Thyroglossal Duct Cyst
What is a thyroglossal duct cyst, and how does it develop?
Answer. Thyroglossal Cyst is a congenital tubular dermoid cyst.
- Thyroglossal Cyst arises from the thyroglossal duct, which extends from the foramen cecum at the base of the tongue to the isthmus of the thyroid gland.
- Thyroglossal Cyst is lined by pseudostratified, ciliated, and columnar or squamous epithelium which produces desquamated epithelial cells or mucus at times.
Thyroglossal Duct Cyst Surgery
“Best Practices For Thyroglossal Duct Cyst Surgical Management”
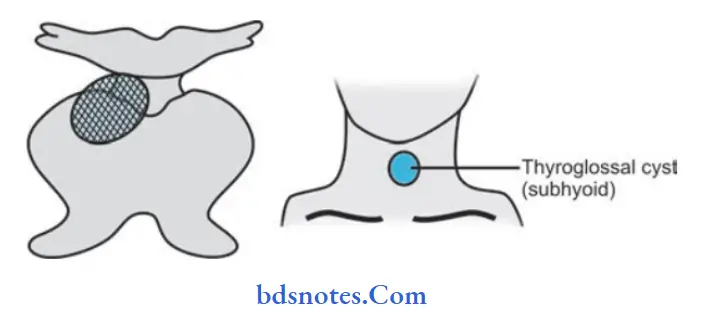
Thyroglossal Cyst Sites
- Subhyoid is the most common site
- At the level of thyroid cartilage
- Suprahyoid: Double chin appears
- At the foramen caecum
- At the level of cricoid cartilage
- At the floor of the mouth.

Read and learn More Cysts: Types, Causes, Symptoms, and Treatment
Congenital Thyroglossal Duct Cyst
“Can Thyroglossal Duct Cyst Recur After Surgery”
Thyroglossal Cyst Clinical Features
- Swelling is present in the midline towards the left side.
- Moves with deglutition as well as with the protrusion of the tongue.
- The patient is asked to open the mouth and keep the lower jaw still.
The examiner holds the cyst between the thumb and forefinger.
When the patient is asked to protrude the tongue, a “tugging sensation” can be felt. - Swelling is smooth, soft, fluctuant (cystic), non-tender, mobile, often transilluminate.
- The thyroid fossa is empty if there is no thyroid in the normal location.
- A thyroglossal cyst can get infected and may form an abscess. The Cyst wall contains lymphatic tissue so infection is common.
- Malignancy can develop in papillary carcinoma.
“The Role Of Imaging Tests In Thyroglossal Duct Cyst Diagnosis”
“Effective Ways To Manage Thyroglossal Duct Cyst Recovery”
Thyroglossal Cyst Treatment
Thyroglossal Cyst Differential Diagnosis
- Subhyoid bursa
- Pretracheal lymph node
- Dermoid cyst
- Solitary nodule of thyroid
- Submental lymph node
- Collar stud abscess.
Thyroglossal Cyst Investigations
- Radioisotope study
- Ultrasound of neck; T3, T4 and TSH estimation
- FNAC from the cyst.
Thyroglossal Duct Cyst In Children
Sistrunk operation
Excision of the cyst and also the full tract up to the foramen cecum is done along with the removal of the central part of the hyoid bone as the tract passes through it.
“Why Early Diagnosis Is Critical For Thyroglossal Duct Cyst“
Sistrunk operation Technique
- A thorough transverse neck incision was placed over the cyst, skin flap was raised above along with the platysma. Care should be taken not to open the cyst.
- Cyst with surrounding tissues is dissected up to the hyoid bone. Sternohyoid and thyrohyoid muscles are divided.
- The central part of the hyoid bone of l cm width is resected along with an intact tract within it.
- Geniohyoid and mylohyoid muscles are divided from the hyoid.
- Track with adjacent tissues is dissected above up to the foramen cecum.
- Adjacent tissues also should be removed because of possibility of multiple tracts which otherwise lead to recurrence or fitula formation.
- After this, the anesthetist is asked to apply digital pressure over the base of the tongue near the foramen cecum to facilitate the dissection and to confirm the reach up to the foramen cecum.
- The track is ligated at the foramen caecum and removed.
- If there is no normal thyroid gland after the surgery maintenance dose of L-thyroxine 0.l mg OD is given lifelong.
Thyroglossal Duct Cyst
Sistrunk operation Complications
- Recurrent thyroglossal fistula formation
- Hemorrhage/hematoma formation
- Infection.
Leave a Reply