Shock – Critical Care Medicine
“Symptoms Of Shock In Critical Care”
Question 2. Describe etiopathogenesis and classification of shock. How will you manage hemorrhagic shock.
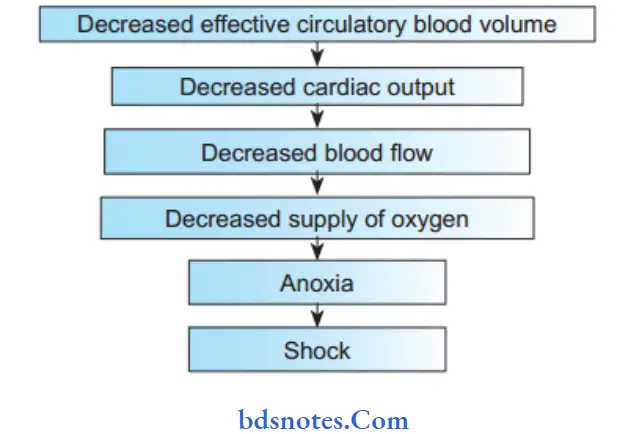
Answer. Etiopathogenesis
“Best Ways To Manage Shock In Critical Care”
Shock Classification
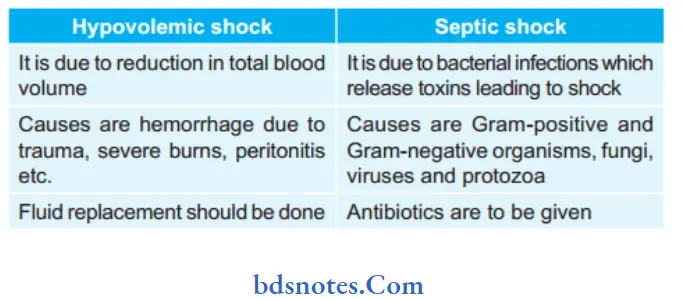
- Hypovolemic shock
- Cardiogenic shock
- Distributive shock:
- Septic shock
- Anaphylactic shock
- Neurogenic shock.
- Obstructive shock.
“Risk Factors For Shock In Icu Patients”
Management of Hemorrhagic Shock
- The primary treatment of hemorrhagic shock is to control the source of bleeding as soon as possible and to replace flid.
- In controlled hemorrhagic shock, where the source of bleeding has been occluded, fluid replacement is aimed toward normalization of hemodynamic parameters.
- In uncontrolled hemorrhagic shock, in which the bleeding has temporarily stopped because of hypotension, vasoconstriction, and clot formation, fluid treatment is aimed at restoration of radial pulse or restoration of sensorium or obtaining
- a blood pressure of 80 mm Hg by aliquots of 250 mL of lactated Ringer’s solution (hypotensive resuscitation).
- When evacuation time is shorter than 1 hour (usually urban trauma), immediate evacuation to a surgical facility is indicated after airway and breathing have been secured.
- When expected evacuation time exceeds 1 hour, an intravenous line is introduced and fluid treatment is started before evacuation. The resuscitation should occur before, or concurrently with, any diagnostic studies.
- Crystalloid is the fist flid of choice for resuscitation.
- Immediately administer 2 L of isotonic sodium chloride solution or lactated Ringer’s solution in response to shock from blood loss.
“Understanding The Causes Of Shock In Critical Care”
- Fluid administration should continue until the patient’s hemodynamics become stabilized.
- Because crystalloids quickly leak from the vascular space,each liter of flid expands the blood volume by 20–30%;therefore, 3 L of flid need to be administered to raise theintravascular volume by 1 L.
- Alternatively, colloids restore volume in a 1:1 ratio.
- Currently available colloids include human albumin,hydroxyethyl starch products (mixed in either 0.9% isotonic sodium chloride solution or lactated Ringer’s solution), or hypertonic saline-dextran combinations.
- Packed red blood cells (PRBCs) should be transfused if the patient remains unstable after 2000 mL of crystalloid resuscitation.
- For acute situations, O-negative non crossmatched blood should be administered.
- Administer 2 U rapidly, and note the response.
- For patients with active bleeding, several units of blood may be necessary.
Leave a Reply