Malignant Melanoma Skin Tumours Notes
The skin, the outermost coat of the human body, functions as a protective cover against various insulting agents, such as ultraviolet radiation of sunlight, excessive heat and various chemical agents. Hence, no wonder it is one of the most common cancers in elderly patients.
Read And Learn More: Clinical Medicine And Surgery Notes
However, more than 90% of skin tumours are curable because of the following reasons:
- They are diagnosed early, and easily (unlike intra-abdominal malignancies) and they are low-grade cancers.
- Among skin cancers, about 70% are basal cell carcinomas, 20% are squamous cell carcinomas and 5% are melanocarcinomas.
- Other rare skin cancers are sebaceous carcinomas, dermoid cystic carcinomas, dermatofibrosarcomas, etc. In this chapter, only common malignant skin tumours are discussed.
- Also, some common skin lesions, such as corn and wart are also discussed in this chapter.

Classification Of Skin Tumours
1. Epidermal Tumours
- Epidermal Tumours Benign
- Papilloma
- Seborrhoeic keratosis
- Verrucous naevus
- Epidermal Tumours Malignant
- Basal cell carcinoma
- Epithelioma, Marjolin’s ulcer
2. Melanocytic Tumours
- Melanocytic Tumours Benign
- Junctional naevus
- Compound naevus
- Intradermal naevus
- Hutchinson’s freckle
- Hairy naevus
- Blue naevus
- Melanocytic Tumours Malignant
- Superficial spreading melanoma
- Nodular melanoma
- Lentigo maligna melanoma
3. Sweat gland tumours (malignant)
- Hidradenocarcinoma
- Adenoid cystic carcinoma
4. Sebaceous gland tumours
- Sebaceous adenoma
- Sebaceous carcinoma
5. Other tumours
- Dermatofibrosarcoma protuberans
- Trichofolliculoma (hair follicle tumour)
Premalignant Lesions Of The Skin
1. Chronic irritation
- The skin can occur due to various chemicals like dyes, tar, inorganic arsenic, etc. which contain various carcinogens. Coal tar contains polycyclic aromatic hydrocarbons like benzopyrenes which are carcinogenic.
2. Solar keratosis (senile keratosis):
- Prolonged exposure to sunrays can cause hyperkeratosis of the skin which is called solar keratosis.
- Skin changes occur due to the accumulated effect of ultraviolet rays over a period of many years. Ultraviolet rays are also present in phototherapy given in the treatment of psoriasis (PUVA therapy-Psoralen Ultra Violet-A).
Common sites: Back of hands, face, rim of ears.
- Age group: Middle age, more than 50 years.
- Clinically the lesion is an irregular, firm and irritating patch which is flat or raised.
- Malignancy should be suspected when the lesion becomes indurated, when a nonhealing ulcer develops, when the central crust is shed and when regional lymph nodes are palpable.

3. Chronic scar:
- Squamous cell carcinoma which develops in scar tissue is called Marjolin’s ulcer.
- Burns scar is the most common cause of Marjolin’s ulcer followed by scar due to varicose ulcer, snake bite scar, chronic osteomyelitis scar, and lupus vulgaris (tuberculosis of face) scar.
- Marjolin’s ulcer differs from squamous cell carcinoma by the following characteristics.
4. Radiodermatitis:
- Increased incidence of skin cancer was found in persons who worked in the X-ray department initially.
- Now, the incidence is less due to the usage of protective gear. Radiation change in the skin may vary from simple erythema initially to atrophy or hyperpigmentation. Later, this lesion changes into squamous cell carcinoma.

5. Bowen’s disease:
- Is an intraepidermal carcinoma. It is rare and occurs in middle-aged patients.
- It occurs on the skin of the trunk as scaly, erythematous plaques which are often multiple. They are brownish patches with raised margins. Microscopically, large clear cells are found (these cells are also found in Paget’s disease of the nipple).
6. Leukoplakia
7. Autosomal recessive disorders:
- In this group, one or more of the DNA repair enzymes are defective or deficient.
- As a result of this, sites exposed to the sun are vulnerable to the development of various skin cancers. Xeroderma pigmentosum and albinism have increased predisposition to skin cancer
Basal Cell Carcinoma (Rodent Ulcer)
It is the most common malignant skin tumour. Generally, it is a slow-growing neoplasm which can present as an ulcer of many years duration. In some cases, it can present as a locally penetrating, ulcerative and destructive lesion. It arises from the basal cell of the pilosebaceous adnexa and occurs only on the skin.
- Location: The majority of the lesions are found on the face above a line from the lobule of the ear to the angle of the mouth.

Common Sites Of The Eye
- Inner canthus of the eye
- Outer canthus of the eye
- Eyelids
- Bridge of the nose
- Around nasolabial fold
- These sites are the areas where the tears roll down. Hence, it is also called tear cancer.
Basal cell carcinoma cannot occur in the mucosal surfaces which do not have pilosebaceous adnexa, e.g. cervix, lips, tongue.
Precipitating Factors
- Ultraviolet rays: Basal cell carcinoma is common in Australia and New Zealand because of ultraviolet rays.
- Fair skin is vulnerable to the development of basal cell carcinoma.
- Arsenic once used in skin ointments, also increases the risk of basal cell carcinoma.
Basal Cell Carcinoma Clinical Features
- The most common clinical presentation is an ulcer that never heals. Sometimes healing takes place with scabbing and later it breaks down and forms an ulcer again.
- The ulcer has a raised and beaded edge, may be indurated and bleeds on touch.
- The base can be subcutaneous fat or deeper structures like muscle or bone depending upon invasion.
- Scabbing occurs only in benign ulcers. Basal cell carcinoma is the only malignant ulcer which shows scabbing.
- It can also present as a painless, firm, nodule, which. is pigmented with fine blood vessels on its surface.

