Hyperthyroidism – Signs, Causes and Treatment
“What is hyperthyroidism? A detailed question and answers guide”
It occurs most commonly in the elderly patients. It is diagnosed when laboratory findings reveal suppressed TSH levels.
Graves’ Disease Aetiopathogenesis
- The exact aetiological factors responsible for this disease are not clear. The following are considered possible aetiological factors:
- Autoimmune disorder is the first possible cause due to the demonstration of
autoantibodies in the circulation. - Example: TSH receptor antibodies. It can also be associated with other autoimmune disorders like vitiligo.
- Familial: The disease can run in families. Familial/Genetic Graves’ disease has been documented in identical twins.
- Thyroid-stimulating immunoglobulins (TSI) and long-acting thyroid stimulators (LATS) are responsible for pathological changes in the thyroid gland in Graves’ disease.
- Exophthalmos-producing substance (EPS) is responsible for “ophthalmopathy” which is seen in Graves’ disease.
- Female sex, emotions, stress, and young age also have been considered as other factors responsible for the disease.
“Understanding hyperthyroidism through FAQs: Signs, causes, and treatments explained”
Aetiopathogenesis Pathology
- As a result of continuous stimulation, acinar hypertrophy and hyperplasia take place.
- The acinar cells which are normally flat, become tall columnar. The normal colloid disappears and the cells are empty, however, rich vascularity is seen.
- Thus, small follicles with hyperplastic columnar epithelium are characteristic.
Read And Learn More: Clinical Medicine And Surgery Notes
Aetiopathogenesis Clinical features
- Primary thyrotoxicosis is 8 times more common in females than in males, aged around 15– 25 years.
- Symptoms, signs and swelling appear simultaneously.
- Very often young women present with unexplained loss of weight in spite of good appetite. Diarrhoea occurs due to increased smooth muscle activity of small intestines. Intolerance to heat, preference to cold, fine tremors, excitability, hyperkinetic movements, and excessive sweating are the other features. Free steroid hormone levels decrease in Graves’ disease, this results in decreased effective oestrogen at the cell level which in turn causes oligomenorrhoea.
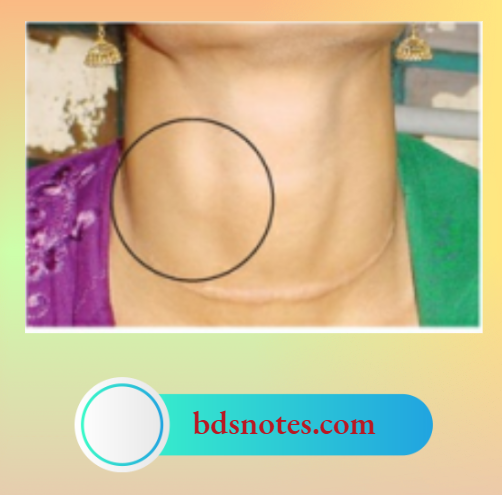
Signs Of Primary Thyrotoxicosis
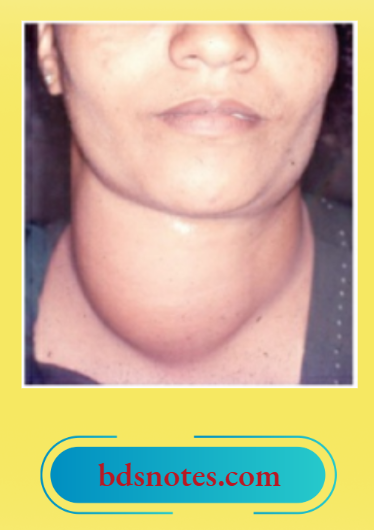
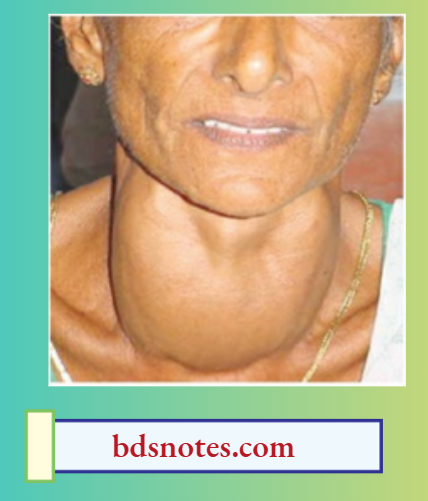
1. Signs of the thyroid gland in Graves’ disease
- Uniformly enlarged (mild degree)
- Smooth surface—no nodules
- The gland is soft or firm in consistency
- Warm and highly vascular
- Auscultation—a bruit is usually heard.
