Squamous Cell Carcinoma
Enumeration of malignant epithelial neoplasms/Tumors:
- Basal cell carcinoma
- Squamous cell carcinoma
- Verrucous carcinoma
- Adenoid squamous cell carcinoma
- Malignant melanoma
- Spindle cell carcinoma
- Primary intra-alveolar carcinoma
- Multicentric oral carcinoma.
squamous cell carcinoma
“Importance Of Early Detection Of Squamous Cell Carcinoma”
Squamous Cell Carcinoma
- Squamous cell carcinoma is defined as a malignant epithelial neoplasm exhibit squamous differentiation as characterized by formation of keratin and/or presence of intercellular bridges. (Pindborg et al, 1997)
- Squamous cell carcinoma is the commonest malignant epithelial tissue neoplasm of oral cavity. It is mostly derived from stratifid squamous epithelium.
squamous cell carcinoma
“Risk Factors For Developing Squamous Cell Carcinoma Of The Skin”
Squamous Cell Carcinoma Etiology
Following are the etiological factors which lead to squamous cell carcinoma:
- Tobacco smoking: Cigaretts, bidis, pipes, cigars and reverse smoking.
- Use of smokeless tobacco: Snuf dipping, gutkha, tobacco chewing, tobacco as a toothpaste.
- Alcohol: Drinking spirits, Drinking wines, drinking beers
- Diet anal nutrition: Vitamin A, B-complex and C defiiency,
- Nutritional defiiency with alcoholism.
- Dental factors: Chronic irritation from broken teeth, Illfitng or broken prosthesis.
squamous cell carcinoma skin
“Early Signs Of Squamous Cell Carcinoma On The Skin”
- Radiations: Actinic radiation, Xray radiation
- Viral infections: Herpes simplex virus (HSV), Human papilloma virus (HPV),
- Human immunodeficiency virus (HIV),
- EpsteinBarr virus (EBV).
- Chronic infections: Candidiasis, syphilis
- Genetic factors: Oncogenes, Tumor suppressor genes
- Pre-existing oral diseases: Lichen planus, PlummerVinson Syndrome, discoid lupus erythematosus, OSMF.
squamous cell carcinoma of the skin
Squamous Cell Carcinoma Clinical Features
- Carcinomas mostly occur in the 4th to 7th decades of life.
- Males are more commonly affcted
- Lower lip is the most common site, the second most common site is the lateral border of the tongue.
Among all intraoral sites, dorsum of the tongue and hard palate are the least common sites for oral squamous cell carcinoma. - Initial lesion may be asymptomatic or can be presented as white or red nodule or fisure over the oral mucosa.
- Initially the lesion is usually painless.
- More advanced lesions present either as a fast enlarging,exophytic or invasive ulcer or sometimes as a large tumor mass or a verrucous growth.
- Ulcerated lesion often shows persistent induration around the periphery with an elevated and everted margin.
“Understanding The Role Of Uv Radiation In Squamous Cell Carcinoma”
- Lesion can be painful either due to secondary infection or due to involvement of the peripheral nerves by the tumor cells. Lesion can also bleed easily.
- Lesions of flor of mouth often cause fiation of the tongue to the underlying structures with diffilty in speech and inability to open the mouth.
- When malignant tumor cells invade into the alveolar bone of either maxilla or mandible, they usually cause mobility or exfoliation of regional teeth.
- Involvement of inferior alveolar nerve often causes paresthesia of the lower teeth and the lower lip.
- Regional lymph nodes are often enlarged, tendered and fied; some of these nodes can be stony hard in consistency.
- Untreated lesions may sometimes destroy the oral tissues and extend into the skin on the outer surface of the face to produce a nodular or lobulated growth on the facial skin,which appears as an extraoral discharging sinus.
- Pathological fracture of the jaw bone may sometimes occur in untreated cases due to extensive destruction of the bone by the tumor.
“The Role Of Biopsy In Diagnosing Squamous Cell Carcinoma Accurately”
Squamous Cell Carcinoma Histological Features
Histological fiding as given by Broder’s grading for squamous cell carcinoma.
