Describe Various Intraoral Radiographic Technique To Diagnose Various Periapical Lesion.
Intraoral radiographic techniques to diagnose periapicallesion.
Periapical Radiography
Periapical radiography is an intraoral radiographic technique showing all of the tooth and the surrounding bone.
There are two techniques used to take periapical radiographs:
- The paralleling or right angle or long cone technique.
- The bisecting angle or short cone technique.
“Understanding the role of intraoral radiography in diagnosing periapical pathologies: Q&A explained”
Read And Learn More: Oral Radiology Question And Answers
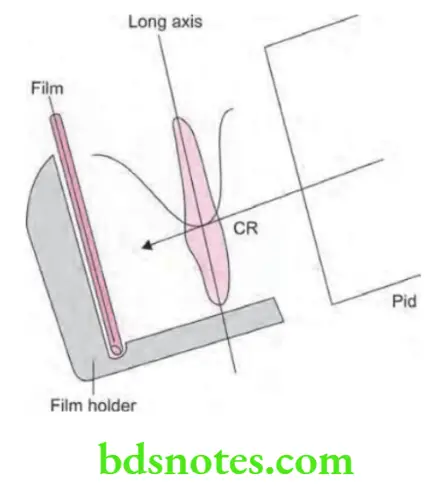
Paralleling technique or Long cone technique
- X-ray film is supported parallel to the long axis of the teeth and the central ray of the X-ray beam is directed at right angles to the teeth and film.
- To achieve parallelism between the film and the tooth, the film must be placed away from the tooth, towards the middle of the oral cavity.
- Because the film is placed away from the tooth, image magnification and loss of definition results. To compensate for image magnification, the target film distance must also be increased to ensure that only the most parallel ray will be directed at the tooth and the film. So this technique is also called as long cone technique.
- Along cone of 12 inches is used and kVp used is 85–90 kVp
- X-rays are directed perpendicular to film so there is less geometric distortion, less magnification and more definition.
“Importance of studying intraoral radiography for better periapical lesion outcomes: Questions explained”
Diagnosis Of Periapical Lesions Using X-Rays
“Common challenges in using intraoral radiography for periapical lesions: FAQs provided”
Procedure for Paralleling Technique
- Prepare unit for exposure: Barriers should be placed for universal infection control and receptors as well as receptor-holding instruments should be ready at chairside.
- Greet and seat the patient: Patient should be positioned upright in the chair with the back and head well supported, and briefly describe the procedures that are to be performed. Dental chair should be positioned low for the maxillary projections and elevated for mandibular projections. Patient should be asked to remove eyeglasses, jewellery which comes in the path of X-ray beam and all removable appliances. Patient should wear a protective apron regardless of whether a single image or a full series is to be made.
- Adjust the x-ray unit setting: X-ray machine should be set for the proper kVp, mA, and exposure time. Generally only the exposure time is adjusted for the various anatomic locations.
- Wash your hands thoroughly and wear appropriate personal protective equipment: Wash your hands with soap and water, preferably in front of the patient or at least in an area where the patient can observe or be aware of this step. Put on disposable gloves and disposable gown or coat.
- Examine the oral cavity: Before placing any of the receptors inside mouth, teeth of the patient should be examined to estimate their axial inclination, which influences placement of receptor. Also note tori or other obstructions that may modify receptor placement.
“Steps to explain different intraoral radiographic techniques: Periapical vs bitewing: Q&A guide”
- Position the x-ray tube head: X-ray tube head should be moved to the side to be examined so that it is easily accessible for final positioning after the receptor has been placed in the mouth.
- Position the receptor: Insert the receptor in the holding device and position the receptor as well as receptor holding device in the region of the patient’s oral cavity to be examined. Angle for the receptor holder should be set in the manner that the image receptor is parallel to the occlusal plane. Leading with the apical end of receptor, rotate it into the oral cavity. For maxillary views, place the receptor in the mouth as far from the teeth as possible, near the midline of the palate, where there is the maximal space available. The added space allows the receptor to be oriented parallel to the long axis of the teeth. With the receptor now in the mouth, place it gently on the palate or floor of the mouth. As the sensor is positioned, rotate the receptor holding device until the bite block rests on the teeth to be radiographed and place a cotton roll between the bite block and the opposing teeth. Holding the instrument and receptor in place, ask the patient to close the mouth gently.
Periapical Lesion Radiographic Diagnosis
“Role of paralleling technique in diagnosing periapical lesions: Questions answered”
- Position the x-ray tube: Adjust both vertical and the horizontal angulation of tube head to correspond to the receptor-holding instrument. End of the aiming ring of the x-ray tube head should be flush or parallel to the guide ring instrument. Alignment is satisfactory when the aiming cylinder covers the port and is within the limits of the face shield. Caution the patient not to move.
- Make the exposure: Exposure is made with the preset exposure time. If receptor is a film or storage phosphor plate, remove the receptor from the patient’s mouth after exposure, dry it with a paper towel, remove the infection control sleeve, and place the receptor in an appropriate receptacle outside the exposure area. If the receptor is a CCD or. CMOS sensor, operator may keep it in the patient’s mouth and reposition it for the next view. Ensure patient comfort after each exposure.
Intraoral Radiography
Paralleling Technique Advantage
- Accuracy:
- Image is dimensionally accurate.
- Radiographic image is free of distortion and exhibit maximum detail and definition.
- There is no overlap of related structures.
- Simplicity: The technique is simple and easy to learn and use.
- Duplication: This technique is easy to standardize and can be accurately duplicated or repeated.
- Facial screen can be used.
- There is decreased secondary radiation.
