lead) while deep X-ray is applied.
Question 35. How does it spreads?
Answer:
- Local invasion.
- Dissimination by blood stream or lymphatics do not occur.
Question 36. What are the indications for radiotherapy?
Answer:
- Extensive lesions.
- Elderly patient.
Modality of radiotherapy – 4000-6000 c GY units
- Fractioning the dose over several weeks.
- Reduces scarring.
- Reduces necrosis.
Question 37. What is the role of surgery?
Answer:
- Share excisions.
- Excision with primary suturing.
- Excision with sliding or a full thickness graft.
“Asymptomatic vs symptomatic effects of ignoring new trends in practical exams: Answered”
Question 38. What is the advantage of excision?
Answer:
- Good scar in plastic surgeons hands.
- Pathological confirmation – for total excision.
Question 39. Disadvantages of excision?
Answer:
- Inadequate removal from depth.
- Recurrence.
- Can be over come by – p.o radiotherapy.
Question 40. What is the role of cryosurgery?
Answer:
- Small lesions.
- Elderly.
- Cosmetically good result.
Question 41. What is curettage and cautery?
Answer:
- Small lesions.
- Elderly patient.
Question 42. What is the role of local chemotherapy?
Answer:
- 5-flourouracil – superficial and small lesions.
- High recurrence rates.
- Head and Neck
- Cervical lymphadenitis
- Tuberculosis
- Malignant
- Hodgkin’s
- Secondary metastasis
- Carcinoma of cheek
- Carcinoma of tongue
- Carcinoma of lip
- Carcinoma of mouth
- Salivary tumour
- Parotid and sub-mandibular
- Carotid body tumour
- Cold abscess
- Cystic hygroma
- Thyroid swelling
- Branchial cyst
- Thyroglossal cyst
- Salivary glands in neck
- Sub-mucous cyst in mouth
- Rannula
- Thyroid
- Adenoma
- Carcinoma
- Multinodular goiter.
Leave a Reply