Basal Cell Carcinoma—Types
- Nodular
- Pigmented
- Superficial
- Cystic
- Infiltrative
- It can present in a nodular ulcerative form.
- Rarely, it can be a cystic variety which does not show fluctuation.
- Field fire rodent ulcer is a rapidly growing rodent ulcer with destruction and disfigurement of the facial skin. It has an advancing edge with a healed central scar.
Differential diagnosis
- Keratoacanthoma: It occurs only in the face. Edge can be raised with ulceration, thus resembling basal cell carcinoma.
- Sclerosing angioma.
- Malignant melanoma: Pigmented basal cell carcinoma may be mistaken for malignant melanoma.
- Squamous cell carcinoma.
A brother and sister with xeroderma pigmentosa developed 33 and 26 skin malignancies respectively, which included basal cell, squamous cell carcinoma and malignant melanoma, from the age of 5 to 22 years.
Eventually, a boy died at 22 years age of. This is the sad part of this distressing and frustrating disease.


Spread
It spreads by local invasion. Even though slow growing, it slowly penetrates deep inside and destroys the underlying tissues like bone, cartilage or even eyeball. Hence, the name rodent ulcer.
It does not spread by lymphatics because the size of the tumour emboli is big. Blood spread is extremely rare.
Wedge Biopsy Investigations
Wedge biopsy from the edge of the ulcer. The edge is selected for the following reasons:
- Edge is the growing part, malignant cells are numerous
- The Centre has a slough or scab which may not reveal malignancy
- Comparison with normal skin is possible.
Microscopic Picture
- The central mass of polyhedral cells
- Cells are darkly stained
- With peripheral palisade layer of columnar cells. Cell nests, keratinisation and mitotic are absent.
Basal Cell Carcinoma Treatment
- Basal cell carcinoma responds well to radiation. Surgical excision also cures the disease.
- Radiation is indicated in elderly patients who have an extensive lesion which requires a complicated plastic reconstruction.
- Dosage: 4000-6000 cGy units.
- Surgery is indicated when the lesion is:
- Very close to the eye, adherent to the cartilage or bone
- In easily accessible sites like neck, hand, etc.
- In radiation failure cases
Types of surgery: Wide excision. This means excision of the growth with at least 1 cm of healthy margin and at the depth also.
The resulting defect is closed by:
- Primary suturing of the defect if the lesion is small
- Skin grafting if the defect is big as in the neck or dorsum of the hand
- Rotation flaps as in face for better cosmetic effect.
Squamous Cell Carcinoma (Epithelioma)
- It is the second most common malignant skin tumour after basal cell carcinoma. It arises from the prickle cell layer of the malpighian layer of the skin.
- It usually affects elderly males. All the premalignant conditions listed earlier apply to this condition.
- It can also occur de novo in the skin. Basosquamous carcinoma is the term applied when squamous cell carcinoma arises in a preexisting basal cell carcinoma.
- It is interesting to note that a variety of names have been given to squamous cell carcinoma when it occurs in different places.

Pathological Types
- Ulcerative variety—Most common.
- Cauliflower-like or proliferative growth
- Ulceroproliferative type
- The typical sites of skin, mucous membrane and junction involvement.
Squamous Cell Carcinoma Clinical Features
- Typically, it is an ulcerative or cauliflower-like lesion.
- Edge is everted and indurated.
- The base is indurated and it may be subcutaneous tissue, muscle or bone.
- The floor contains cancerous tissue which looks like granulation tissue. It is pale, friable, and bleeds easily on the touch.
- The surrounding area is also indurated.
- Mobility is usually restricted due to infiltration of underlying structures. In very early cases, ulcers can be moved along with skin over the underlying structures.
- Regional lymph nodes like inguinal lymph nodes (both vertical and horizontal groups) can get enlarged when squamous cell carcinoma affects the lower limb or abdominal wall. Hard lymph nodes are suggestive of secondaries.



