Tumors Of Salivary Glands Important Question And Answers
Question.1. Describe the clinical features, histology, pathogenesis and differential diagnosis of pleomorphic adenoma.
Or
Classify salivary gland tumors. Describe in detail the clinical features, histopathology, and treatment of pleomorphic adenoma.
“Understanding salivary gland tumors through FAQs: Q&A explained”
Answer.
Salivary Gland Tumor Classification by WHO (2017)
- Malignant tumors
- Mucoepidermoid carcinoma 8430/3
- Adenoid cystic carcinoma 8200/3
- Acinic cell carcinoma 8550/3
- Polymorphous adenocarcinoma 8525/3
- Clear cell carcinoma 8310/3
- Basal cell adenocarcinoma 8147/3
- Intraductal carcinoma 8500/2
- Adenocarcinoma, NOS 8140/3
- Salivary duct carcinoma 8500/3
- Myoepithelial carcinoma 8982/3
- Epithelial myoepithelial carcinoma 8562/3
- Carcinoma ex pleomorphic adenoma 8941/3
- Secretory carcinoma 8502/3*
- Sebaceous adenocarcinoma 8410/3
- Carcinosarcoma 8980/3
- Poorly differentiated carcinoma
- Undifferentiated carcinoma 8020/3
- Large cell neuroendocrine carcinoma 8013/3
- Small cell neuroendocrine carcinoma 8041/3
- Lymphoepithelial carcinoma 8082/3
- Squamous cell carcinoma 8070/3
- Oncocytic carcinoma 8290/3
“Importance of studying salivary gland tumors for better diagnostic outcomes: Questions explained”
Read And Learn More: Oral Pathology Question And Answers
Uncertain malignant potential
- Sialoblastoma 8974/1
- Benign tumors
- Pleomorphic adenoma 8940/0
- Myoepithelioma 8982/0
- Basal cell adenoma 8147/0
- Warthin tumor 8561/0
- Oncocytoma 8290/0
- Lymphadenoma 8563/0*
- Cystadenoma 8440/0
- Sialadenoma papilliferum 8406/0
- Ductal papillomas 8503/0
- Sebaceous adenoma 8410/0
- Canalicular adenoma and other ductal adenomas 8149/0
- Non-neoplastic epithelial lesions
- Sclerosing polycystic adenosis
- Nodular oncocytic hyperplasia
- Lymphoepithelial sialadenitis
- Intercalated duct hyperplasia
- Benign soft tissue lesions
- Haemangioma 9120/0
- Lipoma/sialolipoma 8850/0
- Nodular fasciitis 8828/0
- Haematolymphoid tumors
- Extranodal marginal zone lymphoma of mucosaassociated lymphoid tissue (MALT lymphoma) 9699/3
*These new codes were approvedbythe IARC/WHO CommitteforICD-0. - Pleomorphic adenoma or benign mixed tumor is most common neoplasm of salivary glands. The parotid gland is mostly affcted by the tumor.
- Extranodal marginal zone lymphoma of mucosaassociated lymphoid tissue (MALT lymphoma) 9699/3
“Common challenges in diagnosing salivary gland tumors effectively: FAQs provided”
Clinical Features
- Pleomorphic adenoma develops in 5th and 6th decade of life.
- It produces slow-growing, well-delineated exophytic growth of salivary gland.
- Surface of lesion is smooth and lobulated and generally there is no pain.
- Neoplasm is usually soft or rubbery in consistency and is freely movable.
- Parotid gland lesion is usually superfiial and often arises in superfiial lobe as a small mass overlying angle of mandible or anterior to external ear.
- Sometimes, lesion can be multinodular and can assume an enormous size especially in long standing lesions.
- In buccal mucosa or lip pleomorphic adenoma presents small, painless, well defied, movable nodular lesion with intact overlying mucosa.
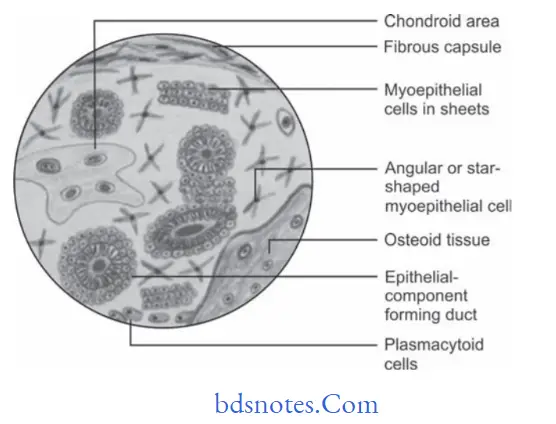
Histopathology
- Neoplasm often exhibits proliferation of glandular epithelial cells in form of diffuse sheet or clusters.
