Pectoral Region And Axilla Notes
Question 1. What is a breast? Describe its structure in brief.
Answer.
The breast is a modified sweat gland (apocrine type). It is rudimentary in male and well developed in female at puberty. In adult female, it is seen as a soft hemispherical protruding organ one on either side in the pectoral region.
Breast Structure
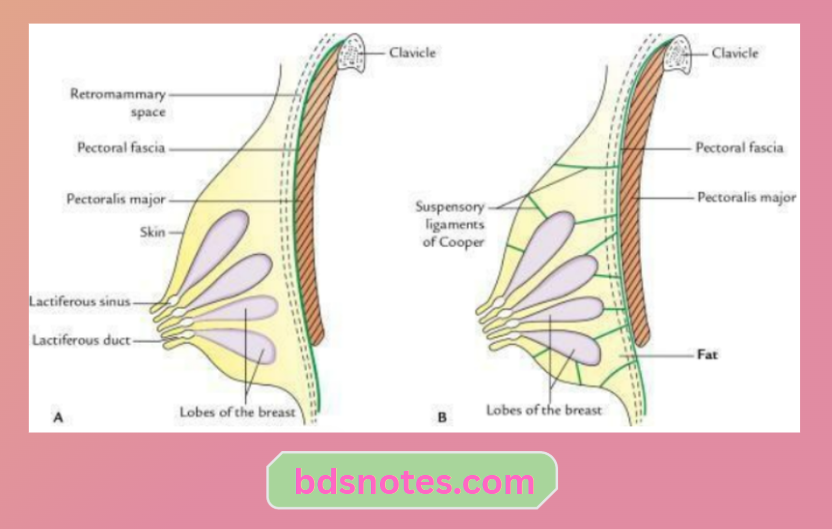
The breast is composed of three components: skin, parenchyma and fibrofatty stroma.
Pectoral Region and Axilla Anatomy
“Understanding the anatomy of the pectoral region and axilla”
“Importance of studying the pectoral region and axilla for healthcare professionals”
Skin:
It presents nipple and areola.
- Nipple: It is a dark conical projection of skin in the centre of the breast. It is pierced by 10–15 lactiferous ducts and contains smooth muscle fibres.
- Areola: It is a circular, blackish discolouration around the nipple. It contains numerous modified sebaceous glands. They secrete an oily secretion which lubricates and prevents the nipple from drying and cracking.
Anatomy of Pectoral Region and Axilla
Parenchyma:
It consists of a glandular part made up of alveoli, lactiferous ducts and lactiferous sinuses.
“Common challenges in diagnosing axillary and pectoral injuries”
“Signs of poor pectoral muscle function in daily activities”
Fibrofatty stroma:
It consists of fibrofatty tissue.
- Fibrous stroma consists of fibrous septa (ligaments of Cooper), which extend from skin to the pectoral fascia and divide the gland into 10–15 lobes.
- Fatty stroma lies between fibrous septa and the aural part.
Venous drainage
The main veins draining the area around the areola and parenchyma (glandular tissue) are deep. They form the circular venous plexus at the base of the gland. From here, they drain into:
- Axillary vein
- Internal mammary vein
- Intercostal veins
Lymphatic drainage
The lymph vessels draining the breast are divided into two sets: (a) A set draining the parenchyma, nipple and areola; (b) A set draining overlying skin, excluding nipple and areola.
“Role of the pectoralis major in shoulder movement”
“Biomechanics of pectoral muscle contractions explained”
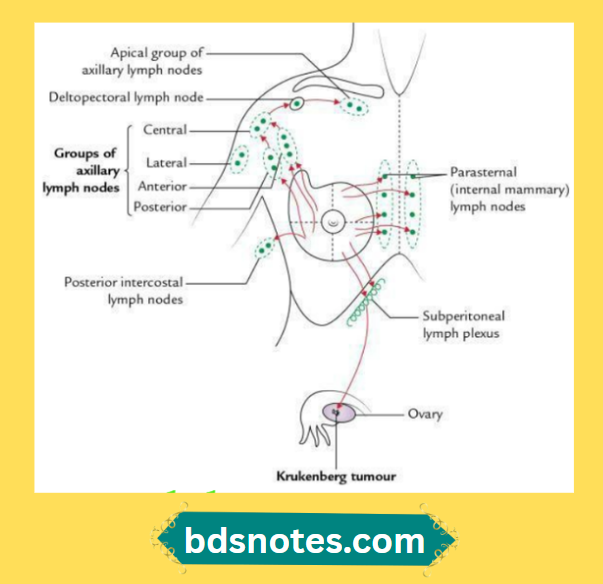
- Those draining the parenchyma, including areola and nipple, form the subareolar plexus of Sappey, which drains as follows:
- Seventy-five per cent (75%) of an axillary group of lymph nodes chiefly into the anterior (or pectoral) group. Some reach the posterior (subscapular) group. Efferents from these pass to the central and thence into the apical group.
- Twenty per cent (20%) drain into parasternal (internal mammary) nodes.
- Five per cent (5%) drain into the posterior intercostal nodes.
- Those draining the overlying skin, excluding the areola and nipple, drain into:
- Axillary nodes – from the outer part
- Supraclavicular nodes – from the upper part
- Parasternal nodes – from the inner part
- Subdiaphragmatic nodes – from the inner part
Read And Learn More: Selective Anatomy Notes And Questions And Answers
“Techniques for managing high-risk groups with injuries”
Female Breast Applied Anatomy
Carcinoma of the breast:
The breast is a common site of carcinoma. The important points to know about breast carcinoma are
- The cancer cells may infiltrate the suspensory ligaments (Cooper’s ligaments) and, as a result, the breast becomes fixed and immobile.
- The contraction of the ligaments causes retraction or puckering of the skin.
- The infiltration of the lactiferous duct and its consequent fibrosis leads to retraction of the nipple.
- Secondary breast cancer is usually lodged in the liver, ovaries or the peritoneum, making the prognosis worse.
“Complications of delaying treatment for pectoral and axillary issues”
- The cancer cells may migrate transcellomically to the ovary, producing a secondary tumour called Krukenberg tumour.
- The cancer cells can also spread to the vertebrae and the brain via venous route, through the communication between the veins draining the breast and the vertebral venous plexus.
- Peau d’orange: In breast cancer, the skin over the breast presents an orange peel appearance. This occurs due to obstruction of cutaneous lymphatics, leading to breast oedema and deepening of the mouths of sweat glands and hair follicles.
Leave a Reply