Regressive Alterations Of The Teeth Important Question And Answers
Question.1. Write note on abrasion.
Or
Write short note on abrasion.
Or
Give descriptive note on abrasion.
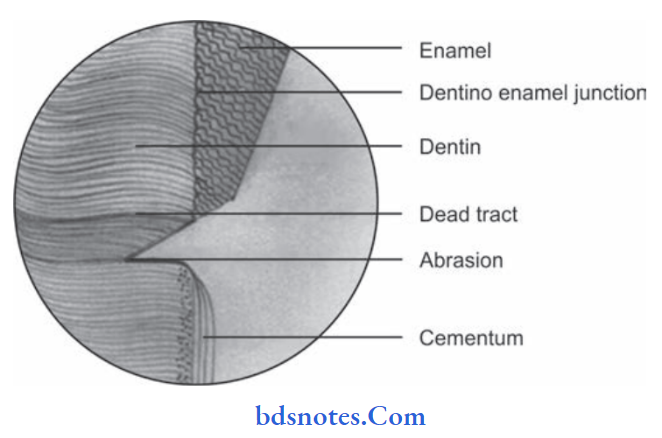
Answer. Abrasion is a pathological wearing of dental tissues by friction with the foreign substances independent of occlusion.
Abrasion Etiology
- Toothbrush abrasion
- Habitual abrasion, e.g. pipe smokers, toothpicks, and dental floss causes abrasion on proximal surfaces of teeth.
- Occupation abrasion, e.g. hairdressers, carpenters, and shoemakers.
- Abrasion by prosthetic appliances
- Ritual abrasions.
“Understanding regressive alterations of teeth through FAQs: Q&A explained”
Read And Learn More: Oral Pathology Question And Answers
Clinical Features Of Abrasion
- In abrasion of tooth the type and severity of surface will depend upon the duration and type of faulty habit adapted by the person.
- Toothbrush abrasion commonly occurs in cervical region of labial surface of incisors, canines and premolars.
- Maxillary teeth are more commonly affcted than the mandibular teeth.
- The produces a ‘V” shaped or wedge-shaped groove on the tooth with sharp angles and highly polished dentin surface.
- Toothbrush abrasion may cause gingival recession.
- Occupational abrasion often produces a small, deep, well-polished ditch on an incisal edge of teeth.
- Sever abrasion may cause opening of dentinal tubules and hence the patient experiences sensitivity in affected teeth due to hot and cold substances.
“Importance of studying regressive alterations of teeth for better diagnostic outcomes: Questions explained”
Treatment For Abrasion
- Adaptance of normal brushing habits prevents abrasion.
- Restorative treatment helps to keep the tooth surface intact and prevents further tooth wear.
“Common challenges in diagnosing regressive alterations effectively: FAQs provided”
Question.2. Write short note on sclerotic dentin.
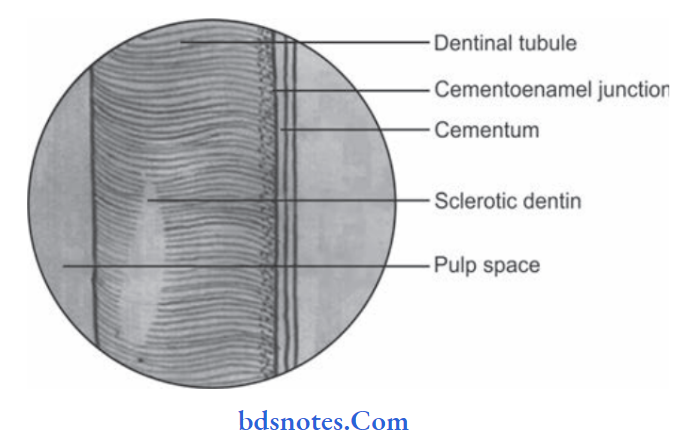
Answer. It is also known as transparent dentin
- Dentinal sclerosis is the condition characterized by calcification of dentinal tubules of the tooth.
- It is the regressive alteration in the tooth surface.
regressive changes in teeth
Sclerotic Dentin Etiology
- Injury to dentin by caries
- Aging process
- Abrasion or erosion of the tooth.
- Sclerotic dentin is found under the slowly progressing caries
- It reduces the permeability of dentin and prolongs pulp vitality.