- The relative position of the film, teeth and X-ray beam are always maintained so useful for handicapped and compromised patient.
- Periodontal bone level is well represented.
- Periapical tissues are accurately shown with minimum foreshortening or elongation.
“Early warning signs of issues addressed by intraoral radiography in periapical lesions: Common questions”
Paralleling Technique Disadvantages
- Film placement with film-holding device is difficult in child patient.
- Patient discomfort: The holding device may impinge oral soft tissues and causes discomfort and gagging.
- Object film distance is increased so more chances of image magnification are present.
- The long cone is more spacious.
- Positioning of film is difficult in third molar region.
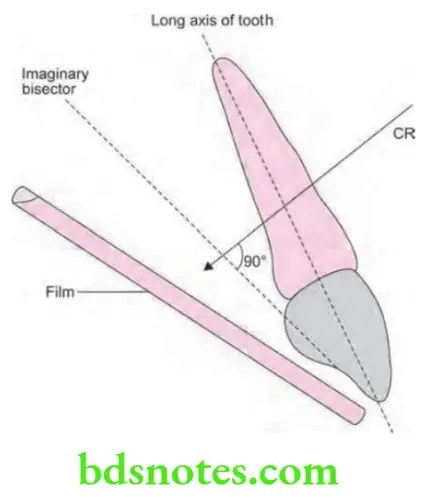
Bisecting Angle Technique
Principle of Angle-bisecting Technique
- Angle bisecting technique is based on the simple geometrical principle known as “Cieszynski’s law of isometry” which states that two triangles are said to be equal when they share one complete side and have two equal angles.
- In dental radiography, the above given law is applied as:
- Film should be positioned close to the lingual surface of teeth, resting on palate or on the floor of mouth.
- Plane of the film along with the long axis of tooth form an angle with its apex at a point where film is in the contact with the teeth.
- When the angle is bisected via the imaginary line two congruent angles with a common side are formed.
- A line which represent the central ray of an X-ray beam complete the third side of two triangles when it is bisected perpendicular to bisecting line.
- This involves in taking the radiographs in the manner that the long axis of rays is perpendicular to bisector between the long axis of tooth and the long axis of film.
- Here an 8 inch cone is used with 55 to 65 kVp.
Bisecting Angle Technique Technique
Film stabilization: In angle bisecting technique, film-holding instruments or the patient’s finger may be use to position and stabilize the film. Various commercially available film holders are Rinn BAI instruments, Stable bite block, EEZEE grip film holder.
Radiographic Features Of Periapical Lesions
Film placement: The film should be positioned to cover the prescribed area of teeth to be examined.
“Asymptomatic vs symptomatic effects of poor communication about periapical lesions: Answered”
Film position: The film must be placed against the lingual surface of the tooth. The occlusal end of the film (indicated by the raised identification mark or dot) must extend approximately 1/8th inch beyond the incisal or occlusal surfaces. The apical end of the film must rest against the palatal or alveolar tissues, if the finger-holding method is used to stabilize the film. The patient must be instructed to press the film gently against the cervical portion (where the crown meets the roots) of the tooth.
Vertical angulation: The central ray of the X-ray beam must be directed perpendicular to the image of the bisector that divides the angle formed by the film and the long axis of the tooth.
Horizontal angulation: The central ray of the X-ray beam must be directed through the contact areas between the teeth.
Film exposure: Center the X-ray beam on the film to ensure that all areas of the film are exposed. Failure to center the X-ray beam results in a partial image on the film or a cone cut.
Intraoral Radiography
Film Stabilization: Film-holding device or the patients finger may be used to position and stabilize the film.
Endodontic Radiographic Examination
Used Film holders
- Rinn BAl (B-bisecting, A-angle, I-instrument).
- Stable bite block.
- EEZEE grip film holder (snap-A-Ray).
“Asymptomatic vs symptomatic effects of ignoring proper intraoral radiographic protocols: Q&A”
“Steps to educate patients about intraoral radiography and its importance: Q&A format”
Bisecting Angle Technique Advantages
- Primary advantage is that it can be used without film holder when the anatomy of patient not allowed use of holder (like in shallow palate bony growth).
- Positioning is reasonably comfortable, simple and quick.
- Decreased exposure time, as a short (8 inch) PID is used.
- Positioning of film packet is comfortable to the patient.
- In the technique, if angulations are assessed properly, there will be no changes in the dimension seen of the tooth which is imaged.
- If angulations are discussed properly, there will be no changes in dimension of tooth which is imaged.
“Early warning signs of knowledge gaps in patient understanding of intraoral radiography: Common questions”
Bisecting Angle Technique Disadvantages
- Image distortion: Due to short PID, there is increase in the divergence of X-rays which causes image magnification.
- Angulation problem: It is difficult for the dental radiologist to visualize the imaginary bisector and determine vertical angulation without the use of film holder and aiming the ring. So if there is any error in the vertical angulation, this causes image distortion.
- Unnecessary exposure: As patient stabilizes the film by their finger, the patient’s hand is unnecessarily exposed to the primary beam of X-ray radiation.
- Incorrect horizontal angulation: This leads to overlapping of the images, while incorrect vertical angulation leads to foreshortening or elongation of the image.
- Periodontal bone levels are poorly represented.
- Shadow of zygomatic bone frequently overlaps the periapical area of maxillary molars.
- Crown of the teeth are often get distorted so detection of proximal caries is difficult.
Intraoral Radiography In Endodontics
“Role of counseling in clarifying intraoral radiographic goals for patients: Questions answered”
Le Master Modification
For maxillary 3rd molar a cotton roll is placed between film and tooth (molar) to make the plane of film more parallel to the tooth plane.
Leave a Reply