Thyroid Cancer Treatment
Describe the classification, clinical features, and management of thyroid neoplasia.
Or
Write about clinical features of papillary and follicular carcinoma of thyroid and management
Answer.
Classification of Thyroid Neoplasia
Benign
- Follicular adenoma—Colloid, embryonal, fetal
- Hurthle cell adenoma
- Colloid adenoma
- Papillary adenoma.
Malignant (Dunhill classifiation)
“Best Treatments For Thyroid Cancer”
Diffrentiated:
- Papillary carcinoma
- Follicular carcinoma
- Papillo-follicular carcinoma behaves like papillary carcinoma of thyroid
- Hurthle cell carcinoma behaves like follicular carcinoma.
Undifferentiated:
- Anaplastic carcinoma
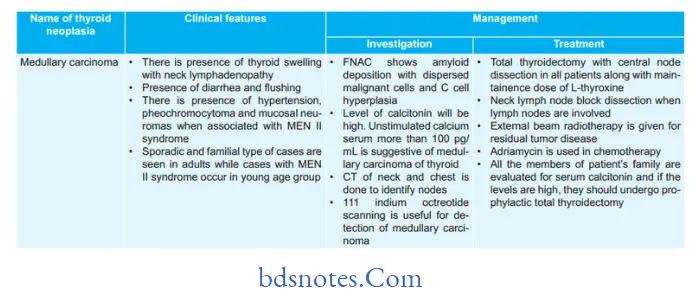
Medullary carcinoma
Malignant lymphoma
Secondaries in thyroid from colon, kidney, melanoma and breast.
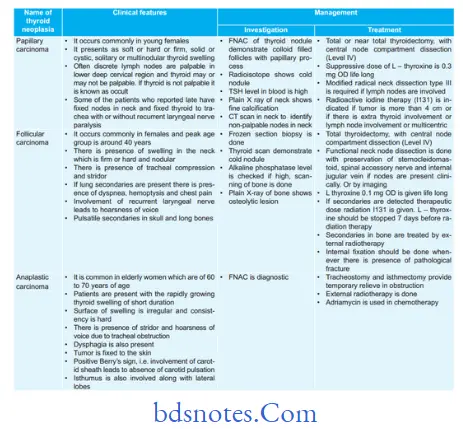
Clinical Features and Management of thyroid neoplasias
“Types Of Thyroid Cancer Treatments”
“Best Practices For Managing Thyroid Cancer Recovery”
Thyroid Cancer Treatment
Describe the classification, clinical features, treatment, and complications of thyroid malignancy.
Answer. Classification of thyroid malignancy Or Dunhill
Classification
- Differentiated (80%)
Papillary carcinoma (60%)
Follicular carcinoma (17%)
Papillo-follicular carcinoma
Hurthle cell carcinoma. - Undifferentiated—20%
Anaplastic carcinoma (13%). - Medullary carcinoma (6%)
- Malignant lymphoma (4%)
- Secondaries in thyroid—from colon, kidney,melanoma, breast.
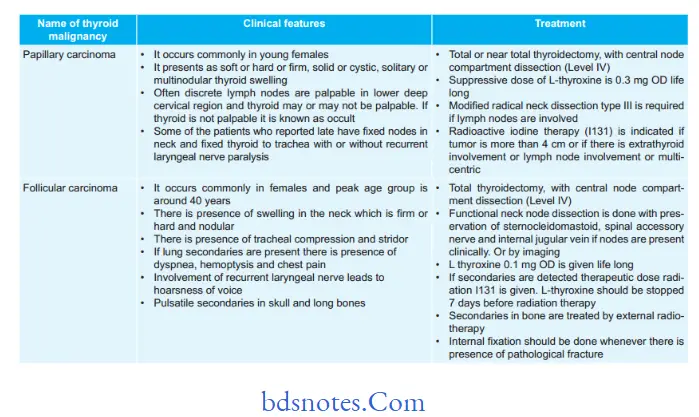
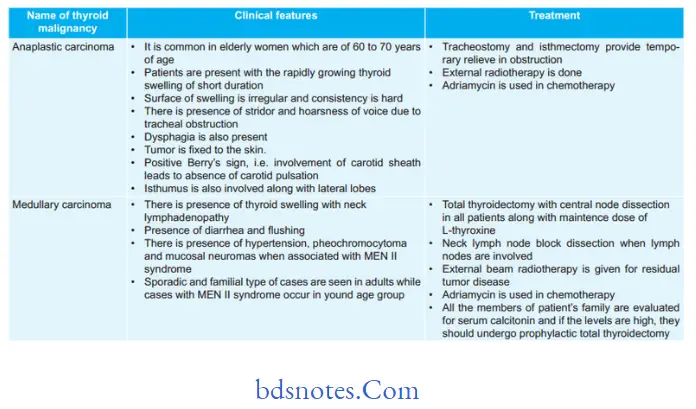
Clinical Features and treatment of thyroid Malignancy
“The Role Of Blood Tests In Monitoring Thyroid Cancer Treatment”
Complications of thyroid Malignancy
Complications of thyroid malignancy are associated with the thyroidectomy procedure followed as surgical treatment in most of thyroid malignancies.
So following are the complications:
Hemorrhage
- Chances of reactionary hemorrhage are present which is more dangerous and occurs within 6 to 8 hours after surgery.
It occurs due to slipping of ligatures, coughing, etc. - Tension hematoma develop deep-to-deep fascia it com presses the larynx.
Respiratory Obstruction
It occur due to hematoma or laryngeal edema, due to tracheomalacia or bilateral recurrent laryngeal nerve palsy.
Recurrent Laryngeal Nerve Palsy
It can be transient or permanent. Transient recover in 3 weeks to 3 months. It presents with hoarseness of voice, aphonia, aspiration and ineffctive cough.
“Comprehensive Overview Of Thyroid Cancer Treatment Options”
Hypoparathyroidism
It is temporary and due to vascular spasm of parathyroid glands. It occurson 2nd and 5thpost-operative day. It presents with weakness,positive Chvostek’s sign, carpopedal spasm, and convulsion.
Thyrotoxic Crisis
It occurs in thyrotoxic patient which is inadequately prepared for thyroidectomy.
Injury to external laryngeal nerve
It leads to weakening of cricothyroid muscle which causes alteration in pitch of voice, voice fatigue, breathy voice, and frequent throat clearing.
Hypothyroidism
It reveals clinically after 6 months.
Stitch Granuloma
It can occur with or without sinus formation and is seen after the use of non-absorbable suture material.
Leave a Reply