- Dentinal sclerosis presents a translucent zone in the teeth which is seen in the tooth by the transmitted light.
- Sclerosis often decreases the conductivity of the tubules.
“Why is early detection critical for managing regressive alterations of teeth? Answered”
Question.3. Describe regressive changes in pulp.
Or
Write short note on age changes in pulp.
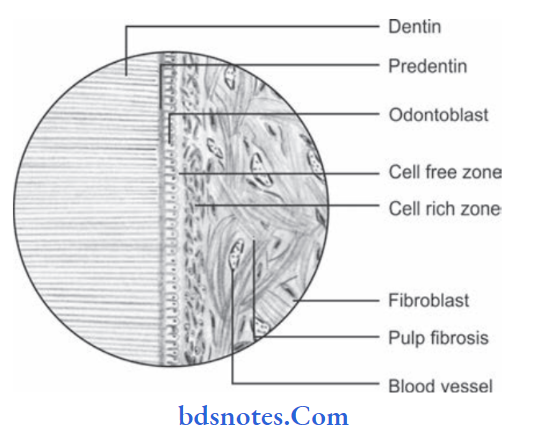
Answer. Regressive changes of pulp mean aging of pulp.
Cell Changes In Pulp
- Cells are characterized by decrease in size and number of cytoplasmic organelles.
- Pulpal fibrocytes or fibroblasts have abundant rough surface, cytoplasmic reticulum, Golgi bodies, and numerous mitochondria with well-developed cristae.
- Fibroblasts in aging pulp exhibit less perinuclear cytoplasm and long thin cytoplasmic processes.
Fibrosis Of Pulp
“Factors influencing success with regressive alteration treatment: Q&A”
- In aging pulp accumulation of diffuse firillar components and bundles of collagen fiers appears.
- Fiber bundles appear arranged longitudinally in bundles in radicular pulp and more diffse arrangement on coronal area.
- Increase in fier in pulp organ is generalized throughout the organ.
- Vascular changes occur in aging pulp organ.
- Atherosclerotic plaque may appear in pulpal vessels.
- Calcifications in the wall of blood vessels are found more often in region near the apical foramen.
- Outer diameter of vessel walls becomes greater, as collagen fiers increase in the medial and adventitial layer.
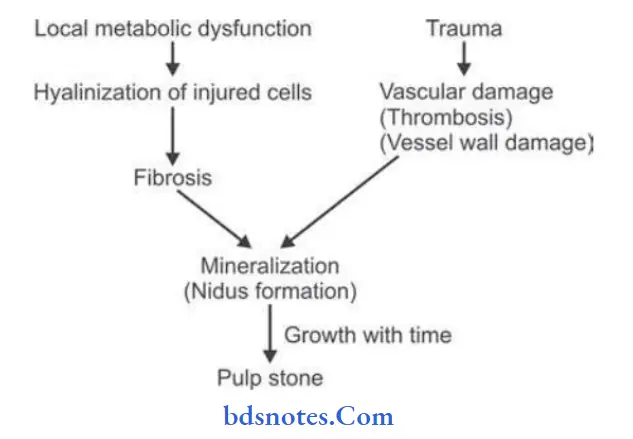
Pulp Stones/Denticles
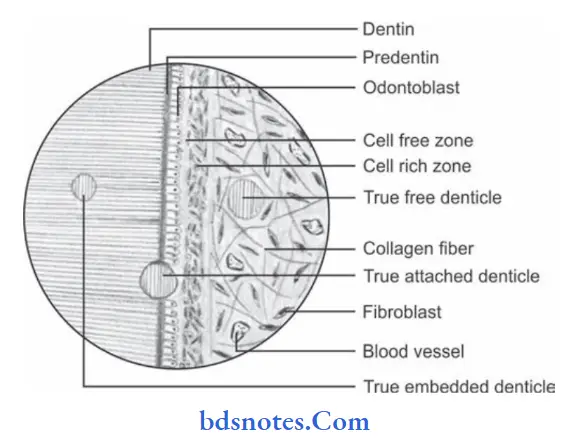
- Pulp stones and denticles are nodular calcifid masses appearing on coronal portions of the pulp organs.
- They are asymptomatic unless they impinge nerves on blood vessels.
