Multiple Myeloma
Multiple myeloma is a relatively uncommon malignancy of plasma cell origin which often has multicentric origin within the bone.
Multiple Myeloma Pathogenesis
Mutation of terminally differentiated B cells or early committd B cells lead to more differentiated plasma cells.
Abnormal plasma cells probably arising from single malignant precursor which had undergone uncontrolled mitotic division and spreads throughout the body.
Since the neoplasm develops from the single cell, all daughter cells which comprises of the lesional tissue have same genetic makeup and produce same proteins.
multiple myeloma
“Importance Of Early Detection Of Multiple Myeloma”
Multiple Myeloma Clinical Features
- It occurs between 40 to 70 years of age.
- Male to female ratio is 4:1.
- Bone pain is present particularly in the lumbar spine.
- Pathological fractures are also present.
- Petechial hemorrhages of skin can be seen.
- Swelling over the areas of bony involvement can be seen.
- Metastatic calcifiation may involve the soft tissue and is due to hypercalcemia secondary to tumor related osteolysis.
- Amyloid deposits occur at periorbital region appearing waxy, fim, plaque like lesions.
- Death occurs due to renal failure as there is accumulation of abnormal proteins in renal tissue.
“Difference Between Multiple Myeloma And Other Cancers”
Multiple Myeloma Oral Manifestations
- Mandible is commonly involved as compared to maxilla.
Angle of mandible is commonly involved. - Patient complaints of pain, numbness and swelling of jaw.
- Intraoral swelling is present which tends to be ulcerated,rounded and bluish red.
- Tongue may show diffuse enlargement and firmness or may have nodular appearance. Sometimes nodules are ulcerated.
multiple myeloma treatment
Multiple Myeloma Radiographic Features
Presence of multiple well defied, punched out radiolucency or ragged radiolucent lesions. This is evident on skull radiograph.
Multiple Myeloma Laboratory Investigations
- Urinary examination: Light chain products found in urine of 30 to 50% of multiple myeloma patients are known as Bence Jones proteins.
- On serum protein electrophoresis most patients suffering from multiple myeloma have decreased quantity of normal immunoglobulin and an abnormal monoclonal immunoglobulin protein peak, known as M spike. The immunoglobulin is usually of IgG or IgA class with monoclonal light chain component.
- Alkaline phosphatase levels are raised.
“Understanding The Role Of Plasma Cells In Multiple Myeloma”
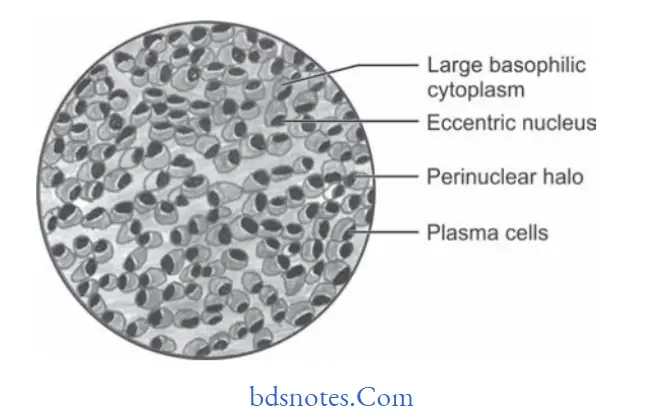
Multiple Myeloma Histopathology
- There is presence of sheets of closely packed cells resembling plasma cells. Cells are round to oval in shape with eccentrically placed nucleus exhibiting chromatin clumping in cartwheel or checkerboard pattrn.
- Perinuclear halo can also be seen.
- Russell bodies are seen in chronic inflmmatory lesions with numerous typical plasma cells.
- Mitotic activity can be seen along with some frequency.
- If amyloid is present, it appears as homogenous, eosinophilic and relatively acellular.
“The Role Of Imaging In Diagnosing Multiple Myeloma Accurately”
“Step-By-Step Guide To Diagnosing Multiple Myeloma Effectively”
Multiple Myeloma Treatment
- Multiple myeloma is treated by chemotherapeutic agents such as melphalan and cyclophosphamide along with prednisolone.
- Oral bicarbonates, high flid intake and corticosteroid decreases calcium levels.
- Local radiation therapy decreases painful bony lesions.
Leave a Reply