Pulsatile Thyroid Swellings
- Primary thyrotoxicosis
- Secondary thyrotoxicosis
- Follicular carcinoma
- Vascular malformations
2. Central nervous system (CNS) signs
- Tremors of the tongue when the tongue is within the oral cavity and tremors of the outstretched hands are characteristic. A piece of paper may be placed on the fingers in doubtful cases to demonstrate the tremors of the hand. The extensor surface of the hand is used because extensors are weak when compared to flexors.
- Hyperkinetic movements.
- Always a moist, warm hand (shake hands and see).
“How does hyperthyroidism affect the body? FAQ answered”
3. Cardiovascular system (CVS) signs
- The pulse rate is always raised and rapid indicating tachycardia. Depending upon the pulse rate, thyrotoxicosis can be classified as follows: mild—90–100/ minute, moderate—100– 110/minute, severe—more than 110/minute.
- Palpitation and extrasystoles can also be found in primary thyrotoxicosis even though other cardiac features such as atrial fibrillation and cardiac failure are rare.
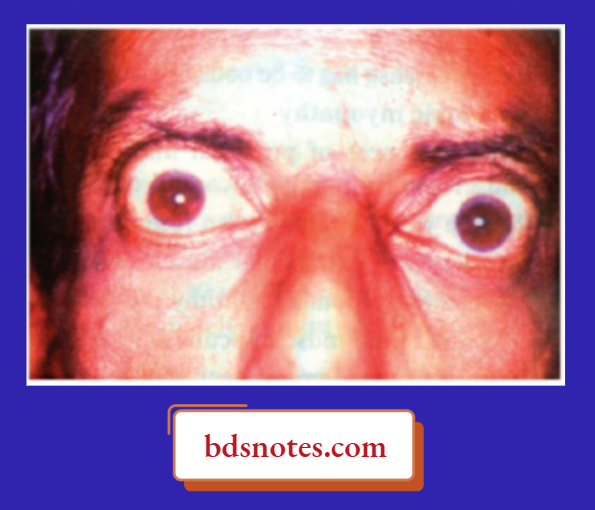
4. Eye signs
- Prominent eyeballs and retraction of the eyelid result in thyrotoxic exophthalmos. This is due to retrobulbar deposition of inflammatory cells, and round cells with venous congestion resulting in oedema.
“Importance of studying hyperthyroidism for medical students: Questions explained”
- The levator palpebrae superioris muscle is innervated by the oculomotor nerve which also carries sympathetic fibres derived from the cavernous plexus supplying the smooth muscle part of the levator. Contraction of this muscle produces lid spasms.
- This is aided by a spasm of Muller’s muscle, a sympathetic muscle which lies on the floor of the orbit. This is responsible for keeping the eyeball forward. All these factors together produce a classical stare.
1. Assessment of exophthalmos
- When upper sclera is seen above the limbus (upper margin of iris and cornea) —
Dalrymple’s sign. - Naffziger’s method: Stand behind the patient and look at the superciliary arch, by tilting the patient’s head backwards. In normal cases, the eyeball is not seen. In cases of exophthalmos, the eyeball is protruded outside.
2. Moebius sign
- Loss of convergence of eyeball. Occurs due to muscle paresis as a part of thyrotoxic ophthalmoplegia.
3. Stellwag’s sign
- Infrequent blinking and widening of the palpebral fissures are due to spasms of sympathetic fibres in the levator palpebrae superioris.
4. Joffroy’s sign
- Absence of wrinkling of the forehead when the patient is asked to look upwards. This occurs due to an increase in the field of vision due to exophthalmos.
5. Von Graefe’s sign (lid lag sign)
- When the patient is asked to look up and down, the upper eyelid cannot cope with the speed of the movement of the finger because of the lid spasm. Hence, the lid lags behind.