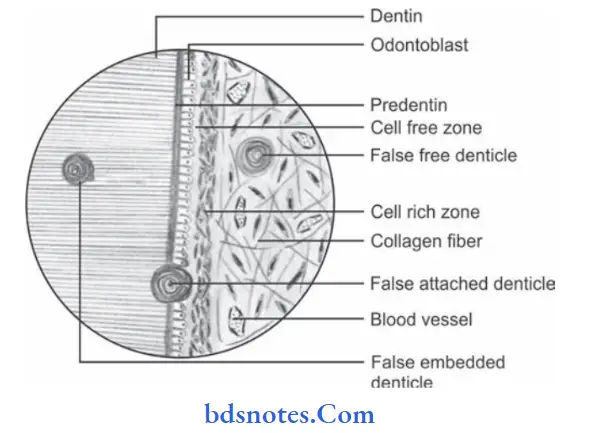
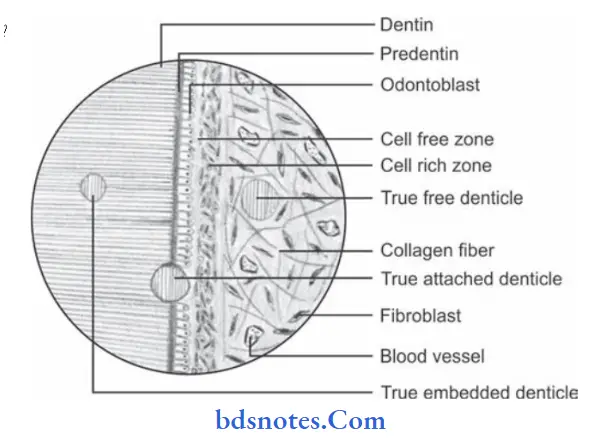
- Pulp stones are classifid according to their structures as true and false denticles.
- They are also classifid as free, attched and embedded depending on the relation to dentin.
- Pulp stones may eventually fil substantial part of pulp chamber.
Pathogenesis Of True Pulp Stone
- Development of true denticles is caused by inclusion of remnants of epithelial root sheath within pulp. These epithelial remnants induce cells of pulp to diffrentiate into odontoblasts which form dentin masses known as true pulp stone.
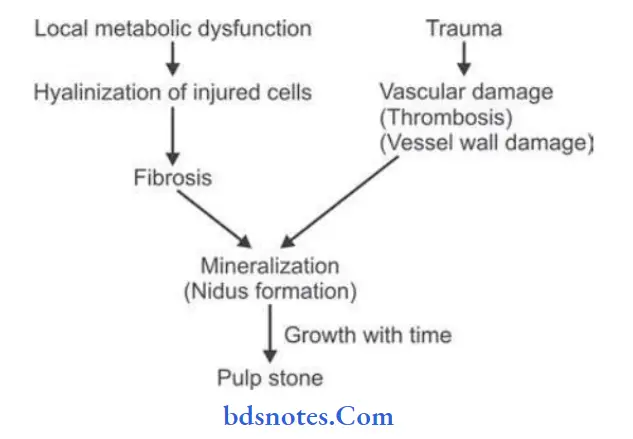
Pathogenesis Of False Pulp Stone
“Steps to explain causes of regressive alterations: Attrition vs abrasion: Q&A guide”
“Role of wear and tear in causing regressive alterations of teeth: Questions answered”
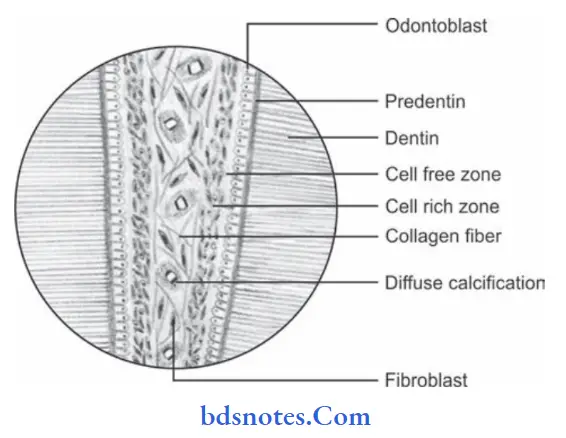
Diffuse Calcification Of Pulp
- They appear as irregular calcifi deposit in pulp tissue following collagenous firous bundles in blood vessels.
