Malignant Tumours Notes
Types Of Malignant Tumours
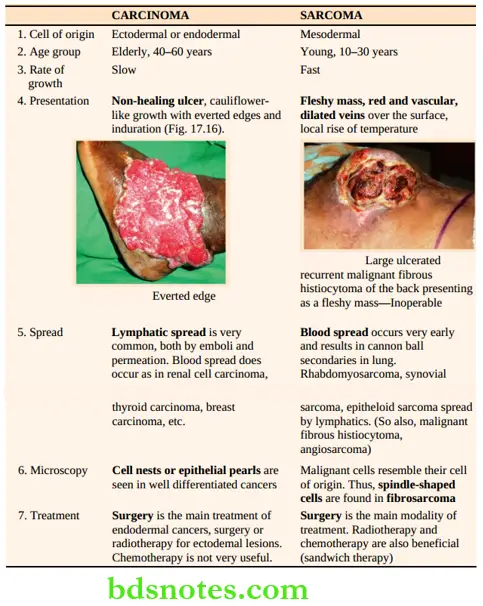
- They are of two types; carcinoma and sarcoma. Carcinoma arises from epithelium — ectodermal, endodermal or mesodermal in origin.
- Sarcomas arise from soft tissues or bone, which are derived from mesoblast or mesenchymal tissues.
- It can be observed that mesoderm can give rise to carcinoma and mesenchymal sarcoma also.
Pathology Spread
- Local spread: Generally occurs in adjacent structures.
A few examples are given:- Carcinoma cheek — fixity to the mandible. Significance: May necessitate removal of mandible along with wide excision.
- Squamous cell carcinoma — fixed to tibia may necessitate an amputation.
- Lymphatic spread: It is one of the most important features of carcinoma. As you complete reading this book, you will come across many cases and many examples of the lymphatic spread of malignant tumours. A few sarcomas are also spread by lymphatics.
Different types of lymphatic spread are given below.
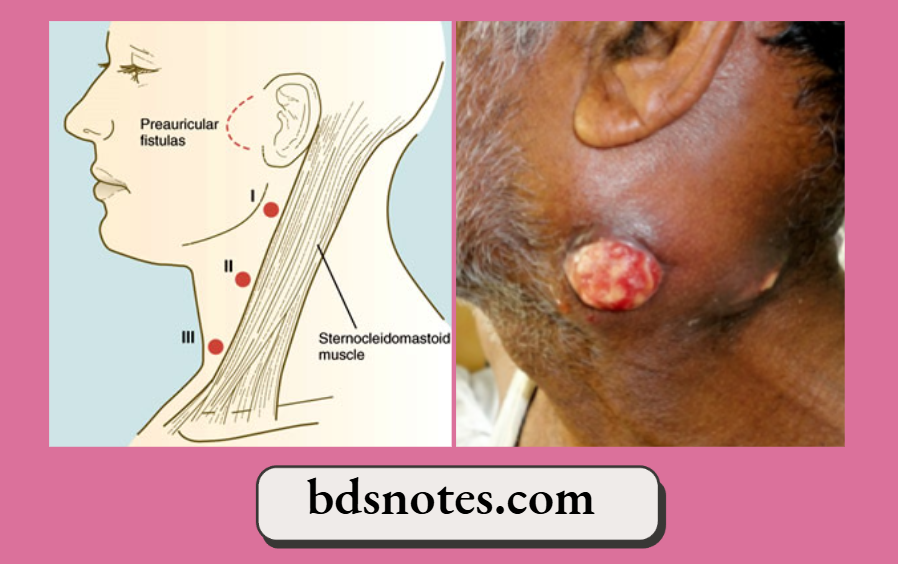
- Permeation: Refers to tumour cells travelling along the lymphatic vessel, for example, Carcinoma tongue with submandibular node enlargement
- Lymph nodes in the neck/groin may infiltrate the skin in advanced cases.
- Embolisation: A more aggressive tumour means more aggressive spread — by embolisation wherein nodes can be enlarged in a faraway station, for example, malignant melanoma.
Read And Learn More: Clinical Medicine And Surgery Notes
Carcinoma
Carcinoma Origin
- Ectodermal—Skin cancer
- Endodermal—Gut cancer
- Mesodermal—Renal carcinoma
CarcinomaTypes
- Squamous cell carcinoma
- Basal cell carcinoma
- Glandular
- Retrograde lymphatic spread: When the main lymphatic pathway is blocked, retrograde spread can occur and a node in an unusual location may get enlarged, e.g. Irish node (left axillary node enlargement in carcinoma of the stomach).