Spread
1. Local spread occurs by infiltration into the surrounding tissues. Depending on the site, various structures can be involved. Some examples are:
- Tendon involvement in the dorsum of the hand.
- Muscle involvement in the abdominal wall.
- Bone involvement like tibia in carcinoma developing in a varicose ulcer or mandible in carcinoma cheek.
2. Lymphatic spread is the chief method of spread even though it occurs relatively late. Regional nodes are involved first.
- Nodes which are soft to firm and tender are due to secondary infection.
- Nodes which are hard, non-tender, with or without fixity are due to secondary deposits.
- In untreated cases, nodes start ulcerating through the skin resulting in bleeding and pain.
- As already stated, nodes do not get involved in Marjolin’s ulcer.
3. Blood spread is rare and late.
Differential Diagnosis
Squamous Cell Carcinoma Investigations
- A wedge biopsy from the edge of the ulcer or growth is taken.
- Microscopic picture: 80% of these cancers are well differentiated.
- It is characterised by a central structureless mass of keratin surrounded by normal-looking squamous cells which are arranged in a concentric manner like onion skin. This whole appearance is called an epithelial pearl or cell nest.
- In 20% of cases, cells are undifferentiated with numerous mitoses, without keratinization.
Differential Diagnosis
- Basal cell carcinoma
- Keratoacanthoma
- Papilloma
- Pyogenic granuloma
- Tuberculous ulcer
Broder’s Classification
- Well-differentiated 75% keratin pearls
- Moderately differentiated 50% keratin pearls
- Poorly differentiated 25% keratin pearls
- <25% keratin pearls
Squamous Cell Carcinoma Treatment
Treatment can be classified as “treatment of the primary” and “treatment of the secondaries”.
Primary Treatment: Squamous Cell Carcinoma Is Treated By Wide Excision Or Radiotherapy.
- Surgery
- It involves the removal of growth along with 2 cm of normal healthy tissue from the palpable indurated edge of the tumour.
- Indications OfSurgery
- When the lesion is small and superficial
- When the lesion has involved deeper tissues like muscles, cartilage or bone, etc.
- Radiorecurrent cases
- Reconstruction: After wide excision, the defect can be closed primarily or with a split skin graft or a flap to reconstruct the part depending upon the extent of resection. If the growth is fixed to the tibia, below-knee amputation is the treatment.
- Radiotherapy
Indications for radiotherapy
- Well-differentiated carcinoma
- Patients who are not fit for surgery
Dosage: 6000 cGy units over 6 weeks, 200 units/day.
2. Treatment Of Secondaries
- 30–40% of the enlarged regional nodes are due to secondary infection. Once the primary is treated or controlled along with antibiotics, lymph nodes regress. In such cases, a ‘wait and watch policy’ is observed.
- If lymph nodes do not regress or are hard and mobile, FNAC can be done to confirm the diagnosis followed by radical block dissection. Thus, squamous cell carcinoma of the leg requires inguinal block dissection.
- If lymph nodes are hard and fixed to the femoral vessels, palliative radiotherapy is given. Even in advanced fungating lesions, the response rate to radiotherapy is reasonably good.
- Dosage: 3000–4000 cGy units over 3–4 weeks, 200 units/day.
Structures removed in inguinal block dissection
- The superficial group of nodes consists of a horizontal chain which lies below the inguinal ligament and a vertical chain which lies along the upper 5–6 cm of the long saphenous vein. These two groups of nodes form the letter T.
- The deep glands are located alongside the proximal end of the femoral vein, and one lies within the femoral canal.
- Fat, fascia, and lymphatics are cleared from 2 cm above the inguinal ligament up to 2 cm below the saphenofemoral junction. The medial clearance is important upto femoral canal. 8–10 cm of long saphenous vein near its termination is removed to facilitate lymph node clearance.
Complications of inguinal block dissection and treatment/prophylaxis
- Wound infection → Broad-spectrum antibiotics
- Lymphorrhoea → Adequate drainage
- Haemorrhage → Perfect haemostasis
- Femoral blowout →Sartorius muscle slide to cover femoral vessels at the end of surgery

A summary of the treatment of squamous cell carcinoma.
Melanocytic Tumours Malignant Melanoma
Simple Melanocytic Tumours
- These are also called pigmented naevi which are composed of modified melanocytes derived from the neural crest.
- All naevi have excess melanin pigmentation because of which they are tan-brown or black in colour.
- They are located in the basal layer of the epidermis. They are benign.
They are of the following types.
1. Junctional naevus:
- Located within the epidermis at the dermo-epidermal junction. They are common in children. They appear as tan-brown to black macules.
- They are smooth, flat and hairless moles.
- As they enlarge, they become slightly raised and can evolve into an intradermal or a compound naevus or a malignant melanoma.
- Junctional naevus commonly occurs on the palm, sole, digits and genitalia and the majority of malignant melanoma develop from junctional naevus.
2. Compound naevus:
- As the mole enlarges, naeval cells also appear in the dermis along the intraepidermal cells.
- Such moles are described as compound naevi. These are found usually in adolescents and are usually benign.
3. Intradermal naevus:
- It is the most common mole in adults. Because of its deep-seated nature, it appears blue, hence the name blue naevus.
- It is seen on the scalp and face. It contains hair and it usually does not become malignant.

4. Congenital pigmented naevus, which is present at birth, has a greater potential for malignant change. It can involve extensive areas of the skin (Giant).
5. Dysplastic naevi are different from acquired naevi in the following ways:
- Malignant potential is more.
- Family members may have such lesions.
- Such a syndrome is described as familial dysplastic naevus syndrome.
Malignant Melanoma (Melanocarcinoma)
- It is a malignant tumour arising from pigment-forming cells (melanoblasts) which are derived from the neural crest.
- Melanoblasts and melanocytes convert dihydroxyphenylalanine (DOPA) into melanin. This is called a positive DOPA reaction.
- It is a potentially curable tumour in its early stages. If left untreated or if not treated properly, it disseminates rapidly, showers the body with tumour emboli and offers a very painful death.
Common sites of malignant melanoma
- Head and neck 20–30%
- Lower extremity 20–30%
- Trunk 20–30%
Positive Dopa Reaction

- The remaining cases occur in upper extremities, genitalia, choroid of the eye, etc.
Aetiopathogenesis
1. Ultraviolet rays:
- It is more common in white-skinned people. There is a linear correlation between intensity of exposure to sunlight and malignant melanoma in white-skinned people1.
- White-skinned people who live close to the equator have an increased tendency to develop malignant melanoma.
- Thus, the highest incidence is found in Queensland (Australia). For the same reasons, malignant melanoma is common in the United Kingdom, North America, Australia, etc.
2. Age and sex:
- Malignant melanoma is more common in females. The higher incidence of the disease is found during the reproductive age period.
- Even though oestrogen and progesterone receptors are found in malignant melanoma in some patients, their true role is not yet established.

