Modified Widman Flap
Periodontal flap is a section of gingiva and/or mucosa surgically elevated from underlying tissues to provide visibility and access to bone and root surface.
“How To Live A Healthier Life With Proper Modified Widman Flap Care”

“What Is A Modified Widman Flap Procedure”
Modified Widman Flap
It is presented in 1974 by Ramfjord and Nissle.
- Step 1: It is an initial, internal bevel incision 0.5 to 1 mm away from gingival margin, directed to alveolar crest. Vertical releasing incisions are not required.
- Step 2: Gingiva is reflected with periosteal elevator.
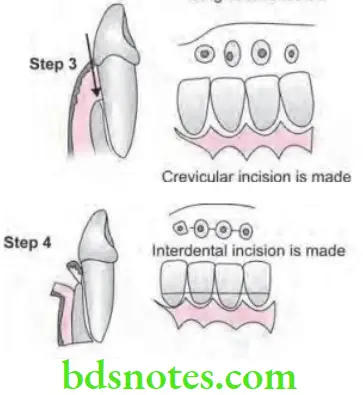
- Step 3: A crevicular incision is made from bottom of the pocket to the bone, circumscribing the triangular wedge of tissue containing pocket lining.
- Step 4: After flap is reflected, third incision is made in interdental space with Orban’s knife and gingival collar is removed.
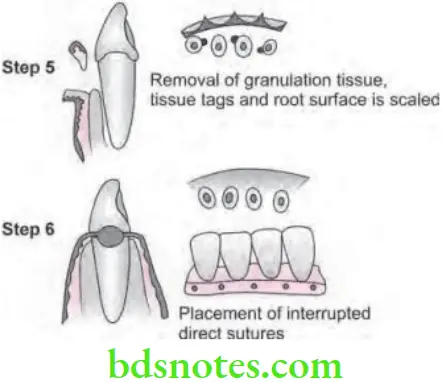
- Step 5: Tissue tags and granulation tissue are removed with a curette. The root surfaces are checked and scaled.
“Best Practices For Maintaining Gum Health After A Modified Widman Flap Procedure”
- Step 6: Bone architecture is not corrected, good approximation of flaps is necessary. Every effort is made to adapt the facial and lingual interproximal tissue adjacent to each other in such a way that no interproximal bone remain exposed at the time of suturing.
- Step 7: Interrupted direct sutures are placed in each inter dental space and covered with tetracycline ointment and with a periodontal surgical pack
“Purpose Of The Modified Widman Flap In Dentistry”
Healing After Flap Surgery
- Immediately after suturing (0 to 24 hours), connection between the flap and the tooth or bone surface is established by the blood clot, which consists of a fibrin reticulum with many polymorphonuclear leukocytes, erythrocytes, debris from injured cells and capillaries at the edge of the wound. There are also bacteria and an exudate or transudate as a result of tissue injury.
- One to three days after flap surgery: Space between the flap and the tooth or the bone is thinner and epithelial cells migrate over the border of the flap, when the flap is closely adapted to the alveolar process there is only a minimal inflammatory response.
“The Role Of The Modified Widman Flap In Reducing Periodontal Pockets”
- One week after flap surgery: Epithelial attachment to the root has been established by means of hemidesmosomes and a basal lamina. The blood clot is replaced by granulation tissue derived from gingival connective tissue, bone marrow and the periodontal ligament.
- Two weeks after surgery: Collagen fibers begin to appear parallel to the tooth surface. Union of the flap and the tooth is still weak (due to immature collagen fibers) but clinically it appears almost normal.
- One month after surgery: A fully epithelialized gingival crevice with a well defined epithelial attachment is present. Supracrestal fibers begin to adapt a functional arrangement.
Leave a Reply