Mucogingival Surgery Periodontal Plastic Surgery
Write short note on gingival recession.
Or
Write short note on etiology of gingival recession and its classification.
Answer. Gingival recession is defined as “exposure of the root surface due to apical shift in marginal gingiva”. Grant
Type
There are two types of recession
- Visible-clinically observable.
- Hidden-covered by gingiva.
“Understanding the role of mucogingival surgery in gum health”

“Importance of studying mucogingival surgery for dental professionals”
Gingival Recession Classification
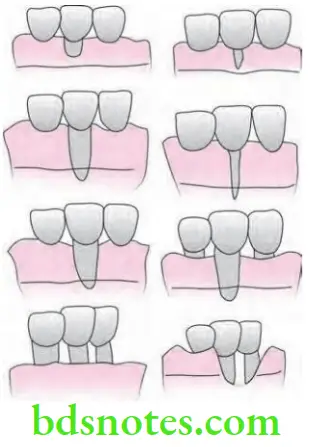
According to Sullivan and Atkins
- Shallow-narrow
- Shallow-wide
- Deep-narrow
- Deep-wide.
“Common challenges in performing mucogingival surgery in periodontics”
Read And Learn More: Periodontics Question And Answers
According to PD Miller’s
“Steps to identify when mucogingival surgery is necessary in periodontics”
- Class 1: Marginal tissue recession that does not extend to the mucogingival junction. There is no loss of bone or soft tissue in the interdental area.
- Class 2: Marginal tissue recession that extends to or beyond the mucogingival junction. There is no loss of bone or soft tissue in the interdental area.
- Class 3: Marginal tissue recession that extends to or beyond the mucogingival junction.
- In addition there is loss of bone and/or soft tissue in the interdental area or there is malpositioning of tooth.
- Class 4: Marginal tissue recession that extends to or beyond the mucogingival junction with severe loss of bone and soft tissue interdentally and/or severe malpositioning of the tooth.
“Role of gingival recession in recommending mucogingival surgery”
Etiology of Gingival Recession
- Inflammatory factors
- Plaque induced inflammatory periodontal diseases, toothbrush injury, etc.
- Anatomic factors
- Developmental anatomic abnormalities (dehiscence, thin body plates, high frenum attachment), malocclusion.
- Iatrogenic factors
- Deleterious habits (Pressure of foreign objects like finger nails, pencils, and hairpins)
- Claps and mandible oral denture bars.
- Prolonged orthodontic treatment.
“Early warning signs of untreated mucogingival issues in periodontics”
Gingival Recession Clinical Significance
- Exposed root surface are susceptible to caries.
- Wearing away of cementum exposed by recession leaves an underlying dentinal hyperemia of the pulp and associated symptoms.
- In interproximal recession plaque and food debris can accumulated.
“Asymptomatic vs symptomatic stages of soft tissue damage”
Gingival Recession Treatment
Various techniques are used to increase the width of attached gingiva:
- Gingival augmentation apical to area of recession
- Free epithelial autograft
- Free connective tissue autograft
- Apically positioned flap
- Fenestration
- Vestibular extension
“Pathophysiology of untreated mucogingival issues in periodontics explained”
- Gingival augmentation coronal to recession or root coverage
- Free epithelial autograft
- Free connective tissue autograft
- Pedicle autografts
- Rotational, i.e. Lateral pedicle flap and double papilla flap
- Advanced, i.e. coronally displaced flap and semilunar flap
“Emerging research on advanced mucogingival techniques in periodontics”
- Subepithelial connective tissue graft
- Subpedicle connective tissue
- Pouch and tunnel technique
- Envelope technique
- Guided tissue regeneration technique.
Leave a Reply