- Neoplastic cells are polygonal, spindle or stellate shape and have tendency to form duct-like structures.
- Duct like structures are of varying size, shape, number and are widely distributed within lesion.
- Histologically, each duct like structure exhibits an inner row of cuboidal or columnar cells and outer row of spindle shape myoepithelial cells.
- Epithelial cells show “squamous metaplasia” and sometimes, there may be formation of keratin pearls by metaplastic epithelial cells.
- Connective tissue undergoes hyalinization to form structureless homogeneous material.
- Mucoid materials in myochondroid are composed of glycosaminoglycAns and consist mainly of chondroitin sulfate.
- Complete capsule is never present.
Malignant salivary gland tumors
“Why is early detection critical for managing salivary gland tumors? Answered”
Pathogenesis
- There is presence of myoepithelial cells and reserve cells arranged in intercalated duct.
- The intercalated duct reserve cells can differentiate into ductal and myoepithelial cells and the later can then undergo mesenchymal metaplasia.
- Dardick’s theory: It is the most accepted theory. They state that a neoplastically altered epithelial cell with the potential for multidirectional differentiation may be histologically responsible for the pleomorphic adenoma.
Differential Diagnosis
- Polymorphous low-grade adenocarcinoma: It shows perineural growth and is infiltrative into peri glandular tissue. It form small tubular structures or single cord of cells at periphery.
- Carcinoma Ex pleomorphic adenoma: Features of malignancy are seen in background of mixed tumor.
- Epithelial myoepithelial carcinoma: Two families of cells are seen, larger epithelial cells are arranged in tubular or acinar crystals and small myoepithelial cells seen mainly as “bipolar” spindly nuclei.
- Warthin’s tumor: It consists of bilayered oncocytic epithelium, the inner cells of which are tall columnar with fie granular and eosinophilic cytoplasm and slightly hyperchromatic nuclei. The outer layer consists of basaloid cells.
- Oncocytoma: It consists of sheets of large polyhedral cells with abundant granular eosinophilic cytoplasm. These cells have centrally located nuclei which can vary from small and hyperchromatic to large and vesicular.
- Mucoepidermoid carcinoma: It consists of mixture of mucus producing cells ad squamous (epidermoid) cells. Mucus cells vary in shape and consist of foamy cytoplasm while epidermoid cells have squamoid features, polygonal shape,intercellular bridges and rarely keratinization. It is of three types, i.e. low grade, high grade and intermediate grade.
- Adenoid cystic carcinoma: It is a malignant tumor. It consists of mixture of myoepithelial cells and ductal cells which have varied arrangement. Three major pattrns are cribriform, tubular and solid. It also shows increased nuclear atypia.
- Various mesenchymal tumors such as nerve sheath tumor,smooth muscle tumor.
“Steps to explain causes of salivary gland tumors: Benign vs malignant factors: Q&A guide”
Treatment
- Pleomorphic adenomas are best treated by surgical excision.
- Pleomorphic adenoma present in superficial lobe of parotid gland undergoes superficial parotidectomy with identification and preservation of facial nerve.
- For tumors of deep lobe of parotid gland, total parotidectomy is necessary with preservation of facial nerve if possible.
- Pleomorphic adenoma in submandibular gland is treated by total removal of the gland along with tumor.
- Pleomorphic adenoma of hard palate is excised down to periosteum, including overlying mucosa.
- At other oral sites lesion enucleates easily through the incision site.
“Role of genetic mutations in causing salivary gland tumors: Questions answered”
Question.2.Classify salivary gland diseases. Write about clinical features and histopathology of mucoepidermoid carcinoma.
Or
Classify salivary gland neoplasm. Discuss in detail mucoepidermoid carcinoma.
Or
Classify salivary gland disorders describe mucoepi dermoid carcinoma.
Or
Classify salivary gland tumors. Write in detail about mucoepidermoid carcinoma.
Answer. Enumeration of salivary gland tumors.