3. Genetic factors:
- Increased incidence has been found in patients with familial dysplastic naevus syndrome.
- The disease is also common in individuals of the Celtic race who have a family history of malignant melanoma (3–5%).
4. Trauma:
- Malignant melanoma occurs in the sole in African Blacks. Whether trauma is the cause is not clear.
5. Pre-existing mole:
- Approximately 50% of melanomas arise in a preexisting mole, and 50% arise de novo in the normal skin.
- Malignant change occurs in the junctional or compound naevus. Malignancy should be suspected where the following changes occur in a mole.
- Enlargement
- More pigmentation
- Ulceration
- Itching
- Bleeding
- Development of the halo surrounding the lesion.
6. Increased incidence of malignant melanoma has been found in patients with renal transplantation and leukaemia as a result of immunosuppression.
7. Xeroderma pigmentosa and albinism patients are susceptible for melanomas.
Pathology
Microscopic picture:
- Anaplastic, pigment-laden melanocytes are confined to the epidermis. The cells which have vacuolated cytoplasm (Paget’s cells resembling those seen in Paget’s disease of the breast) are found. Cells also invade the dermis.
- Along with pigment-laden macrophages, dermal infiltration of lymphocytes1 may be present. Rarely, anaplastic melanocytes do not form pigment (amelanotic melanoma).
- All melanomas (except nodular) show radial growth initially in the form of intraepidermal growth.
- However, nodular melanoma has a vertical growth phase, thus involving the dermis leading to nodule formation. This has a poor prognosis.
Pathological Grading of Malignant Melanoma
(not followed nowadays)
Clarke’s level of invasion is represented in the diagram.
- Level 1 → Tumour cells confined to the basement membrane
- Level 2 → Tumour extension into the papillary dermis
- Level 3 → Tumour reaches the interface between papillary dermis and reticular dermis
- Level 4 → Tumour reaches the reticular dermis
- Level 5 → Tumour invades subcutaneous fat
Breslow described the staging depending on the maximum thickness at the centre of the lesion.
- Stage 1 → Thickness less than 0.75 mm
- Stage 2 → 0.76 to 1.5 mm
- Stage 3 → 1.51 to 3 mm
- Stage 4 → More than 3 mm


Malignant melanoma Clinical Features
- Malignant melanoma can present as changes in the pre-existing mole which are already described.
- The patient can present with a non-healing ulcer of the sole.
- It is a painless ulcer
- Edges are irregular
- Floor is irregular
- Bleeds on touch
- Typically, the ulcer is pigmented. In 10% of patients, pigment is absent called amelanotic melanoma.
- The lesion is firm in consistency and induration is absent.
- A halo may be present surrounding the ulcer.

- The lesion moves with the skin and is usually not fixed to underlying structures.
- Satellite nodules (within 2 cm of the primary) may be found surrounding the lesion which is due to spread through intradermal lymphatics. Such patients will have greatly enlarged, firm, non-tender nodes.


ABCDE of Melanoma
Staging
- 1A: Thickness less than 0.75 mm
- 1B: Thickness between 0.76 to 1.5 mm
- 2A: Thickness between 1.51 to 4.0 mm
- 2B: Thickness more than 4.0 mm
- 3A : Any of the above + nodes less than 3 cm
- 3B : Any of the above + nodes more than 3 cm
- 4 : Any of the above + any node + M1 (distant spread).
ABODE Of Melanoma
- A: Asymmetry
- B: Border irregular
- C: Colour Variegation
- D: Diameter >6 mm
- E: Elevation
Differential Diagnosis
Spread
1. Local spread
- Occurs mainly by continuity and contiguity. Satellite nodules are due to local and lymphatic spread, situated within 2 cm of the primary lesion.
- Malignant melanoma rarely infiltrates the deep fascia unless and until a ‘blunder biopsy’ is done. Inadequate local excision can result in local recurrence later.
2. Lymphatic spread is the principal mode of spread. Regional nodes get involved very early in malignant melanoma thus altering the prognosis. Thus, nodes can get enlarged to a large extent even when the lesion looks innocent.
Spread occurs both by permeation and embolisation. Permeation produces satellite nodules and in-transit nodules which develop between primary and secondary. Embolisation occurs rapidly and early producing massive regional nodes.
Basal Cell Carcinoma Differential Diagnosis
- Pigmented basal cell carcinoma, Histiocytoma (sclerosing angioma), Naevus
- Kaposi’s sarcoma, Cavernous haemangioma
In-transit metastasis appears in the skin as intracutaneous metastasis. They are thought to be due to melanoma cells trapped in lymphatic vessels.
3. Blood spread occurs relatively early and it causes secondaries in the liver, lungs, brain and bones producing miserable, pathetic situations.
Basal Cell Carcinoma Investigations
- There is no specific investigation except an excision biopsy of the lesion. Excision with 1 cm of the margin is all that is required. Incisional biopsy is avoided because of the following reasons:
- It may injure the deep fascia and it may open up a new plane of spread.
- It does not allow the pathologist to perform a detailed histological examination
- Nonspecific investigations to look for metastasis are:
- Chest X-ray—Cannon ball secondary
- Ultrasound abdomen- Secondaries in liver
- X-ray of involved bone Osteolytic lesions
- FNAC of the regional lymph nodes
- Fine needle aspiration of groin nodes is helpful in detecting the spread and staging the disease.
- In advanced cases punch biopsy can also be taken.
- Chest X-ray and ultrasound abdomen are other relevant investigations.
Malignant Melanoma Sole

Malignant Melanoma Sole Treatment
Surgery is the main modality of the treatment available for malignant melanoma. All other modalities of treatment are only palliative and supportive.
Types of surgery possible are as follows
- Excision biopsy—wide excision: A small lesion of 2–4 cm can be excised even under local anaesthesia with 1 cm of healthy margin around (narrow excision). Defects can be closed by primary suturing.
- While excising the tumour, it is better not to handle the tumour. It is possible to remove the tumour by strictly adhering to the principle of the ‘No Touch’ technique.
- Clarke’s level 2 lesions are managed by a wider excision along with 2 cm of healthy margin around. The resulting defect is closed by split skin grafting.
- Subungual malignant melanoma is treated by amputation of the digit.
- Malignant melanoma of the choroid has a good prognosis. It is treated by enucleation of the eye.
- Amputations (advanced and large lesions).