Thyrotoxic Exophthalmos
- Proptosis and lid retraction result in exophthalmos
- The sclera is visible beyond the limbus
- Naffziger’s method to examine
- Staring look
- Typically seen in Graves’ disease
- Rarely seen in secondary thyrotoxicosis
“Common challenges in mastering hyperthyroidism notes effectively: FAQs provided”
Malignant Exophthalmos
- This occurs in untreated cases of Graves’ disease.
- If the disease continues, infrequent blinking secondary to exophthalmos results in constant exposure of the cornea to the atmosphere.
- This results in keratitis, corneal ulcer, and conjunctivitis, Chemosis can occur and may even lead to blindness. This is called malignant exophthalmos.
- Malignant exophthalmos is probably due to autoimmune disease.
- In late stages, optic nerve damage and blindness can occur.
Grading Of Thyroid Eye Diseases
- Grade 0: No signs or symptoms
- Grade 1: Only signs, no symptoms
- Grade 2: Soft tissue involvement
- Grade 3: Proptosis
- Grade 4: Extraocular muscle involvement
- Grade 5: Corneal involvement
- Grade 6: Loss of vision with optic nerve atrophy
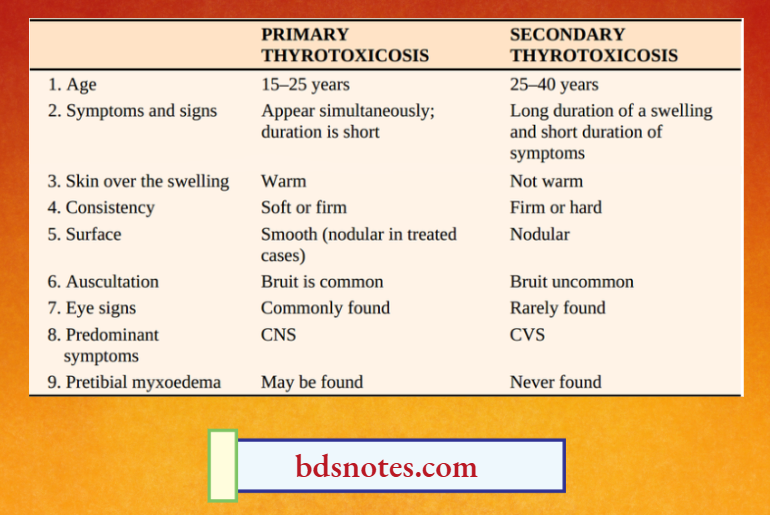
Comparison of primary thyrotoxicosis and secondary thyrotoxicosis
Treatment Of Thyrotoxic Ophthalmopathy
- Massive doses of steroids – oral prednisolone and metronidazole
- Lateral tarsorrhaphy
- Orbital decompression may be necessary in late cases.
- Guanethidine eye drops are useful to decrease lid spasm and lid retraction
- Primary disease has to be controlled
- Head end elevation
- Protect the eye with dark glasses and use diuretics to decrease periorbital and retrobulbar oedema.
4. Thyrotoxic myopathy
- Mild weakness of proximal limb muscles is common. On careful questioning, the patient may admit difficulty in climbing steps.
- Weakness of extraocular muscles results in double vision (diplopia).
- Myopathy responds to antithyroid treatment.
- Proximal limb muscles, ocular muscles, and frontalis are commonly involved (weakness of muscle).
- Features suggestive of myasthenia gravis, and periodic paralysis can be found.
5. Pretibial myxoedema¹ is seen in thyrotoxicosis patients treated with surgery or antithyroid drugs. It is always associated with exophthalmos.
“Why is early detection of hyperthyroidism critical for thyroid health? Answered”
Few Misnomers
- Pretibial myxoedema – Not seen in myxoedema
- Mycosis fungoides – Not a fungal infection
- White bile – Not white, not bile
- Adenolymphoma – Not a lymphoma
- Sternomastoid tumour – Not a tumour
- Malignant hydatid – Not malignant
“Factors influencing success with hyperthyroidism studies: Q&A”
- Bilateral symmetrical deposition of myxomatous tissue mainly in the pretibial region, may also affect the foot and ankle, sometimes the entire leg below the knee. Skin is dry and coarse (thickening of skin by mucin—like deposits).