Salivary Gland Tumor Classification by WHO (2017)
- Malignant tumors
- Mucoepidermoid carcinoma 8430/3
- Adenoid cystic carcinoma 8200/3
- Acinic cell carcinoma 8550/3
- Polymorphous adenocarcinoma 8525/3
- Clear cell carcinoma 8310/3
- Basal cell adenocarcinoma 8147/3
- Intraductal carcinoma 8500/2
- Adenocarcinoma, NOS 8140/3
- Salivary duct carcinoma 8500/3
- Myoepithelial carcinoma 8982/3
- Epithelial myoepithelial carcinoma 8562/3
- Carcinoma ex pleomorphic adenoma 8941/3
- Secretory carcinoma 8502/3*
- Sebaceous adenocarcinoma 8410/3
- Carcinosarcoma 8980/3
- Poorly differentiated carcinoma
- Undifferentiated carcinoma 8020/3
- Large cell neuroendocrine carcinoma 8013/3
- Small cell neuroendocrine carcinoma 8041/3
- Lymphoepithelial carcinoma 8082/3
- Squamous cell carcinoma 8070/3
- Oncocytic carcinoma 8290/3
Uncertain malignant potential
“How does abnormal cell growth lead to salivary gland tumors? FAQ explained”
- Sialoblastoma 8974/1
- Benign tumors
- Pleomorphic adenoma 8940/0
- Myoepithelioma 8982/0
- Basal cell adenoma 8147/0
- Warthin tumor 8561/0
- Oncocytoma 8290/0
- Lymphadenoma 8563/0*
- Cystadenoma 8440/0
- Sialadenoma papilliferum 8406/0
- Ductal papillomas 8503/0
- Sebaceous adenoma 8410/0
- Canalicular adenoma and other ductal adenomas 8149/0
- Non-neoplastic epithelial lesions
- Sclerosing polycystic adenosis
- Nodular oncocytic hyperplasia
- Lymphoepithelial sialadenitis
- Intercalated duct hyperplasia
- Benign soft tissue lesions
- Haemangioma 9120/0
- Lipoma/sialolipoma 8850/0
- Nodular fasciitis 8828/0
- Haematolymphoid tumors
- Extranodal marginal zone lymphoma of mucosaassociated lymphoid tissue
(MALT lymphoma) 9699/3
- Extranodal marginal zone lymphoma of mucosaassociated lymphoid tissue
*These new codes were approved by the IARC/WHO Committee for ICD-0.
Mucoepidermal tumor/mucoepidermoid Carcinoma
Mucoepidermal tumor is an unusual type of malignant salivary gland neoplasm with varying degree of aggressiveness.
“Early warning signs of issues addressed by understanding salivary gland tumor pathogenesis: Common questions”
Pathogenesis
- It can occur due to entrapment of retromolar mucous glands in the mandible which undergo malignant transformation.
- Developmentally induced embryonic remnants of submaxillary gland within the mandible.
- Mucous secreting cells which are commonly found in pluripotential epithelial lining of dentigerous cyst associated with impacted third molars undergo neoplastic transformation.
- Neoplastic transformation as well as invasion from lining of maxillary sinus.
Clinical Features
- Tumor occurs at the age of 30 to 50 years.
- Tumor involves the parotid and minor salivary glands of palate, lips, buccal mucosa, tongue and retromolar areas.
- Tumor occurs as slowly enlarging painless mass which leads to the stimulation of pleomorphic adenoma.
- Facial nerve palsy and pain is present at times.
- Lowgrade mucoepidermoid carcinomas is a slowly enlarging painless mass which rarely exceeds 5 cm in diameter.
- Highgrade mucoepidermoid carcinomas grow rapidly and cause pain. It also infitrates the surrounding tissues and metastatize to regional lymph nodes.
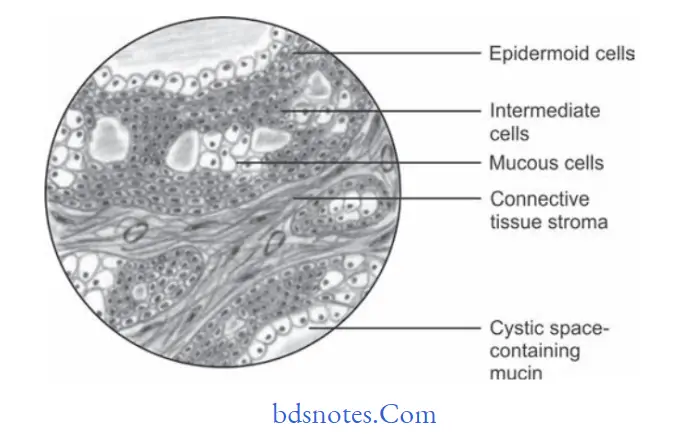
Histopathology
- Tumor is encapsulated and consists of three types of cells:
1. Mucus-secreting cells
2. Epidermoid cells
3. Intermediate type of cells. - According to distribution of these cells, the mucoepidermoid cells are divided into three grades:
1. Well differentiated tumor or low-grade tumor
2. Poorly diffrentiated tumor or high-grade tumor
3. Intermediategrade tumor- Low-grade tumor: They show well formed glandular structures and prominent mucin filed with cystic space, minimal cellular atypia and high proportion of mucus cells.