Management Of Lymph Nodes
- If lymph nodes are situated adjacent to the primary lesion, block dissection is done along with the primary lesion in continuity so as to include ‘in-transit’ deposits.
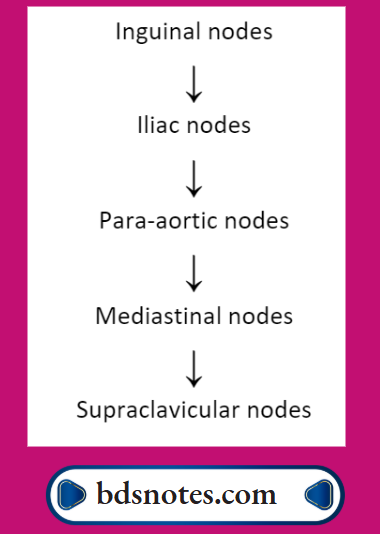
- If lymph nodes are away, radical block dissection is done. Example: for a lower limb malignant melanoma inguinal nodes along with iliac nodes are removed. This is called ilioinguinal block dissection. If these groups of nodes are positive at the frozen section, lymph node clearance should include lymph nodes of obturator vessels. This is called ilio-obturator block dissection.
- Sentinel lymph node mapping: Isosulfan Blue is injected intradermally and the node which gets stained is identified and sent for frozen section (Haematoxylin and eosin stains and immunohistochemical technique). If the node is positive regional lymphadenectomy is done even when nodes are clinically not palpable.
- At least 20– 30% of the patients who are in Stage I will go to Stage III after sentinel node biopsy. Also, there is a definite survival advantage in patients who undergo sentinel node biopsy and regional lymphadenectomy when the nodes are not palpable.
- Otherwise, prophylactic block dissection is indicated only if the melanoma has poor prognostic histological factors.
- Sentinel lymph node mapping: Isosulfan Blue is injected intradermally and the node which gets stained is identified and sent for frozen section (Haematoxylin and eosin stains and immunohistochemical technique). If the node is positive regional lymphadenectomy is done even when nodes are clinically not palpable.
- If lymph nodes are enlarged, hard and fixed, palliative radiotherapy is given.

Management Of Advanced Malignant Melanoma
- The aim of treating this group of patients is only to afford a reasonable palliation. More than 50% of patients, who have metastasis in the regional nodes are dead by the end of one year.
- The choroid has no lymphatics. Hence, melanoma in the choroid has a good prognosis. However, blood spread and metastasis to the liver have been reported even 15–20 years later.
Malignant Melanoma Modes of Treatment
- Radiotherapy for bone, brain and skin metastasis
- Systemic chemotherapy: DTIC (Diethyl Triamine Imidazole Carboxamide) is the standard agent.
- The response rate is around 20-30%. Cisplatin, Vinblastine, and Bleomycin are also used in combination.
- The addition of immunomodulators like BCG or Levamisole to chemotherapy has been tried.
- Intralesional injection of BCG has caused regression of the cutaneous nodules in some patients.
- Immunotherapy
- Alpha-interferon
- Interleukin-2 (IL-2), interferon
- Monoclonal antibodies: These are directed against antigens, expressed on the surface of melanoma cells. These antibodies like IgG3 activate the immune system.
- Cutaneous nodules can be managed by surgery or CO2 laser excision.
4. Hormone treatment: Antioestrogens like tamoxifen have been tried in systemic disease with a 15–20% response rate.
5. Isolated limb perfusion:
- This is tried when there are extensive in-transit deposits in the limb or recurrent disease in the limb.
- Melphalan is the drug of choice. A tourniquet is applied first, the femoral vein and artery are cannulated, and the blood which comes out is passed through a pump and oxygenator, into which a high dose of Melphalan or DTIC is given. The input temperature is kept at 41° C.
- Therapy is aimed at controlling local disease in the limb and to give a better functional limb even in the presence of metastasis.
Complications of isolated limb perfusion
- Deep vein thrombosis
- Pulmonary emboli
- Complications of anticoagulants
- Damage to the vessels.

Summary of Skin Tumours Other Malignant Skin Tumours Dermatofibrosarcoma Protuberans
- This is a locally malignant tumour arising from the dermis
- Common sites are the trunk, and the flexor region of the limbs. It presents as a nodular (bossellated) ulcerative lesion of ‘many years’ duration.
- Regional lymph node involvement is uncommon.
- It is less aggressive, hence curable.
- Treatment is by local-wide excision followed by primary closure or skin grafting.
Kaposi’s Angiosarcoma
- Common in the Black population.
- This neoplasm arises from proliferating capillary vessels and perivascular connective tissue cells.
- Multiple, purplish nodules appear in the limb, which ulcerates with bleeding, is a characteristic feature.
- Regional lymph node involvement can occur.
- Increasing incidence due to AIDS.
Diseases Associated With Kaposi’s Sarcoma
- Diabetes mellitus
- Lymphoma
- Following renal transplantation
- Acute and chronic immunosuppression (HIV)
Types Of Kaposi’s Sarcoma
- European: Elderly males
- African: Young and children
- Transplant: Due to immunosuppression
- AIDS: Homosexuals
Other Malignant Skin Tumours Differential Diagnosis
- Malignant melanoma
- Soft tissue sarcoma
- Multiple cutaneous metastasis
- T Cell lymphoma.
Other Skin Lesions
- They arise from sebaceous glands, sweat glands, hair follicles, etc.
- A few examples are syringoma, hidradenoma, trichoepithelioma, etc.
- They present as localised swelling treated by excision.
- They have to be kept in mind as a differential diagnosis for malignant skin tumours. Details of a few skin lesions are given below:
Keratoacanthoma—Molluscum Sebaceum, Molluscum
Pseudocarcinomatosum
- Self-limiting, benign neoplasm of viral origin (probably).
- Arises due to overgrowth of the hair follicle and subsequent spontaneous regression is characteristic.
- It is a painless swelling in the skin with a central dark brown core. After initial rapid growth of 2–4 weeks, spontaneous regression occurs in 24 hours. After the separation of the central core, the lump diminishes in size leaving a deep indrawn scar.
- Usually single, the face is the most common site
- Like a sebaceous cyst, it presents as hemispherical swelling.
- Treated by excision.
Types Of Exocrine Glands
- Holocrine: Entire cell dies or disintegrates to liberate secretion, e.g. sebaceous gland
- Apocrine: Only the luminal part of the cell disintegrates, cell regeneration takes place from the nucleus and basal portion, e.g. mammary gland
- Merocrine: Without destruction of the cells, secretion is discharged—most of the glands belong to this type
Turban Tumour
It is the blanket term used to describe a tumour occupying the whole of the scalp thus resembling a turban.
- Most often used to describe multiple cylindromata
- They produce pink nodular masses
- Diagnosis confirmed by biopsy
- For differential diagnosis
- Treatment includes excision and reconstruction by skin grafting or rotational flaps.
Corn
It is a popular painful lesion in the plantar surface of the foot (sole of the foot)
- It affects the plantar surface of the toes and soles of the feet.
- Corn develops due to intermittent pressure over a limited area.
- Basically, it is a localized hyper-keratinisation of the skin with a hard central core.
- It will be a ‘CONE’ shaped lesion with a broad surface and narrow at a deeper plane.
- They are painful and very tender.
- Most of these are hard corns.
- Soft corn can occur in between the toes.
Turban Tumour Types
- Very rare
- Multiple cylindromata
- Multiple nodular basal cell carcinoma
- Hidradenomata
- Plexiform neurofibromatosa of scalp

