Trigeminal Neuralgia: Causes, Symptoms, and Treatment
It is also called Tic Douloureux, trifacial neuralgia, or Fothergill’s disease.
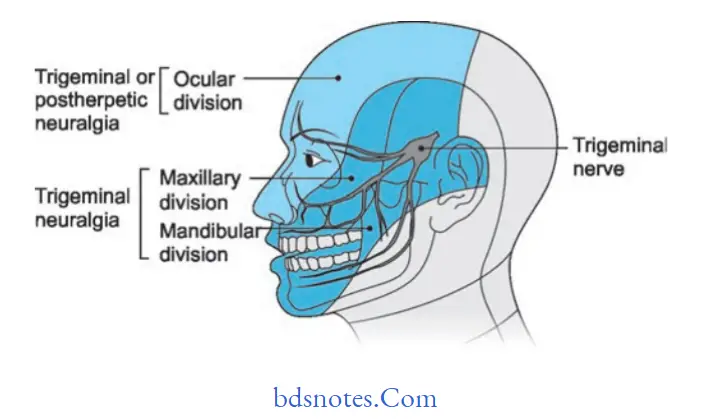
Trigeminal neuralgia is an extremely painful condition along the distribution of any branches of the trigeminal nerve.
Trigeminal Neuralgia
Trigeminal neuralgia Etiology
- Dental pathosis at times leads to trigeminal neuralgia.
- Due to excessive traction, divisions of the trigeminal nerve are affected, which leads to trigeminal neuralgia.
- Allergic and hypersensitivity reactions may lead to trigeminal neuralgia.
- Mechanical factors such as pressure are caused by aneurysms of the internal carotid artery.
- Secondary lesions such as carcinomas of maxillary antrum, and carcinoma of the nasopharynx lead to trigeminal neuralgia.

Read And Learn More: Neurological and Facial Disorders: Causes, Diagnosis, and Treatment Strategies
“Understanding The Causes Of Trigeminal Neuralgia“
Trigeminal Neuralgia Symptoms
Trigeminal neuralgia Clinical Features
- It occurs in middle-aged and older people.
- Female predilection is seen.
- Pain is paroxysmal, lasts for a few minutes, and is of extreme intensity.
- Pain is usually limited to the distribution of trigeminal nerve and is unilateral. At times, pain is bilateral, too.
- Pain is provoked by obvious stimuli to the face. A touch, a draft of air, any movement of the face as in talking, chewing, yawning, or swallowing.
- Pain attacks are precipitated by touching some “trigger zone” on the face, i.e., the vermilion border of the lip, the ala of the nose, the cheek, and around the eyes.
Patients usually avoid touching the skin over these areas.
The patient has an unshaven face, avoids brushing, andundergoeso dental extraction. - Objective signs or sensory loss are demonstrated on examination.
- The onset of pain is sudden and tends to persist for weeks or months before remitting spontaneously.
Trigeminal Neuralgia Causes
“Can Trigeminal Neuralgia Affect Both Sides Of The Face”
Trigeminal neuralgia Treatment
Trigeminal neuralgia Medical treatment
- Carbamazepine (Tegretol) has a special effect on paroxysmal pain. This is considered to be the best conservative treatment for trigeminal neuralgia.
As an initial dose, 100 mg twice daily till relief is established. - Dilantin: Diphenylhydantoin, an anticonvulsant drug, has been recommended, effective when given orally, 300 to 400 mg/day.
- Recently, baclofen, an antispastic drug, hass alsobeeng used.
- A combinationOff ilantintin and carbamazepine may also be given.
- Clonazepam, an antiepilept, wasic found to be useful.
- Anti-inflammatory agents like indomethacin and sa hort course ofsteroids aree useful.
Trigeminal Neuralgia Diagnosis
“Step-By-Step Guide To Managing Trigeminal Neuralgia”
Trigeminal neuralgia Surgical treatment
- Infection of the nerve with an anesthetic solution: Local anesthetics of various types are injected near the peripheral branches of the trigeminal nerve to serve to provide temporary relief from pain.
- Injection ofthe nerve with alcohol:
- The most popular material, alcohol, can be placed directly into the area where a nerve exits from the skull or peripherally.
- When alcohol contracts the nerve, neurolysis occurs distal to the injection site.
- Generally, 95% alcohol is used, or procaine or monocaine 2%, chloroform 5%, absolute alcohol 70%, and Ringer’s solution 23% can also be used.
- Nerve sectioning and nerve evolution (peripheral neurectomy):
This procedure is more lasting and effective than an injection with alcohol.
Peripheral neurectomy results ina high degree of success in the elimination of pain.
Trigeminal Neuralgia Treatment
“Tips To Prevent Trigeminal Neuralgia Flare-Ups”
- Electrocoagulation of gasserian ganglion: Diathermy apparatus is placed in the gasserian ganglion to coagulate and destroy it.
- Percutaneous radiofrequency trigeminal neurolysis: It is performed by insertion of a temperature monitoring electrode through the foramen ovale into the trigeminal ganglion.
Advantages include decreased mortality and morbidity and permanent cure. - Rhizotomy: Actual cutting of trigeminal sensory root results in permanent anesthesia in most patients.
- Bulbar trigeminal tractotomy: The descending tract of the trigeminal nerve may be cut in the area of the medulla oblongata to induce loss of pain and temperature sensation.
Leave a Reply