- They persists as fie calcifid spicules and sometimes develop into larger masses.
- Diffuse calcifications are found in root canal.
- Diffuse calcifications may surround the blood vessels.
- Diffse calcifiation is also termed as “calcifi degeneration.”
regressive alterations in oral pathology
“How does enamel loss lead to regressive alterations? FAQ explained”
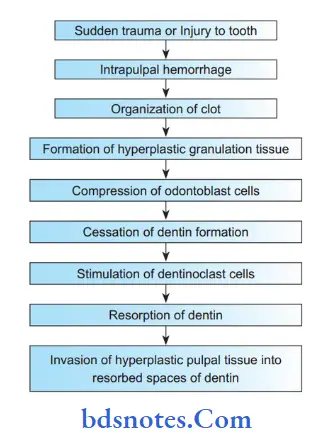
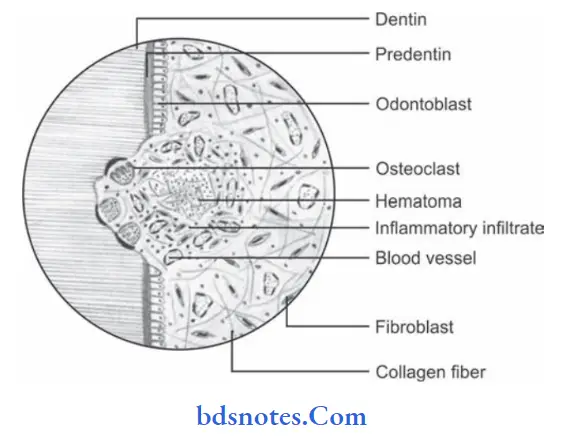
Question.4. Write short note on pink tooth.
Answer. It is also called as chronic perforating hyperplasia of the pulp or internal granuloma or odontoclastoma or pink tooth of Mummery or internal resorption of teeth.
Pathological resorption of tooth which is starting from the pulpal surface is called as internal resorption.
regressive changes of teeth BDS
Pathogenesis Of Pink Tooth.
“Early warning signs of issues addressed by understanding regressive alteration pathogenesis: Common questions”
Clinical Features Of Pink Tooth.
- Internal resorption may involve either the crown portion of the tooth or the root portion.
- Any tooth may be involved and usually only a single tooth is affected.
- Pink appearance of tooth occur in advanced stage when the coronal dentin is involved.
- When internal resorption affects the root of the tooth no color change is found
- Affected tooth remains vital unless there is pulp necrosis due to fracture of tooth or due to its perforation.
regressive alterations of teeth questions
Histopathology Of Pink Tooth.
- Multiple irregular or smooth areas of resorption in pulpal surfaces of dentin.
- A hyperplastic, highly vascular pulp tissue is projecting into the spaces of dentin which are created by resorption.
- Multiple multinucleated dentinoclasts are found near the resorpting front of the dentin.
“Asymptomatic vs symptomatic effects of ignoring regressive alterations: Q&A”
Treatment Of Pink Tooth.
- Extirpation (complete removal of part) of pulp tissue and conventional endodontic therapy
- When the tooth is perforated extraction is only the treatment.
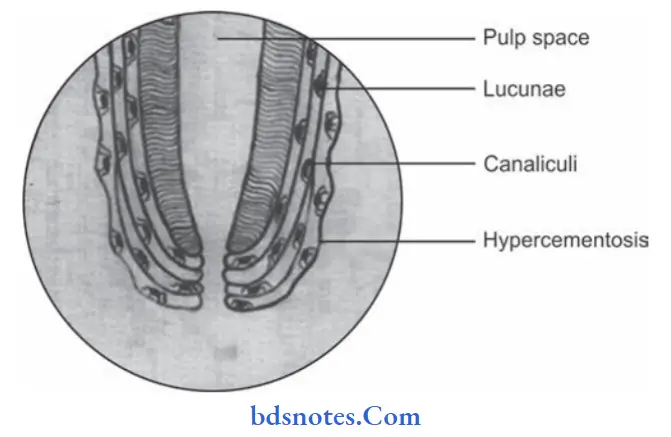
Question.5. Write notes on hypercementosis.