“Best Practices For Treating Squamous Cell Carcinoma Symptoms Safely”
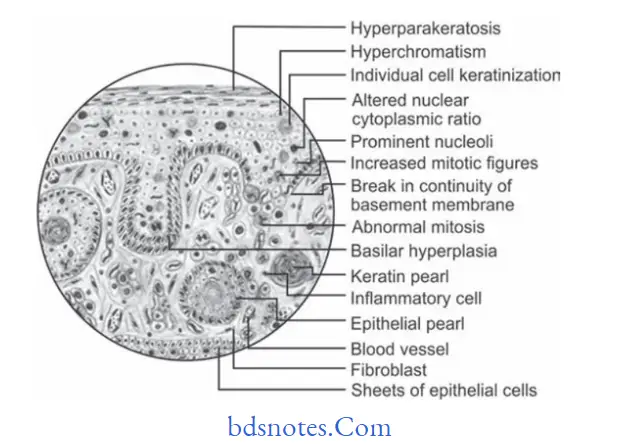
Well-differentiated Squamous Cell Carcinoma
- Most of the squamous cell carcinomas histologically belong to the well-diffrentiated category.
- In this lesion, the tumor epithelial cells to a large extent resemble the cells of the squamous epithelium both structurally and functionally.
- Tumor cells produce large amount of keratin in the form of “keratin pearls”.
- Tumor cells invade into the underlying connective tissue, where the cells proliferate further and give rise to the formation of many epithelial islands within the connective tissue stroma.
- Tumor cells often exhibit dysplastic features like cellular pleomorphism, nuclear hyperchromatism, individual cell keratinization, and altered nuclearcytoplasmic ratio, loss of cohesion, etc.
- Prognosis is better.
“Comprehensive Overview Of Squamous Cell Carcinoma And Its Causes”
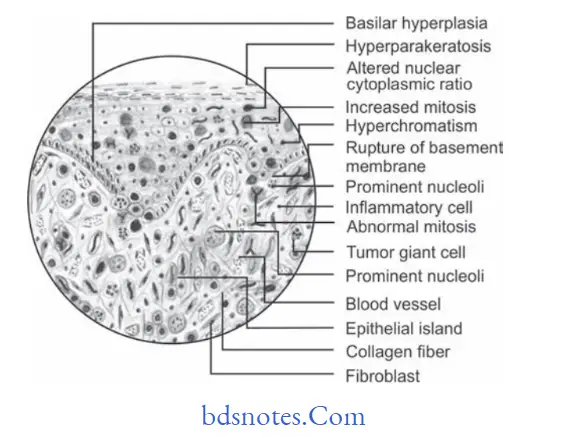
Moderately-differentiated squamous Cell Carcinoma
- Tumor cells are usually more severely dysplastic than that of the well-differentiated type.
- Growth rate of individual cells is more rapid and this is reflcted in greater number of mitotic fiures.
- There is formation of epithelial islands or cell nests, etc. are diminished since these tumor cells do not differentiate or
mature as much as the well differentiated type of cells do. - This tumor also carries a reasonably good prognosis.
“Tips To Prevent Complications From Squamous Cell Carcinoma Progression”
Poorly-differentiated squamous Cell Carcinoma
- In poorly differentiated squamous cell carcinoma, the malignant tumor cells produce no keratin .
- The tumor exhibits extensive cellular abnormalities with lack of normal architectural pattern and loss of intercellular bridges between the tumor cells.
- Mitotic cell division is extremely high and because of this,the neoplastic cells are often very immature and primitive looking and it is often very difficult even to recognize them as squamous epithelial cells.
- Prognosis is poor.
“Step-By-Step Guide To Diagnosing Squamous Cell Carcinoma Effectively”
Squamous Cell Carcinoma Investigations
- Biopsy of the involved area should be done for confimation of diagnosis.
- Toluidine blue test should be done.
- Tumor markers like cytokeratins, epithlial membrane
antigen, carcinoembryonic antigen (CEA) and alphafetoprotein should be used for detection of cancer.
Squamous Cell Carcinoma Treatment
Surgical excision of the involved site is the treatment of choice.
Leave a Reply