- Intermediate grade tumor: They have solid areas of epidermoid cells or squamous cells with
intermediate basaloid cells. Cyst formation is seen but is less prominent than observed in lowgrade tumor. - High-grade tumor: They consist of cells present as solid nests and cords of intermediate basaloid cells and epidermoid cells, prominent nuclear pleomorphism and mitotic activity is noted. Necrosis and perineural invasion may be present.
“Asymptomatic vs symptomatic effects of ignoring salivary gland tumor triggers: Q&A”
Differential Diagnosis
- Pleomorphic adenoma
- Squamous cell carcinoma
- Metastatic carcinoma
- Adenocarcinoma.
Treatment
Conservative excision with the preservation of facial nerve.
The affected submandibular gland should be removed entirely.
Treatment for minor glands is surgical.
“Can targeted interventions improve outcomes using knowledge of salivary gland tumor etiology? Answer provided”
Question.3. Enumerate the disease of salivary gland and describe in detail adenoid cystic carcinoma.
Or
Classify various diseases affcting salivary glands.
Describe in detail adenoid cystic carcinoma.
Or
Classify salivary gland tumors. Describe in detail cylindroma.
Answer.
Adenoid Cystic Carcinoma/Cylindroma
It is a malignant neoplasm arising from glandular epithelium of either major or minor glands.
It is also known as cylindroma.
Clinical Features
- Tumor arises at the age of 50–70 years and is more common in females.
It frequently affects parotid and other common sites are minor glands of palate, tongue, lacrimal glands, breast, prostrate, etc. - Lesion produces, slow enlarging growth with frequent surface ulceration.
- Pain is common feature and neurological signs are anesthesia, paresthesia or palsy frequently develops.
- Often there is fiation of tumor to underlying structures along with the local invasion.
- It has marked tendency to spread through perineural spaces and usually invades well beyond the clinically apparent borders.
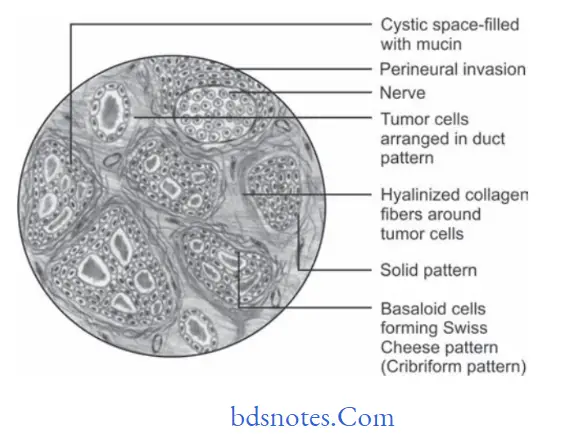
Histopathology
- It is characterized by the presence of numerous, small, darkly stained polygonal or cuboidal cells. Cells often resemble basal cells of oral epithelium and have hyperchromatic nuclei and minimum mitotic activity.
- Double layer of tumor cells are arranged in duct-like pattrn and contains eosinophilic coagulum at center,because of this lesion typically produces “Swiss Cheese appearance”.
- Stroma of connective tissue tumor is hyalinized which surrounds tumor cells by forming structural pattrn of many cylinders.
- Most striking feature of adenoid cystic carcinoma is spread of tumor cells via perineural or intraneural spaces. This is known as neurotrophism. This accounts for high rates in the recurrence of tumors.
“Steps to educate patients about salivary gland tumors and their importance: Q&A format”
Treatment
By wide surgical excision.
Question.4. Write note on Sjogren’s syndrome.
Or
Write short note on Sjogren’s syndrome.
Or
Write in brief on Sjogren’s syndrome.