Or
Describe in brief hypercementosis.
Answer. Hypercementosis is also known as cementum hyperplasia.
It increases the thickness of cementum on root surfaces of the tooth due to excessive cementogenesis and is called as hypercementosis.
Etiology Of Hypercementosis
- Periapical inflammation
- Mechanical stimulation
- Functionless or unerupted tooth
- Paget’s disease of bone
- Tooth repair.
Clinical Features Of Hypercementosis
- Involved teeth are completely asymptomatic.
- There is no increase or decrease in tooth sensitivity, no sensitivity to percussion unless periapical inflammation is present.
- When the tooth with hypercementosis is extracted the roots appear larger in diameter than normal and present rounded apices.
Histological Features Of Hypercementosis
“Can targeted interventions improve outcomes using knowledge of regressive etiology? Answer provided”
- There is excessive amount of cellular cementum found deposited directly over the layer of acellular cementum.
- Area involved may be the entire root and the apical region.
- Cementum is arranged in the concentric layers around the root.
- Cementum shows numerous resting lines indicated by deeply staining hematoxyphilic line parallel to root surface.
Roentgenographic Features
Radiograph shows excessive cemental thickening with typical bulbous appearance of roots.
Treatment Of Roentgenographic Features
No treatment is indicated for teeth exhibiting hypercementosis since the condition is itself innocuous.
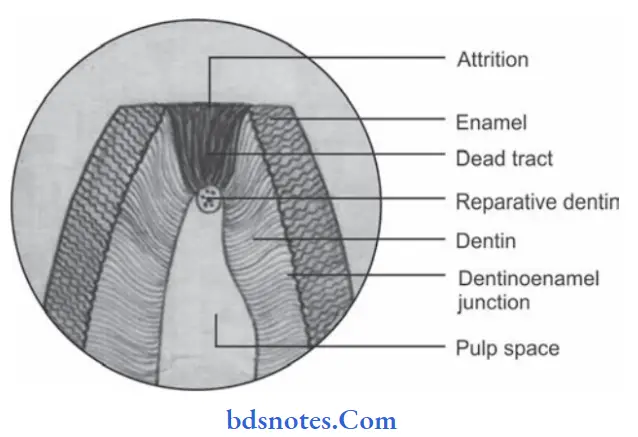
Question.6.Write short note on attrition.
Answer. Attention is a constant form of retrogressive change in teeth, characterized by the wear of tooth structure or restoration as a result of tooth to tooth contact during mastication.
Types Of Attention
- Physiological attrition: Tooth loss is proportionate to age of individual.
- Pathological attention: It occurs due to certain abnormalities in occlusion, chewing pattern or due to some structural defects.
Causes Of Attention
- Abnormal occlusion, e.g. crowding of teeth or malposed teeth.
- Abnormal chewing habit, e.g. bruxism
- Structural defects in teeth, e.g. amelogenesis imperfecta, dentinogenesis imperfecta.
Clinical Features Of Attention
- Addition of tooth is manifested by formation of well polished facete on tip of cusps, incisal edges and on proximal contact area of teeth.
- In advanced cases attrition may lead to severe reduction in cuspal height with complete wearing of enamel and flattening of occlusal surface.
- When dentin is exposed it becomes discolored brown.
- Attrition in proximal surface of teeth causes transformation of proximal contact point to relatively bordered contact areas.
- Exposure of dentinal tubules in severe cases of attention leads to hypersensitivity.
- Attrition may also lead to pulp exposure.
“Steps to educate patients about regressive alterations and their importance: Q&A format”
Treatment Of Attention
- Correction of developmental abnormalities.
- Correction of parafunctional chewing habits.
- Protection of tooth by metal or metal-ceramic crowns where structural defects are present.
Question. 7. Write short note on attrition, abrasion, abstraction and erosion.
Answer.
Abfraction
Abfraction is the loss of tooth surface at the cervical areas of teeth caused by the tensile and compressive forces during tooth flexure.
Clinical Features Of Abfraction
- Affects buccal/labial cervical areas of teeth.
- Deep, narrow Vshaped notch.
- Commonly affect single teeth with excursive interferences or eccentric occlusal loads
Erosion
It is defined as progressive loss of hard dental tissue by chemical process not involving bacterial action.