3. Haematogenous spread: This is the most important method of spreading sarcomas. A few malignancies, such as renal cell carcinoma, follicular carcinoma thyroid, carcinoma prostate, carcinoma breast, and malignant melanoma, are also commonly spread by blood.
- Bony metastasis and lung metastasis result from blood spread. Bone metastasis can be mild form such as bony pains to severe form such as quadriplegia/ pathological fracture, etc.
4. Seeding
- Cancer of the lower lip spreads to the upper lip. Also called kiss cancer. Another example: is cancer of the vulva.
- Incision and ‘port’ site metastasis — (port refers to laparoscopic port)
5. Transcoelomic spread: Spread through the peritoneal cavity by dislodgement of malignant cells, for example. Ca stomach with Krukenberg tumour — bilateral bulky ovarian metastasis, commonly seen in pre-menopausal patients.
Aetiology Of Carcinoma In General
1. Tobacco is the most important factor in the development of lung cancer, upper respiratory tract cancer, gastrointestinal tract and genitourinary tract cancer. Carcinoma pancreas is found more commonly in smokers. Passive smokers also have an increased incidence of the development of cancers.
2. Alcohol: Smoking with alcohol increases the permeability of the upper digestive tract mucosa and respiratory mucosa to the carcinogens. Thus, they increase the incidence of cancer. Hepatocellular cancer is commonly found in alcoholic cirrhotic liver.
3. Ionising radiation: Atomic bomb blasts in Japan have definitely resulted in an increased number of cases of breast cancer in premenopausal women and leukaemia in children.
4. Ultraviolet radiation: Causes all types of skin cancers.
5. Genetic causes:
6. Hereditary causes
- MEN syndrome: Medullary carcinoma thyroid. (Multiple Endocrine Neoplasia)
- FPC: Colonic cancer (Multiple) (Familial Polyposis Coli)
- Li-Fraumeni syndrome — Familial breast cancer.
- Retinoblastoma.
7. Dietary factors
- Red meat: Carcinoma colon, carcinoma breast.
- Fat: Carcinoma breast, carcinoma colon.
- Smoked, charred fish: Carcinoma oesophagus, carcinoma stomach.
Genetic/Defective DNA Repair
- Xeroderma pigmentosa
- Skin cancer
- Bloom’s syndrome – Acute leukaemia, various cancers
- Fanconi’s anaemia – Acute leukaemia, squamous cell carcinoma, hepatoma
- Ataxia telangiectasia – Acute leukaemia, lymphoma, breast cancer
8. Chemicals
- Benzanthracenes — Skin cancer when painted on the skin
- Benzopyrenes — Lung cancer
- β-naphthylamine — Bladder cancer
- Nitrosamines and amides — Cancer stomach
- Anatoxin B — Hepatocellular carcinoma
- Asbestos — Lung cancer.
9. Viral factors
- Human T-cell leukaemia virus type 1 (HTLV-1) — T-cell leukaemia/lymphoma. (RNA virus)
- Human papillomavirus (HPV) Cancer cervix, cancer urogenital region
- Epstein-Barr virus — Burkitt’s lymphoma.
Soft Tissue Sarcomas
These are the malignant tumours arising from soft tissues. Thus they can occur in any part of the body. Examples are given.
Soft Tissue Sarcomas Introduction
- These are malignant tumours which are fatal if untreated or mistreated.
- Most of them occur in young patients as painless lumps
- CT scan, MRI, and incision biopsy (details later) are the key investigations.
- Early diagnosis and curative resection have a major role in the management of soft tissue sarcomas.
- Staging: In addition to the TNM staging, pathological grading of the tumour has been included — GTNM staging.
Aetiology Of Sarcoma
- Lymphangiosarcoma can develop from post-mastectomy lymphoedema of the upper limb, a few years later. This is called Stewart-Treves syndrome. It can occur in any chronic lymphoedematous tissue.
- Angiosarcoma and other soft tissue sarcomas: Polyvinyl chloride, thorium dioxide, arsenic, etc.
- Osteogenic sarcoma: Paget’s disease of the bone, exposure to radium (Watch dials).
- Fibrosarcoma: Paget’s disease of the bone, post-irradiation.
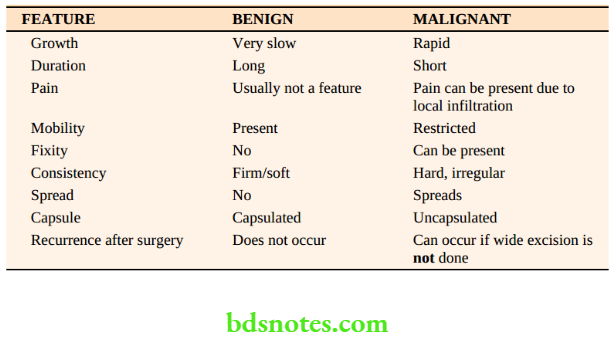
- Kaposi’s sarcoma: Cytomegalovirus and human immunodeficiency virus (HIV). (See Table 17.6 for a comparison of carcinoma with sarcoma).