Turban Tumour Treatment
- Diabetic patients have to be carefully explained the consequences of a ‘mistreated’ com.
- Sensations and pulsation have to be checked in those patients.
- Symptomatic corns have to be excised, one has to take out a good ‘CONE’ shaped tissue for a permanent cure. Otherwise, recurrence can occur.
Wart
- A wart is a rough excrescence on the skin.
- Papillomaviruses are responsible for this.
- They are pigmented, keratinized, irregular lesions and common in young adults.
- Common sites: Fingers, feet, genitalia, beard area, etc.
- Venereal warts: They are also called papilloma accuminata. They can occur in the anal region, perineum and in the coronal sulcus of the penis. Some of the warts may regress spontaneously. Fulguration with diathermy is the treatment.
Merkel Cell Carcinoma
- It is derived from neuroendocrine cells which function as touch receptors.
Highly malignant tumour. - Elderly white males are affected.
- Sun-affected areas, such as the head and neck region are involved probably due to ultraviolet rays.
- Surgery, radiation and chemotherapy have been tried.
- Histopathological report resembles metastatic oat cell carcinoma.
Examination Of Skin And Skin Tumours
- Introduction: Skin malignancies such as basal cell carcinoma, epithelioma (squamous cell carcinoma) and malignant melanoma are common cases in the university clinical examinations.
- No doubt, they are classified under malignant ulcers.
- However, a discussion of these malignancies in the ulcer chapter dilutes the clinical examination of these malignant ulcers more so with reference to malignant melanoma (Malignant skin tumour arising from melanin pigment).
- For students, it is important first to realize that a given ulcer or a lesion is malignant, then only they should refer to and follow this chapter for further clinical methods.
- It is understood that by this time when students start reading this chapter they are thorough with the ulcer chapter.
Skin Tumours History
- Where are you from and what is your occupation? Especially in whites, malignant melanoma is common in patients who are exposed too much to sunburns (outdoor occupations). Those who are exposed to chemicals, such as tar or dye industries are more susceptible because of chronic irritation of the skin.
- How does it start? Often malignant melanoma in the leg more so on the sole starts as an ulcer or an itchy lesion in a preexisting naevus.
- Did you have any mole? The patient may tell that I started scratching or itching over the mole and an ulcer developed. Is there any trauma? Trivial trauma might have brought the attention of the patient to the lesion.
- How is the progress? Often patient may show you a lesion which is so slow-growing growing you may not believe it. Such lesions are basal cell carcinomas which are very slow-growing. Melanomas can grow and spread to 5–6 cm size by 2–3 months. Is it becoming bigger or remaining the same or is it healing?
- An ulcer which is becoming bigger is a spreading ulcer. A non-healing and spreading ulcer can be malignant especially malignant melanoma and the leg is one of the common sites of melanoma.
- Do you have any pain? Pain is not a feature of skin malignancies unless secondarily infected or infiltrated sensitive structures such as bone. This is the reason why many patients come late to the hospital.
- Did you see any blood coming out of the wound? Malignant ulcer especially squamous cell carcinomas are very friable, they easily bleed especially on touch.
- Has the ulcer healed for some time? Healing is the property of benign ulcers. But basal cell carcinoma is an exception to this rule. Healing in between sometimes with scab and again ulcerating is typical of basal cell carcinoma. It reflects the slow indolent nature of the tumour.
- Do you have any groin swelling? The presence of groin swelling reflects enlargement of inguinal or iliac lymph nodes.
- Do you have any other complaints? Squamous cell carcinoma is relatively slow growing and distant metastasis is uncommon, but malignant melanoma can rapidly grow and spread to other organs. Thus symptoms suggestive of metastasis should be asked for. Examples are given below.
- Cough with or without haemoptysis: Pulmonary secondaries
- Bony pains especially backbones: Bony metastasis
- Headache, vomiting: Cerebral metastasis
- Pain right hypochondrium/jaundice: Liver metastasis
- Have you taken any treatment for this condition? Patients may tell you about hospitalization, biopsy FNAC, etc. Try getting the reports from the patient.
- Have any family members had this problem? Xeroderma pigmentosum is a definite pre-malignant condition for all skin malignancies. It can run in family members.
Pearls Of Wisdom
Easy friability and bleeding gums in a young patient should raise the suspicion of leukaemia.
Past History
- Any history suggestive of chronic ulcers or history of burns should be asked for. As you know squamous cell carcinoma arises in scar tissue, especially burn scars. Such lesions are called Marjolin’s ulcers.
- Did you undergo surgery in the past? The patient may show groin region swelling or a few lesions in the leg. But he says he has undergone surgery in the past for a pigmented lesion in the leg/sole. The diagnosis is quite obvious—malignant melanoma.