Clinical Features Of Erosion
- Broad concavities are present on tooth with smooth surface enamel.
- There is presence of cupping of occlusal surfaces with dentin exposure.
- Presence of increased incisal translucency
- Wearing away of nonoccluding surfaces.
- Amalgam restorations in erosive teeth get raised.
- Hypersensitivity is seen with the affcted tooth.
- Pulp exposure is seen in deciduous teeth.
“Role of counseling in clarifying goals for managing regressive alterations: Questions answered”
Question.8. Enumerate the diseases of cementum and describe the regressive alterations of cementum.
Answer.
Enumeration Of Diseases Of Cementum
Based on clinical radiographic and histological features boney lesions of cementum were classifid by Pindborg et al (1971).
- Periapical cemental dysplasia (Cementoma)
- Benign cementoblastoma
- Cementifying firoma
- Gigantiform cementoma
- Cementoosseous dysplasia
Regressive Alterations Of Cementum
- With aging, surface of cementum become more irregular.
- As thickness of cementum increases due to hypercementosis permeability of cementum decreases.
- Under light microscope only the surface layer of cementocytes appear viable. All other lacunae become empty.
- Greater amount of cementum appear in apical zone, middle third of the root and furcation areas.
- With age as a result of functional inflences on teeth the location and shape of apical foramina undergo changes.
- Due to aging cementum can resorb or deposit creating reversal lines.
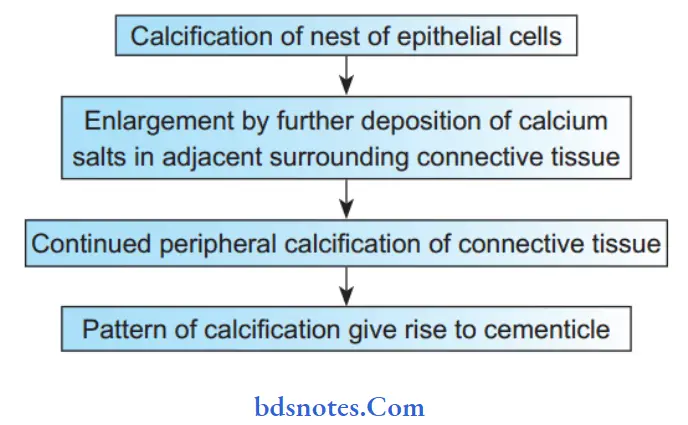
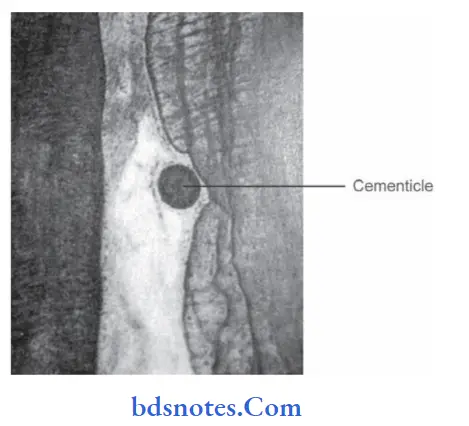
- Cementicles: Calcifying spherical bodies composed of cementum either lying free within PDL, attached to cementum or within it. They are mostly 0.5 mm in size. They usually are ovoid or round with similar appearance to denticles and are classifid as free, attched or embedded. Cementicles are a response to either local trauma or hyperactivity and appears in increasing numbers in an aging person. Found in 35% of human roots.
Pathogenesis Or Formation Of Cementicles
“How do educational materials explain complex regressive alteration concepts? FAQ explained”
Question.9.Defie attrition, abrasion and erosion.
Answer. Attition: Attition is defined as physiologic wearing away of a tooth as a result of tooth to tooth contact as in mastication.
Abrasion: Abrasion is the pathologic wearing away of tooth substance through some abnormal mechanical process.
Erosion: Erosion is defined as irreversible loss of dental hard tissue by a chemical process that does not involve bacteria.
“Early warning signs of knowledge gaps in patient understanding of regressive alterations: Common questions”
Question.10. Write short note on abstraction.
Answer. Abfraction is defied as the loss of tooth surface at the cervical areas of teeth caused by tensile and compressive forces during tooth flxure.