Soft Tissue Sarcomas Types Of Biopsy
- FNAC — Grading not possible
- Core biopsy — Grading may be difficult
- Incision biopsy — Adequate sample
- Excision biopsy — The Best.
Soft Tissue Sarcomas Clinical Features
Staging Of Soft Tissue Sarcoma
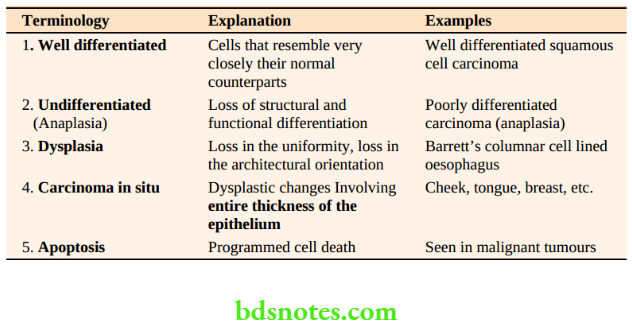
- Grade (G)
- G1 — Well differentiated
- G2—Moderately differentiated
- G3 — Poorly differentiated
- G4 — Undifferentiated
- Primary tumour (T)
- T1 Tumour ≤ 4–5 cm in greatest dimension
- T2 Tumour ≥ 5 cm in greatest dimension
- Regional lymph nodes (N)
- N0 : No nodal metastasis
- N1: Regional lymph node metastasis present.
- Distant metastasis (M)
- M0: No distant metastasis
- M1: Distant metastasis present.

G—Tnm Staging System
Stage Grouping
- 1 G1 T1−T2 N0 M0
- 2 G2 T1−T2 N0 M0
- 3 G3 T1−T2 N0 M0
- 4 G1−G3 T1−T2 N1 M0
- G1−G3 T1−T2 N1 M1
Soft Tissue Sarcomas Treatment
- The aim is to achieve local control and to treat metastasis including subclinical metastasis.
- Surgery is the first line of treatment, varying from a wide excision to amputation or disarticulation when it occurs in the extremities.
- Tumours do respond to radiotherapy and chemotherapy.
- If amputation can be avoided by giving preoperative radiotherapy, it is preferred first, followed by the wide excision/ compartmental excision followed by postoperative RT.
- Low-grade tumours can be treated on a 1 cm wide excision with a 1 cm margin and high-grade tumours by a 4 cm margin.
Role Of Chemotherapy
- The high-grade tumours have a high potential for metastasis. Hence, combination chemotherapy is to be considered before or after surgery.
- The most favoured combination chemotherapy drugs include – Mesna, Adriamycin, Ifosfamide and Dacarbazine (MAID)
- The success rate is around 10–20%.
Differential Diagnosis Of Soft Tissue Sarcoma Liposarcoma
- It is a malignant fatty tumour.
- Common sites: Proximal extremity, trunk or retroperitoneum.
- They are generally large at the time of diagnosis, for example. retroperitoneum. It results in gross swelling, which is firm to hard.
- The compression of blood vessels may result in oedema of the limbs when it occurs in the retroperitoneum.
- Well-differentiated myxoid liposarcomas are notorious for recurring many times before spreading to the lungs. Hence, the prognosis is good.
- Pleomorphic and lipoblastic liposarcomas tend to be of higher grade and often present with metastasis.
- They do respond well to radiotherapy.
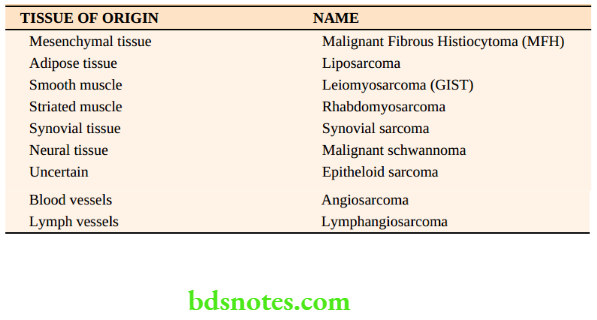
Malignant Fibrous Histiocytoma (MFH)
- Malignant tumour of mesenchymal tissue (fibrous tissue). This is the recent nomenclature of sarcoma. Fibrosarcoma or pleomorphic rhabdomyosarcomas are included under this.
