Subgingival Calculus
Subgingival calculus is located below the crest of marginal gingiva and, therefore, is not visible on routine clinical examination.
Subgingival Calculus is also known as subgingival calculus.
“Importance Of Removing Subgingival Calculus For Gum Health”
Subgingival Calculus Location
The location and extent of subgingival calculus are evaluated by careful tactile perception with a delicate dental instrument known as an explorer.
Subgingival Calculus Composition
In this salivary proteins are absent; more magnesium whitlockite, lesser brushite and octacalcium phosphate; sodium content increases with pocket.
Subgingival Calculus Clinical Features
- Subgingival calculus is typically hard and dense and frequently appears dark brown and greenish black.
- Subgingival Calculus is found inside the gingival sulcus or the periodontal pockets.
- Subgingival Calculus appears first in interproximal areas where supragingival calculus already exists.
- This is occasionally seen on the dentures when it forms in narrow grooves, mainly those at the tooth–acrylic interface.
- Subgingival Calculus consistency is flint-like and is firmly adherent to the surface and is difficult to remove.
- Subgingival Calculus is not visible on routine oral examination, but can be found by tactile exploration.
“Difference Between Supragingival And Subgingival Calculus”
Subgingival Calculus Diagnosis
Direct vision
The subgingival calculus is seen directly:
- By using a gentle stream of air to reflect he gingival margin.
- By following the gingival surgery
- During periodontal surgery.
Indirect vision
The subgingival calculus is seen indirectly:
- When gingival margin is dried, dark color of subgingival calculus is seen via the marginal tissue.
- By probing
- A fine calculus probe (WHO 621 probe) is used to detect subgingival calculus.
- Ball end of the CPITN probe with a light touch determines the location of subgingival calculus, which appears as rough area or catch on the root surface.
- Exploring: Use of subgingival explorer no. TU – 17 can detect the subgingival calculus.
- Radiographs and transillumination.
“Understanding The Role Of Bacteria In Subgingival Calculus Formation”
Mineralization of Calculus
“Calculus is Defined as the hard deposit that forms by the mineralization of dental plaque and is generally covered by layer of unmineralized plaque.”
Classification of Dental Calculus
According to its relation to gingival margin. The dental calculus is classified as:
- Supragingival
- Subgingival
Supragingival Calculus
- Supragingival Calculusis tightly adherent calcified deposit that forms on the clinical crowns of the teeth above the free gingival margin. Supragingival Calculus is clinically visible. It is also called as salivary calculus because it forms from the saliva.
- Supragingival Calculus is white or yellow in color.
- Supragingival Calculus hard, clay-like consistency.
- Supragingival calculus is easily detachable from the tooth.
- Supragingival Calculus is commonly found on the buccal surface of maxillary molars and lingual surfaces of anterior mandibular teeth.
- Supragingival calculus consists of hydroxyapatite and octacalcium phosphate.
“Comprehensive Overview Of Subgingival Calculus And Its Significance”
Subgingival Calculus
- Subgingival Calculus lies below the crest of gingiva.
- Subgingival Calculus is dense dark brown or greenish black in color.
- Subgingival Calculus has hard or flint-like consistency.
- This is more firmly attached to tooth surface.
- Ratio of calcium to phosphate is high subgingivally and there is increase in sodium content along with depth of pockets.
- Subgingival calculus consists of more magnesium whitlockite and less brushite and octacalcium phosphate when comparison is done between supragingival and subgingival calculus.
Formation of Calculus
- Calculus is the dental plaque which had undergone mineralization.
- Calculus is formed by precipitation of mineral salts which starts between 1st and 14th day of plaque formation.
- Under 2 days plaque can be 50% mineralized and rest 60 to 90% of plaque is mineralized in 12 days.
- calcification starts in separate foci on inner surface of plaque.
- These foci of mineralization increase in size and coalesce to form solid mass of calculus.
- Calculus formation continues till it reaches its maximum level in about 10 weeks and 6 months.