Answer. It is a chronic inflammatory autoimmune disorder that affects salivary, lacrimal and other exocrine glands.
Types
- Primary Sjögren’s syndrome: It is also known as Sicca syndrome. It consists of dry eyes, i.e. xerophthalmia and dry
mouth, i.e. xerostomia. - Secondary Sjögren’s syndrome: It consists of dry eyes, i.e.
xerophthalmia, dry mouth, i.e. xerostomia and collagen disorders, i.e. rheumatoid arthritis or systemic lupus erythematous.
Clinical Features
- Xerostomia is present with unpleasant taste, soreness and diffilty in eating dry fruits.
- Patient also complains of xerophthalmia and arthralgia
- Severe tiredness is present.
- There is cobblestone appearance of tongue.
- There is often secondary acute bacterial sialadenitis and rapid progressive dental caries.
- Burning sensation present in the eyes.
- Parotid gland is predominantly affcted, sometimes submandibular and minor glands can also be affcted.
Histopathology
- Initially infiltration of lymphocytes in intralobular ducts of involved salivary gland.
- There is atrophy of salivary gland acini and proliferation of ductal epithelial cells.
- Hyperplasia of ductal epithelium obliterates ductal lumen and there is formation of myoepithelial islands.
- In fullydeveloped lesions entire glandular tissue is replaced by myoepithelial islands which are surrounded by proliferating lymphoid tissue.
Treatment
- Use of systemic steroids
- Antibiotic eye drops
- Antifungal drugs
- Maintenance of oral hygiene.
“Role of counseling in clarifying goals for managing salivary gland tumors: Questions answered”
Question.5. Write short note on mucocele.
Answer. It is also called as mucus extravasation phenomenon or mucus escape reaction.
Mucocele is defined as swelling caused by pooling of saliva at the site of injured minor salivary gland.
Types
- Mucus extravasation cyst: In this mucus is extravasated into the connective tissue and is devoid of epithelial lining.
It is also known as pseudocyst. - Mucus retention cyst: In this mucin is retained in the dilated salivary excretory duct and is lined by epithelium.
This is known as true cyst.
Clinical Features
- They are common and occur on the inner aspect of lower lip. They may also occur on palate, cheek, tongue and flor of the mouth.
- They occur most frequently during third decade of life.
- Patient complains of painless swelling. The swelling may suddenly develops at mealtime and may drain simultaneously at interval.
- Swelling is round, oval or smooth.
- The superficial cyst appears as bluish mass and if inflamed it is fluctuant, soft, nodular, and dome-shaped elevation.
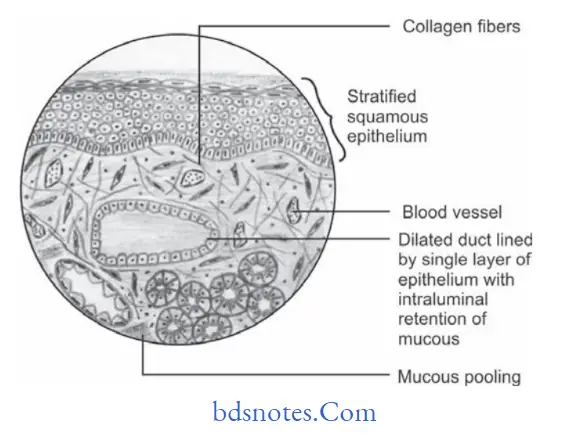
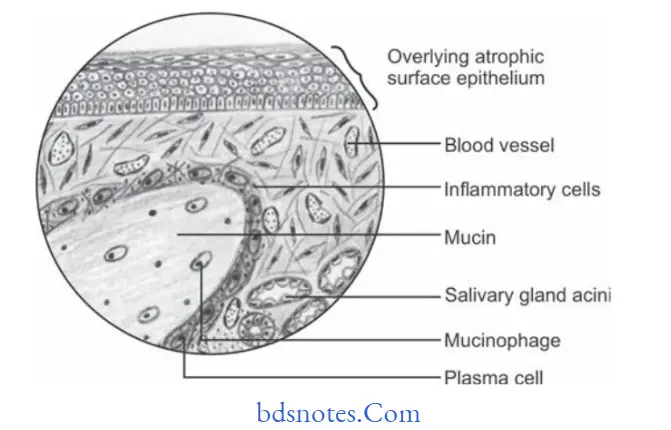
Histopathological Features
“How do educational materials explain complex salivary gland tumor concepts? FAQ explained”
In poorly defined cyst, it consists of irregularly shaped poorly defied pools that contain eosinophilic mucinous material, numerous vacuolated macrophages which are known as mucinophage.