- These are high-grade tumours which lack differentiation.
- It can also arise from the bone
- Most of the so-called fibrosarcomas are presently included under MFH.
- The MFH —Superficial type rarely metastasises and carries a good prognosis.
- Locations: Retroperitoneum, trunks and limbs (intermuscular septae of adductors, scapulohumeral and pectoral muscles).

Malignant Fibrous Histiocytoma Clinical features
- Common in elderly patients (50 years) but can occur at any age.
- Slow-growing firm to hard mass with restricted mobility.
- Common locations (as mentioned above)
- As the tumour is locally invasive, it infiltrates the muscles and adjacent structures and thus can cause muscle weakness or pain, etc.
- Spread: Local spread is common. Distant metastasis by blood is late (lungs). Lymph node metastasis is rare.
- Like other sarcomas, dilated veins, the local rise of temperature, restricted mobility and hardness will clinch the diagnosis.
Synovial Sarcoma
- Any rapidly growing tumour in the region of the joint/or near the tendons in young patients (20– 40 years), synovial sarcoma is to be considered.
- Common site: Shoulder, wrist, knee, etc.
- Age: Young between 20 and 40 years.
- Clinical features are similar to the other sarcomas—hard, painful mass.
- In addition to the local and blood spread, it also spreads by the lymphatic route.
- Plain X-ray: May show characteristic calcification
- It is aggressive, with high rates of recurrence.
- In the G-TNM staging system, they are grade 3.
Angiosarcoma
- 1 to 2% of soft tissue sarcomas.
- Affects elderly patients
- They are high-grade and aggressive tumours.
- They arise from skin and subcutaneous tissue rather than deeper tissues.
- Most of them occur in the head and neck, breast and liver.
- Surgery (excision) followed by radiotherapy/ combination chemotherapy may have to be given.

Rhabdomyosarcoma
- The most common soft tissue sarcoma is seen in children, even though they are rare.
- It arises from striated muscle.
- Resection/Chemotherapy/Radiotherapy (combination) is tried depending on location.
- Sites: Head and neck 70%, genitalia (15–20%)
- All 3 varieties — Embryonal, alveolar, and pleomorphic are considered as Grade 3 in GTNM staging.
- Hence, the prognosis is not good.
Kaposi’s Sarcoma
- Vulnerable sections of people include — Jews, immunocompromised patients such as transplant recipients and AIDS patients.
- Typical sites: Legs. Other sites include the chest, arm, and neck in epidemic form (Africa) It presents as multiple pigmented sarcoma nodules in the leg.
- It is interesting to note that Kaposi’s sarcoma is not seen in transfusion-related ‘AIDS’.
- Purplish to red subcutaneous nodules in the leg followed by ulceration with bleeding is the manifestation.
- Combination chemotherapy with doxorubicin, etoposide and interferon has been used to control the disease.

Sarcomas That Metastasize To Lymph nodes
- Rhabdomyosarcoma
- Synovial sarcoma
- Epitheloid sarcoma
- MFH
- Angiosarcoma.
Useful Tips In A Case Of Soft Tissue Sarcoma
In undergraduate clinical examination, students are advised to offer soft tissue sarcoma as the diagnosis. When asked about the possible type, then only give a possible histological type based on various clinical features mentioned above. Ask the Following Questions To yourself, get ready for the clinical exams.
1. Is it soft tissue sarcoma?
Tumours arise from soft tissue, dilated veins, reddish skin, increase in local temperature, firm to hard, rapidly growing swelling, with late involvement of the skin. (Carcinoma starts in the skin)
2. What is the age of the patient?
- In children – Rhabdomyosarcoma, Undifferentiated sarcomas
- 20–40 years – Liposarcoma Synovial sarcoma Kaposi’s sarcoma
- Elderly – Angiosarcoma patients

3. Which site has it occurred?
- Head and neck – Angiosarcoma Rhabdomyosarcoma Osteogenic sarcoma (jaw)
- Distal extremity (limbs) – Synovial sarcoma, Epithelioid sarcoma, Clear cell sarcoma
- Retroperitoneum and mesentery – Liposarcoma
4. Has it spread to lymph nodes?
- Rhabdomyosarcoma
- Synovial sarcoma, Epithelioid sarcoma
5. Has it spread to the lungs or liver?
- Chest X-ray
- Ultrasound
6. Can I preserve the limb?
- Wide excision
- Compartmental excision
- Preoperative radiotherapy combined with surgery and postoperative radiotherapy
Leave a Reply