Theories of Calculus Formation
Calculus Formation can be explained mainly under two categories:
Precipitation of minerals can occur from a local rise in the degree of saturation of calcium and phosphate ions, this is explained in:
- Booster mechanism: It is the main mechanism of precipitation which states that precipitation of calcium phosphate salts leads to local rise in degree of saturation of calcium and phosphate ions due to following ways:
- Increase in pH of saliva is because of:
- Loss of carbon dioxide or
- Production of ammonia by dental plaque bacteria or
- Protein degradation during stagnation leads to precipitation of calcium and phosphate salts by lowering the precipitation constant.
- Increase in pH of saliva is because of:
- Colloidal proteins in saliva bind to calcium and phosphate ions and maintain the supersaturated solution. As saliva stagnates in the oral cavity, colloids settle down and supersaturated stage is no longer maintained. This leads to precipitation of calcium and phosphate salts.
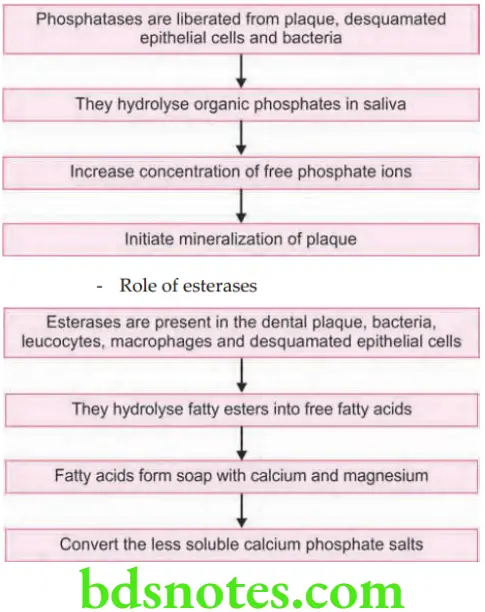
- Role of enzymes in precipitation of calcium and phosphate salts:
“Best Practices For Removing Subgingival Calculus Safely”
Role of phosphatases
Another concept that has been most widely held is “Epitactic Concept” (heterogeneous nucleation).
- According to this, seeding agents induce small foci of calcification. These foci enlarge and coalesce to form calculus. Hence, more appropriately called as heterogeneous nucleation. The seeding agents in calculus is not clearly known, but suspected agents could be, intercellular matrix of plaque, carbohydrate protein complexes and plaque bacteria.
Inhibition theory: This theory considers the possibility of calcification occurring only at specific sites because, there exists an inhibiting mechanism at non-calcifying sites. Wherever calcification occurs, the inhibitor is either altered or removed. One such inhibiting agents could be pyrophosphate which prevents the initial nucleus from growing, by possibly ‘poisoning’ the growth centers of the crystal.
Calculus Formation Etiologic Significance
- The non-mineralized plaque on the calculus surface is the principal irritant, but the underlying calcified portion may be a significant contributing factor. It does not irritate the gingiva directly but provides a fixed nidus for the continued accumulation of plaque and retains it close to the gingiva.
- Subgingival calculus may be the product rather than the cause of periodontal pockets.
- Plaque initiates gingival inflammation, which starts pocket formation, and the pocket in turn provides a sheltered area for plaque and bacterial accumulation.
- The increased flow of gingival fluid associated with gingival inflammation provides the minerals that convert the continually accumulating plaque into subgingival calculus.
- Although the bacterial plaque that coats the teeth is the main etiologic factor in the development of periodontal disease, the removal of subgingival plaque and calculus constitutes the cornerstone of periodontal therapy.
- Calculus plays an important role in maintaining and accentuating periodontal disease by keeping plaque in close contact with the ‘gingival tissue and creating areas where plaque removal is impossible.
“The Role Of Dental X-Rays In Diagnosing Subgingival Calculus”
Role of Microorganisms in Mineralization
- Mineralization of plaque starts extracellularly around both gram-positive organisms and gram-negative organisms. It may also start intracellularly.
- Filamentous organisms, diphtheroids, and Bacterionema and Veillonella species have the ability to form intracellular apatite crystals.
- Calculus formation spreads until the matrix and bacteria are calcified.
- Bacterial plaque may actively participate in the mineralization of calculus by forming phosphatases, which changes the pH of the plaque and induces mineralization, but the prevalent opinion is that these bacteria are only passively involved and are simply calcified with other plaque components.
Leave a Reply