Cysts Of Oral Cavity Important Question And Answers
Question 1. Classify cysts of oral cavity. Describe pathogenesis, histopathology and clinical features and roentgenographic appearance of dentigerous cyst.
Or
Define and classify cysts. Write in detail about dentigerous cyst.
Or
Classify odontogenic cyst. Describe pathogenesis, clinical radiological and histopathologic features of dentigerous cyst.
Or
Classify odontogenic cysts and describe clinical features, radiographic and histopathologic features of dentigerous cyst.
Or
Classifyodontogenic cyst. Describe pathogenesis, clinical, radiological features along with histopathology of dentigerous cyst.
Answer. Cyst is defined as “A pathological cavity having flid,semifluid or gaseous contents and which is not created by accumulation of pus.” — Kramer (1974)
“Understanding the role of oral cysts in dental health: Q&A explained”
Classification of Cyst of Oral Cavity by Mervin Shear
Cysts of the Jaws
- Epithelial:
- Developmental:
- Odontogenic:
- Gingival cyst of infants
- Odontogenic keratocyst (Neoplasm)
- Dentigerous cyst
- Eruption cyst
- Lateral periodontal cyst
- Gingival cyst of adults
- Botryoid odontogenic cyst
- Glandular odontogenic cyst
- Calcifying odontogenic cyst (neoplasm)
- Odontogenic:
- Developmental:
Read And Learn More: Oral Pathology Question And Answers
“Importance of studying oral cavity cysts for better diagnostic outcomes: Questions explained”
- Non-odontogenic:
- Naso palatine duct cyst
- Naso labial cyst
- Midpalatal raphe cyst of infants
- Median palatine, median alveolar
- Median mandibular cyst
- Globulo maxillary cyst
- Non-odontogenic:
- Inflammatory
- Radicular cyst, apical and lateral
- Residual cyst
- Paradental cyst and mandibular infected buccal cyst
Inflammatory collateral cyst
- Nonepithelial (pseudocysts)
- Solitary bone cyst
- Aneurysmal bone cyst
“Common challenges in diagnosing oral cavity cysts effectively: FAQs provided”
Cyst Associated With Maxillary Antrum
- Benign mucosal cyst of the maxillary antrum
- Post-operative maxillary cyst
Cyst of the Soft Tissues Of Mouth, Face And Neck
- Dermoid and epidermoid cyst
- Lymphoepithelial cyst (branchial cyst)
- Thyroglossal duct cyst
- Anterior medial lingual cyst (intra lingual cyst of foregut origin)
- Oral cyst with gastric or intestinal epithelium
- Cystic hygroma
- Nasopharyngeal cyst
- Thymic cyst
- Cyst of salivary glandsmucous extravasation cyst
- Mucous retention cyst, ranula, polycystic disease of the parotid.
- Parasitic cyst hydatid cyst, cysticercus cellulosae, trichinosis.
“Steps to explain types of oral cavity cysts: Odontogenic vs non-odontogenic: Q&A guide”
Classification of Odontogenic Cyst
WHO (2017) Classification of Odontogenic Cysts
- Odontogenic cysts of inflammatory origin
- Radicular cyst
- Inflammatory collateral cysts
- Odontogenic developmental cysts
- Dentigerous cyst
- Odontogenic keratocyst
- Lateral periodontal cyst and botryoid odontogenic cyst
- Gingival cysts
- Glandular odontogenic cyst
- Calcifying odontogenic cyst
- Orthokeratinized odontogenic cyst.
“Role of dentigerous cysts in oral pathology: Questions answered”
Dentigerous Cyst
- It is also called a follicular cyst or a pericoronal cyst
- It is the odontogenic cyst that surrounds the crown of the impacted tooth.
Pathogenesis Of Dentigerous Cyst
- Intrafollicular theory: Dentigerous cyst is caused by flid accumulation between reduced enamel epithelium and enamel surface which result in a cyst in which crown is located within the lumen.
- Extrafollicular theory: Dentigerous cyst may arise by proliferation and cystic transformation of islands by odontogenic epithelium in connective tissue wall of dental follicle or even outside dental follicle and this transformed epithelium then unite with lining follicular epithelium forming cystic cavity around tooth crown.
“Early warning signs of issues addressed by understanding oral cyst types: Common questions”
Clinical Features Of Dentigerous Cyst
- It is usually found in children.
- Most lesions are present in the 2nd and 3rd decades with male predilection.
- Most common site of the cyst are the mandibular and maxillary third molar and maxillary cuspid areas, since these are most commonly impacted teeth.
- Generally, it is painless but may be painful if it is infected.
- Dentigerous cyst has potential to become an aggressive
lesion with expansion of bone and subsequent facial asymmetry. - There is extreme displacement of teeth, severe root resorption of adjacent teeth and pain.
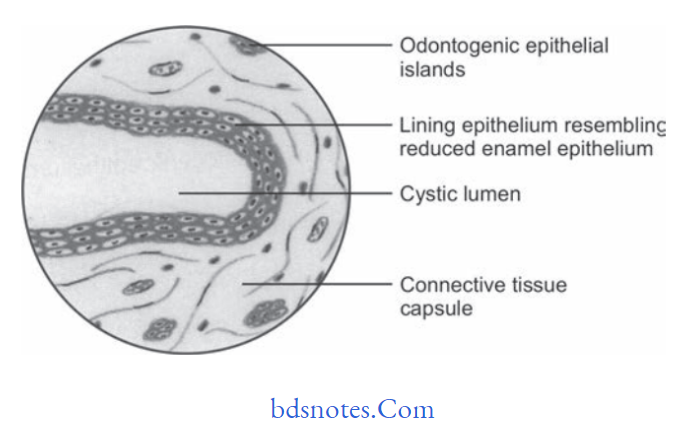
Histopathological Features Of Dentigerous Cyst
“Asymptomatic vs symptomatic effects of ignoring oral cyst classification: Q&A”
- The epithelial lining consists of two to four layers of flattened nonkeratinizing cells and the epithelium and connective tissue interface is flt.
- It is usually composed of thin connective tissue wall with a thin layer of stratifid squamous epithelium lining the lumen.
- Rete pegs formation is absent except in case of secondarily infected cyst.
- Connective tissue wall is frequently quite thickened and composed of very loose firous connective tissue.
- Inflammatory cells commonly infiltrate connective tissue
- It also shows Rushton bodies within the lining epithelium which are peculiar linear and often curved hyaline bodies.
- Content of cystic lumen is usually thin watery yellow flid and is occasionally blood tinged.
“Steps to educate patients about oral cavity cysts and their importance: Q&A format”
Roentgenographic/Radiological Features
- There is presence of well-defied radiolucency having hyperostotic borders.
- An unerupted tooth is also seen around the radiolucency
- Cyst is unilocular but at times it appears multilocular.
- Bony margins of the cyst are well defied as well as sharp.
- If infection persists margins are ill defied.
- Cyst can envelop the crown symmetrically, but it can expand laterally from the crown of tooth. Tooth can also be displaced away in any direction.
- Resorption of roots of adjacent teeth can also be seen.
- The floor of the maxillary sinus gets displaced with the expansion of cyst.
Leave a Reply