Abfraction Pathogenesis
When occlusal forces are applied eccentrically to a tooth the tensile stress is concentrated at cervical fulcrum which causes flxure that leads to disruption in the chemical bonds of enamel crystals in cervical areas. Once damaged, cracked enamel can be lost or more easily removed by erosion or abrasion.
Abfraction Etiology
- Static forces: These forces are produced during swallowing,clenching and tongue thrusting.
- Cyclic forces: These forces are produced at the time of chewing.
- People with open bite or deep class I cavity are prone for abfraction.
Clinical Features Of Abfraction
- It can occur at any age.
- It affects buccal or labial cervical third or gingival third area of teeth.
- Most commonly affected teeth are facial surfaces of bicuspids and molars.
- There is presence of a narrow Vshaped notch.
- Single tooth is affected most commonly with excessive interferences or eccentric occlusal loads.
- Tooth becomes hypersensitive and there is wearing of occlusal surface.
- Since lateral forces damage the cervical area of tooth, repeated restoration failures are appreciated.
Treatment For Abfraction
- Etiological agent should be removed.
- Progression of the problem is stopped by bite guard.
- Areas of Vshaped notching should be restored by tooth colored restorative material.
“Can interactive tools improve adherence to regressive alteration care protocols? FAQs provided”
Question.11. Write short note on erosion.
Answer. Erosion is defined as progressive loss of hard dental tissue by chemical process not involving bacterial action.
Erosion Etiology
Dissolution of mineralized part of tooth occurs due to intrinsic causes and extrinsic causes.
Extrinsic causes are acidic beverages and citrus fruits.
Intrinsic causes are gastroesophageal reflx and vomiting
Extrinsic Causes Of Erosion
- It consists of acidic foods or due to iatrogenic exposure.
- Extrinsic causes consist of acidic beverages and foods,dietary acids, medication, environmental acids, sport drink, fruit juices, etc.
- Erosion is commonly seen in professional swimmers and occupational wine tasters.
Intrinsic Causes Of Erosion
- Gastric acids which regurgitate in esophagus and mouth because of acid reflux or due to excessive vomiting.
- Anorexia bulimia can also cause erosion of teeth, mostly the palatal surfaces of maxillary anterior teeth are involved.
Clinical Features Of Erosion
- Broad concavities are present on tooth with smooth surface enamel.
- There is presence of cupping of occlusal surfaces with dentin exposure.
- Presence of increased incisal translucency
- Wearing away of non-occluding surfaces.
- Amalgam restorations in erosive teeth get raised.
- Hypersensitivity is seen with the affected tooth.
- Pulp exposure is seen in deciduous teeth.
Treatment Of Erosion
- Proper etiology should be ruled out.
- Cases of acid reflux should be sent to physician for proper treatment.
- In cases with hyposalivation chewing gums are used to enhance the salivary flow.
Question.12. Write short note on pulp stones.
Answer. Pulp stones are nodular calcified masses appearing on coronal portions of the pulp organs.
- They are asymptomatic unless they impinge nerves on blood vessels.
- Pulp stones are classified according to their structures as true and false denticles.
- They are also classified as free, attached, and embedded depending on the relation to dentin.
- Pulp stones develop around central nidus of pulp tissue
- Pulp stones may eventually fill substantial part of pulp chamber.
- Pulp stones may arise as a part of agerelated changes or local pathologic changes.
Pathogenesis Of True Pulp Stone
- Development of true denticles is caused by inclusion of remnants of epithelial root sheath within pulp. These epithelial remnants induce cells of pulp to differentiate into odontoblasts which form dentin masses known as true pulp stone.
Pathogenesis Of False Pulp Stone
“Asymptomatic vs symptomatic effects of poor communication about regressive alterations: Answered”
Histopathology Of Pulp Stones
- Pulp stones show central amorphous mass of irregular calcifiation which is surrounded by concentric lamellar rings of regular calcifid material.
- Occasionally peripheral layer of tubular dentin is applied by odontoblasts which arise from surrounding pulp tissue in response to pulp stone present.
- Fibrillar irregular calcified material can also be seen on periphery of pulp stone.
Clinical Significance Of Pulp Stones
- Pulp stones are cause of pain, varying from mild pulp neuralgia to severe excruciating pain resembling of trigeminal neuralgia.