General Physical Examination
- Chronic anaemia: Poor wound healing
- Multiple lymph nodes: Spread from melanoma or epithelioma
Local Examination Inspection
- First, decide whether the lesion is a swelling, an ulcer or an ulceroproliferative lesion (growth) and describe it in the usual way, like location, size, shape, surface for a swelling and floor for an ulcer. Describe the discharge.
- Serous and serosanguinous discharge is common for any ulcer. Mention any pigmentation in the lesion or in the surrounding area.
- Malignant ulcers are friable and bleeding is a feature. Then describe the surrounding area for any swelling, pigmentation or scarring.
Some typical examples/lesions are described below.
1. Malignant melanoma in the sole: A pigmented ulcer is present in the sole measuring about 2–4 cm in size which is irregular in shape, the floor is covered with unhealthy tissue, edges are everted, and pigmented.
- Bloody discharge is seen on the floor of the ulcer. The surrounding area is pigmented and oedematous (if lymphatics are blocked or due to secondary infection). You may find nodules surrounding the lesion.
- They are called satellite nodules which are characteristic of malignant melanoma. They are due to lymphatic spread. Also, such nodules may be present in the leg which are called in-transit deposits.
Special Check List For Malignant Melanoma In Inspection
- Pigmentation
- Loss of normal skin marking (crease)
- Oozing
- Brown Halo is due to pigment produced by the tumour which spreads into the normal skin
- Flat mole changes to nodule or plaque
- Normal Impalpable mole becomes palpable

Pearls of wisdom
Multiple circumoral moles are seen in Peutz-Jegher’s syndrome. They are patches of lentigo and they do not turn malignant.
2. Epithelioma/Squamous cell carcinoma/ Marjolins ulcer:
Ulceroproliferative growth present in the leg or trunk measuring about 4–5 cm in size, edges are everted, floor covered with necrotic tissue or tumour tissue, with serous discharge or bloody discharge, the surrounding area is oedematous. Scarring is present in Marjolin’s ulcer.