- In well-defied cysts the periphery consists of granulation tissue or condensed firous tissue or both and is infitrated by vacuolated macrophages, lymphocytes, polymorphonuclear leukocytes including eosinophils.
- Lumen of cyst like cavity is filled with eosinophilic coagulum.
Treatment
Complete excision of cyst under local anesthesia should be done.
Question.6.Classify salivary gland tumor. Write briefl about etiopathogenesis, clinical features, histopathology and radiographic fidings of mucoepidermoid carcinoma.
Or
Write about clinical features, etiopathogenesis and histopathology of mucoepidermoid carcinoma.
Answer.
Etiopathogenesis
- As per the multicellular theory mucoepidermoid tumor arise from the excretory duct cells of salivary gland.
- During development, the retromolar mucous glands get entrapped in the mandible which undergoes neoplastic transformation and leads to formation of intraosseous mucoepidermoid carcinoma.
Radiographic Findings
- Mucoepidermoid carcinoma appear as a unilocular or multilocular expanding mass.
- Margins are corticated, well defied.
- At times lesion show honeycomb or soap bubble appearance.
- Lamina dura of associated teeth is lost.
- Inferior border of mandible, buccal and cortical plates are displaced and thinned.
“Asymptomatic vs symptomatic effects of poor communication about salivary gland tumors: Answered”
Question.7 Write short note on sialadenitis.
Answer. Inflammation of salivary gland is known as sialadenitis.
Etiology
- Viral Infections: Mumps, CMV virus, Coxsackie virus and parainflenza.
- Bacterial Infections
- Blockage of duct by sialolithiasis
- Congenital strictures
- Compression by adjacent tumor
- Recent surgeries of salivary glands.
Clinical Features
- It occours most commonly in parotid gland.
- Affected gland is swollen and painful and overlying skin is warm and erythematous.
- Lowgrade fever and trismus may be present.
- A purulent discharge is observed from the duct orifie.
Histopathology
- Accumulation of neutrophils is observed within the ductal system and acini.
- Chronic sialadenitis is characterized by scattred or patchy infitration of parenchyma by lymphocytes and plasma cells.
- Atrophy of acini is common.
Sialographic Features
- It demonstrates ductal dilatation proximal to the area of obstruction.
- In acute sialadenitis sialography is contraindicated.
- In chronic sialadenitis Stenson’s duct may show a characteristic sialographic pattrn known as sausaging which reflcts a combination of dilatation plus ductal strictures from scar formation.
Treatment
- Antibiotics should be given to patient
- Proper hydration should be maintained
- If necessary go for surgical intervention.
Question.8.Classify salivary gland pathologies. Discuss in detail warthin’s tumor.
Or
Write in detail on Warthin’s tumor.
Or
Write short note on Warthin’s tumor.
Answer.
Warthin’s Tumor
It is also known as papillary cystadenoma lymphomatosum or adenolymphoma.
It is the second most common tumor of salivary glands.
Pathogenesis
- According to the most accepted theory, the tumor arises in salivary gland tissue entrapped within paraparotid or intraparotid lymph nodes during embryogenesis.
- According to Allegra Warthin’s tumor is a delayed hypersensitivity disease, the lymphocytes being an immune reaction to the salivary ducts which undergo oncocytic change.
Etiology
- Smoking
- Epstein Barr virus infection.
Clinical Features
- It occurs during 6th and 7th decades of life with average age of 62 years.
- Men are most commonly affcted
- Tumor is superfiial lying beneath the parotid capsule or protruding towards it.
- The tumor appear as a slow growing painless nodular mass over the angle of jaw. Lesion can be bilateral too.
- Tumor is 1 to 3 cm in diameter and is spherical in shape.
- Surface of the lesion is smooth
- On palpation lesion is fim and is non-tender.