- Pretibial myxoedema is non-pitting in nature and may be associated with clubbing of fingers and toes called thyroid acropachy
Skin Changes
- Pretibial myxoedema
- Pruritis
- Palmar erythema
- Thinning of hair
Management Of Primary Thyrotoxicosis Investigations
- Routine investigations such as complete blood picture, fasting and postprandial blood sugar estimation, urine examination, and chest X-ray including neck and indirect laryngoscopy are done.
- A thyroid scan will show a warm gland (findings are already discussed).
- Serum T3, T4 and TSH estimation is done. The T3 or T4 levels are high with low levels of TSH. The normal level of T3 is 1.3–3.5 nanomoles/litre and the normal level of T4 is 55–150 nanomoles/litre.
- Thyroid antibodies are elevated.
- The sleeping pulse rate is counted after the patient is sedated with 30 mg of phenobarbitone.
- In the case of toxic goitre, the pulse rate remains high even during sleep because of increased metabolism. This is a simple bedside investigation in cases of toxic goitre.
- In anxiety states, the pulse rate may be high in the morning hours and it comes back to normal during sleep
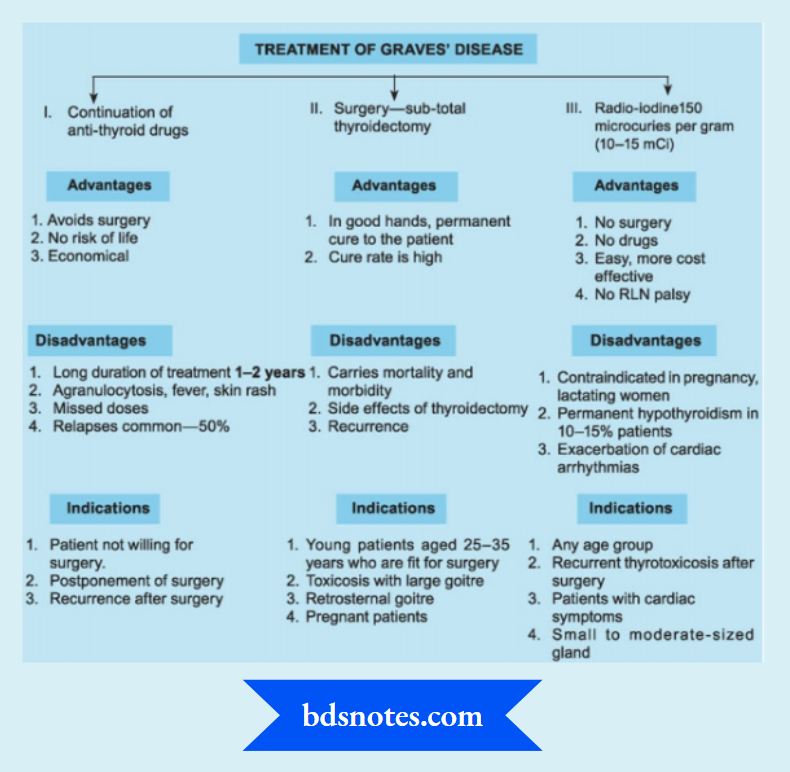
Treatment of Primary Thyrotoxicosis
Aim of treatment
- To restore the patients to a euthyroid state.
- To reduce the functioning thyroid mass to a very critical level (about 6–8 g of thyroid tissue).
- To minimise complications.
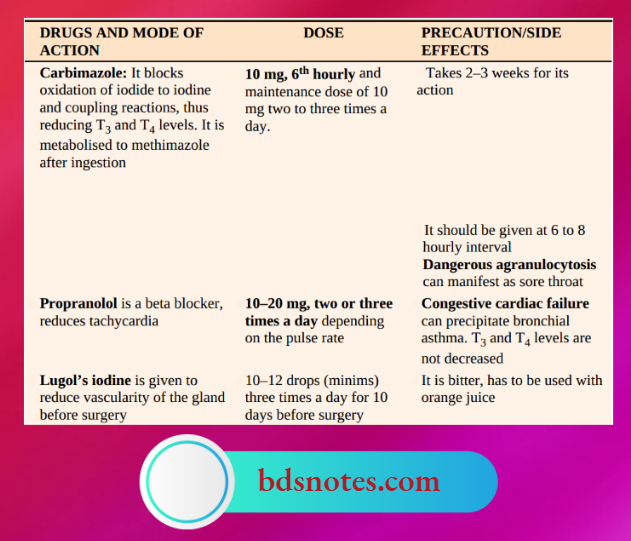
1. To restore the patient to an euthyroid state.
“Steps to explain signs of hyperthyroidism: Weight loss vs palpitations vs heat intolerance: Q&A guide”
- Other drugs such as potassium Perchlorate are given in a dose of 200 mg three times a day. The maintenance dose is 200–400 mg daily. Propyl thiouracil in the dose of 200 mg three times a day can also be given in patients who develop neutropenia due to Carbimazole.