Palpation
- Tenderness and local rise in temperature: Malignant ulcers are non-tender unless they are infected or infiltrated bones. Local rise in temperature is indicative of increased vascularity due to inflammation or vascular tumours.
- It is important to realize that even malignant ulcers are painful if they are infected or when they infiltrate bones.
- Edge: Induration (hardness) of the edge is characteristic of squamous cell carcinoma. Induration occurs due to extensive fibrosis. It is said to be a host defence mechanism. By causing fibrosis, lymphatic spread is delayed.
- Base: The base can be tendons, muscles or bone depending upon the site of the ulcer. Marked induration at the house is diagnostic of squamous cell carcinoma.
- It is interesting to note that induration is comparatively less in malignant melanoma as it induces less desmoplastic reaction.
- Depth: It is not an important sign. However, if possible, try to assess the depth of the ulcer.
- Penetrating or perforating ulcers in the sole, pressure sores (bedsores) will be very deep up to the bone.
- This can be done by probing which is not recommended for the fear of risk. Melanoma over the sole may infiltrate deeper structures especially when a patient comes late to the hospital.
- Mobility: A gentle attempt is made to move the ulcer or growth to know its fixity to the underlying tissues. Malignant ulcers or growth arise from the skin and hence they move with the skin. Immobility is a feature of infiltration into deeper structures such as bones.
- Bleeding: Epithelioma is friable like a cauliflower. On gentle palpation, it bleeds.
- Surrounding area:
- Thickening and induration is found in squamous cell carcinoma.
- Tenderness and pitting on pressure indicate spreading inflammation surrounding the ulcer.
- Satellite nodules and in-transit deposits: If present, describe them—they are non-tender, firm swellings which are black.
- Function of the joint: Movements of the involved joint are restricted either due to pain, involvement of the joint or due to infiltration into the joint by malignant ulcers.
- Regional lymph nodes
- Tender and enlarged- Acute secondary infection
- Non-tender and hard squamous cell carcinoma
- Non-tender, large, firm TO HARD, multiple-malignant melanoma.
Malignant lesions and nodes are usually hard, but when the tumour and nodes grow rapidly, necrosis results and they may feel firm or even soft—in such situations, better to use the term variable consistency.
Differential Diagnosis Of A Nodule In The Skin
- Malignant melanoma–satellite nodule or in-transit deposits
- T cell lymphoma
- Metastasis in the skin
- Keratoacanthoma
- Neurilemmoma/Neurofibroma
- Kaposi’s sarcoma
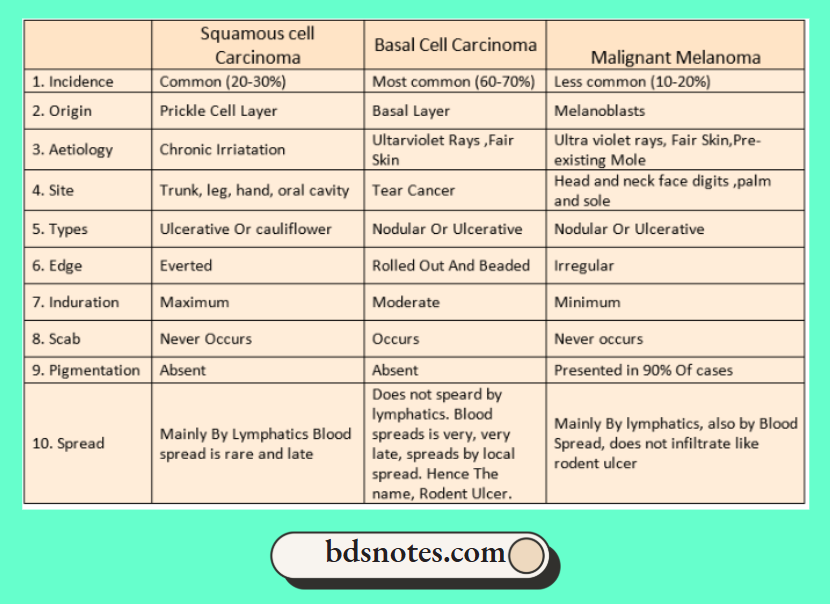
Malignant Melanoma Differential Diagnosis
1. Malignant melanoma:
- It is a malignant tumour arising from the neural crest and so ectodermal in origin.
- It is common in whites, however, also seen in other races. Exposure to sunlight has been blamed as one of the factors.
- It is rare before puberty. Majority of the malignant melanoma arises in pre-existing moles. It starts as an itchy lesion or with ulcerations and bleeding.
- Classically lesion is pigmented (amelanotic is without pigmentation) with or without satellite nodules and in-transit deposits. Groin nodes are enlarged and they are a big size too.
2. Epithelioma/Squamous cell carcinoma and Marjolin’s ulcer:
- It is common in elderly patients. The chief precipitating factor is chronic irritation. Thus, Kangri cancer, Kang cancer, Chimney sweep cancer, Saree and Dhothi cancer are other names of epithelioma when it occurs in different locations.
- A typical lesion is an ulceroproliferative growth resembling cauliflower with everted edges. Flood bleeds on touch.
- The base is indurated. Slowly growth infiltrates the deeper structures and gets fixed. Satellite nodules and in-transit deposits are not a feature of epithelioma.
- Regional lymph node enlargement is an important feature. Affected nodes are hard and indurated.
- Tender nodes suggest secondary infection, which is more common in epithelioma than malignant melanoma.
- It should be noted that Marjolin’s ulcer does not spread to lymph nodes because lymphatics are obliterated due to scarring.
- However, when the lesion invades normal skin, lymph nodes do get enlarged. Kindl,e see the differences between Marjolin’s ulcer and Squamous cell carcinoma.
3. Basal cell carcinoma (Rodent ulcer):
- It is the most common malignant skin tumour arising from the basal cell of the pilosebaceous adnexa. It is diagnosed by the long duration of the history of a non-healing ulcer and its typical location.
- Classical location: The majority of the lesions are found on the face above a line from the lobule of the ear to the angle of the mouth. In some cases, it can present as a locally penetrating, ulcerative and destructive lesion.
- The ulcer has a raised and beaded edge, induration may be present and bleeds on touch. The base can be subcutaneous fat or deeper structures like muscle or bone depending upon invasion.
- Scabbing also takes place suggesting a slow indolent nature of the disease. It can also present as a painless, firm, nodule, which is pigmented with fine blood vessels on its surface.
Differential diagnosis for basal cell carcinoma
- Keratoacanthoma: It occurs only in the face. Edge can be raised with ulceration, thus resembling basal cell carcinoma.
- Sclerosing angioma
- Malignant melanoma: Pigmented basal cell carcinoma may be mistaken for malignant melanoma.
- Squamous cell carcinoma: The face is not a common site of epithelioma. Everted edge, induration and significant nodes confirm the diagnosis.
Malignant Melanoma Clinical Discussion
- What are the Ectodermal Sites for melanoma? The anal canal, choroids and meninges,
- What are the areas of junctional naevus? Palm, sole, face, neck, subungual, digits and genitalia.
- What is amelanotic melanoma? In 10% of patients, pigment is absent. They are called amelanotic melanoma.
- Which are the areas wherein basal cell carcinoma cannot occur? It cannot occur in the mucosal surfaces which do not have pilosebaceous adnexa, e.g. cervix, lips, tongue.
- Satellite nodules (within 2 cm of the primary) may be found surrounding the lesion which is due to spread through intradermal lymphatics.
- What is Temozolamide? It is an oral analogue of dacarbazine. It is supposed to decrease the incidence of cerebral metastasis.
Skin Lesions
Non-palpable
- Macule: Flat, circumscribed lesion in the skin having a diameter of less than 1 cm
- Patch: Flat circumscribed lesion in the skin having a diameter 1 cm or more: Vitiligo patch, hypopigmented patch in leprosy.
Palpable
- Papule: A solid elevated lesion up to 5 mm in diameter. Examples: Wart
- Nodule: A solid elevated lesion more than 5 mm in diameter, usually about 1 cm in diameter. Metastatic deposits in the skin, hard subcutaneous nodules in rheumatoid arthritis, and nodules of neurofibromatosis.
- Plaque. It is classically seen in psoriasis. It is a confluence of papules or nodules having large flat-topped raised lesions.
- Wheal: It is a round elevated lesion due to the accumulation of fluid in the dermis. It is a primary lesion seen in urticaria.
- Vesicle: It is a lesion due to the accumulation of fluid in the elevated horny layer of skin thus (up to 5 mm in diameter), resulting in a lesion elevated above the surface.
- Bullae: A larger blister of more than 5 mm may contain serous, sero-purulent or turbid fluid.
- Pustule: Classically described for hair follicle infection. It is a small yellow elevated, circumscribed lesion in the skin.
- What is Merkel Cell Carcinoma? It is a highly malignant tumour derived from neuroendocrine cells which function as touch receptors.
Leave a Reply