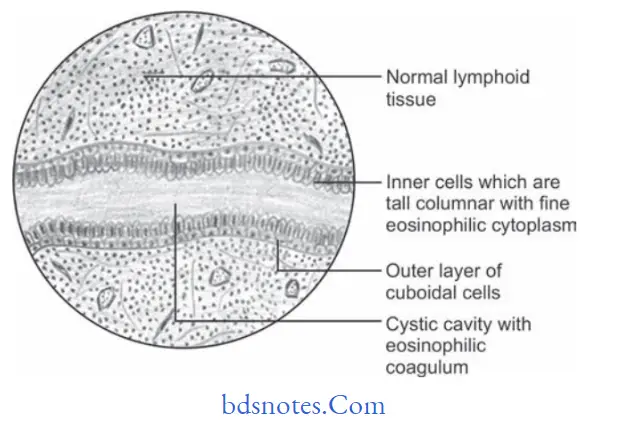
Histopathology
- Tumor is composed of epithelial and lymphoid tissue.
- Lesion is an adenoma undergoing cyst formation with papillary projections in cystic spaces.
- Lymphoid matrix exhibit germinal centers.
- Cyst is lined by a bilayered oncocytic epithelium, the inner cells of which are tall columnar with fie granular and eosinophilic cytoplasm and slightly hyperchromatic nuclei.
- The outer layer consist of basaloid cells.
- An eosinophilic coagulum is present within the cystic spaces.
- The numerous lymphocytic component may represent normal lymphoid tissue within which tumor is developed.
Treatment
Surgical excision is treatment of choice.
“Early warning signs of knowledge gaps in patient understanding of salivary gland tumors: Common questions”
Question.9. Write short note on sialolithiasis.
Answer. Sialolithiasis is also known as salivary duct calculi or salivary duct stone.
Sialolith are the calcifid structures which develop within the salivary ductal system.
Pathogenesis
Salivary duct stone are formed by deposition of calcium salts around a central nidus which consists of altered salivary mucins, desquamated epithelial cells, bacteria, foreign bodies or products of bacterial decomposition.
Clinical Features
- Sialoliths occur during 2nd to 4th decades of life.
- Submandibular gland ductal system is the most common site for occurrence of sialolith.
- Sialoliths cause episodic pain or swelling of the affcted gland during meal or thought of the meal.
- If it is not treated for longer time exacerbation of the lesion occur and systemic symptoms occur such as malaise and fever.
- Pus can exude from the ductal orifie and surrounding soft tissues are inflamed.
- At times ulceration of the overlying mucosa is evident which allows calculus to extend in flor of oral cavity.
- Saliva can never be seen oozing out from the orifie of the affcted duct.
Histopathology
- Calcifid mass exhibit concentric lamellation which surrounds the nidus of amorphous deposits.
- Associated ductal epithelium shows squamous, oncocytic or mucus cell metaplasia.
- Periductal inflammation is also present.
- Ductal obstruction is frequently associated with acute or chronic sialadenitis of feeding gland.
Treatment
- Small calculi are removed by manipulation or increasing the salivation.
- Larger calculi require surgical exposure for removal.
Question.10. List benign epithelial tumors of salivary gland. Discuss in detail pleomorphic adenoma.
Answer. Salivary Gland Tumor Classifiation by WHO (2017)
Benign Tumors
- Pleomorphic adenoma 8940/0
- Myoepithelioma 8982/0
- Basal cell adenoma 8147/0
- Warthin tumor 8561/0
- Oncocytoma 8290/0
- Lymphadenoma 8563/0*
- Cystadenoma 8440/0
- Sialadenoma papilliferum 8406/0
- Ductal papillomas 8503/0
- Sebaceous adenoma 8410/0
- Canalicular adenoma and other ductal adenomas 8149/0
- Nonneoplastic epithelial lesions
- Sclerosing polycystic adenosis
- Nodular oncocytic hyperplasia
- Lymphoepithelial sialadenitis
- Intercalated duct hyperplasia
- Benign soft tissue lesions
- Haemangioma 9120/0
- Lipoma/sialolipoma 8850/0
- Nodular fasciitis 8828/0
- Haematolymphoid tumors
- Extranodal marginal zone lymphoma of mucosaassociated lymphoid tissue (MALT lymphoma) 9699/3
*These new codes were approved by the IARC/WHO
Committee for ICD-0.
Question.11.Classify and discuss ameloblastoma.
Answer. Ameloblastoma is classified, according to WHO and the International Agency for Research on Cancer, 2017,as a benign epithelial odontogenic tumor. It is further classified as:
Classification Of Ameloblastoma WHO 2017
- Ameloblastoma
- Ameloblastoma, unicystic type
- Ameloblastoma, extraosseous/peripheral type
- Metastasizing ameloblastoma
Leave a Reply