- Difficulty is encountered in extirpating the pulp during root canal therapy if pulp stones are present.
Treatment For Pulp Stones
No treatment is required.
Question.13.Write short note on pulp calcification.
Answer. Pulp calcifications are of three types, i.e. denticles, pulp stones and diffuse calcifications.
All of the pulp calcifications start as free bodies in pulp tissue but many of them get attched or embedded in dentinal walls of the pulp.
Pulp Calcifications Denticles
- They occur due to the epitheliomesenchymal interaction inside the developing pulp.
- Epithelial strands which originate from the root sheath or cervical extensions in pulp chamber adjacent to furcation, induce differentiation of osteoblasts of surrounding mesenchyme of dental papilla forming the core of denticle
- Odontoblasts deposit tubular dentin as they migrate away from central epithelium and produce thimbleshaped structures which surround the epithelium.
- Denticles are formed at the time of root development and occur in root canal and pulp chamber adjacent to furcation areas of multirooted teeth.
- Most of the denticles remain attach or embedded in dentin.
Histopathology
- Denticles consist of tubular dentin which surround central nest of epithelium. As time progresses this central epithelium degenerates and tubules undergo sclerosis making their detection difficult.
- Mainly denticles are free or embedded but those remain free in pulp at times develop outer layers of irregular fibrillar calcification or lamellated layers of calcification.
Pulp Stones
- Pulp stones are nodular calcifid masses appearing on coronal portions of the pulp organs.
- They are asymptomatic unless they impinge nerves on blood vessels.
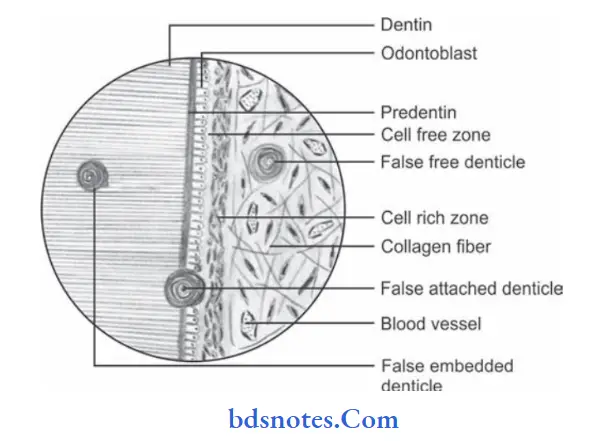
- Pulp stones are classified according to their structures as true and false denticles.
- They are also classified as free, attached and embedded depending on the relation to dentin.
- Pulp stones develop around central nidus of pulp tissue
- Pulp stones may eventually fil substantial part of pulp chamber.
- Pulp stones may arise as a part of age related changes or local pathologic changes.
Histopathology Of Pulp Stones
- Pulp stones show central amorphous mass of irregular calcifiation which is surrounded by concentric lamellar rings of regular calcifid material.
- Occasionally peripheral layer of tubular dentin is applied by odontoblasts which arise from surrounding pulp tissue in response to pulp stone present.
- Fibrillar irregular calcifid material can also be seen on periphery of pulp stone.
Diffuse Calcifiations
- Diffse calcifiation is also termed as “calcifi degeneration.”
- They are areas of fie, firillar, irregular calcification which are parallel to vasculature.
- They persist as fie calcifid spicules and sometimes develop into larger masses.
Diffuse calcifications are found in pulp chamber or root canal. - Diffuse calcifications may surround the blood vessels.
Histopathology
Its pattern is amorphous, unorganized linear strands or columns paralleling blood vessels and nerves of pulp.
Clinical Signifiance of Pulp Calcifiations
- Pulp stones are cause of pain, varying from mild pulp neuralgia to severe excruciating pain resembling of trigeminal neuralgia.
- Difficulty is encountered in extirpating the pulp during root canal therapy if pulp stones are present.
- Pulp calcifications can also interfere with formation of root causing early periodontal destruction and tooth loss.
- Prominent pulp calcifiations are associated with some diseases such as dentin dysplasia, pulp dysplasia, Calcinosis universalis and Ehlers-Danlos syndrome.
Treatment of Pulp Calcifications
No treatment is required.
Leave a Reply