Please note
- Iodine-containing antiarrhythmic drug amiodarone may worsen thyrotoxicosis.
- Propyl thiouracil is safe in pregnancy with Graves’ disease.
- The role of Lugol’s iodine is doubtful.
- Antithyroid drugs will not cure the disease. In selected patients (30 to 40%) remission is possible with regular intake of drugs. They may be continued for a maximum period of 2 years. If toxicity persists or if it occurs on stopping drugs, surgery is recommended. However, the majority of the patients ultimately require surgery or radio-iodine.
Block And Replace Treatment
If a small dose of T3 (20 mg up to 4 times/ day) or T4 (0.1mg/day) is given along with antithyroid drugs, there is less incidence of development of hypothyroidism and an increase in the size of the goitre.
2. To reduce the functioning thyroid mass
- Subtotal thyroidectomy: In this procedure, the thyroid gland is removed for a nontoxic multinodular goitre. However, being a toxic goitre, very little gland should be left behind so as to avoid persistent toxicity in the postoperative period. It is recommended that at least 6–8 gm of thyroid tissue be left behind. This is difficult to measure. Hence, some surgeons advocate leaving thyroid tissue as small as the tip of the little finger, on each side.
- Radio-iodine therapy1: This is a suitable alternative to surgery in cases of primary thyrotoxicosis in patients above the age of 40
Radio-Iodine Therapy
- Today there is ‘No Restriction Of Age And Sex’
- Absolute contraindication is pregnancy
- To avoid conception for a period of 4 months after radio-iodine therapy
To minimise complications
- Good preoperative preparation of the patient, good anaesthetic and surgical techniques and good postoperative care will reduce the complications of surgery.
Thus, antithyroid drugs, subtotal thyroidectomy and radio-iodine therapy are the three different modalities available for the treatment of primary thyrotoxicosis. The indications, merits, and demerits of each treatment.
Treatment of Secondary Thyrotoxicosis
- Patients with severe cardiac damage entirely or partly due to hyperthyroidism are middle-aged or elderly with secondary thyrotoxicosis and the hyperthyroidism is not very severe.
- These patients develop atrial fibrillation and cardiac failure if left untreated. In elderly patients, when the operative risk is unacceptable, radio-iodine is given.
- Treatment with antithyroid drugs is started 48 hours later and continued until radio-iodine has had its effect (6 weeks).
- If the cardiac symptoms are controlled well and anaesthesia risk is acceptable, subtotal thyroidectomy is done. However, the gland that is left behind should be equal to the terminal phalanx of the thumb of the patient.
“Role of weight loss in identifying hyperthyroidism: Questions answered”
Some Specific Toxic Thyroid Conditions
Thyrotoxicosis in children
Initially, antithyroid drugs are given for 10–15 years followed by surgery.
- Radioiodine is absolutely contraindicated as there is a fear of carcinoma developing at a later date.
Thyrocardiac
It refers to a condition wherein cardiac damage has resulted due to hyperthyroidism.
- Classically, it happens in secondary thyrotoxicosis usually seen in middle-aged or old-aged patients
Secondary Thyrotoxicosis Effect On CVS
- Tachycardia
- Wide pulse pressure
- Extrasystoles
- Atrial fibrillation
- Cardiac failure

“How does heat intolerance indicate thyroid dysfunction? FAQ explained”
- Propranolol controls the disease very well.
- Radioiodine therapy is the treatment of choice.
Hyperthyroidism In Pregnancy
- Invariably, it is Graves’ disease.
- In the first trimester surgery and radio-iodine are contraindicated. The smallest dose of Carbimazole or propyl thiouracil can be used with fetal monitoring (both TSH and antithyroid drugs cross the placenta).
- Surgery, if necessary can be done in 2nd trimester.
Apathetic Thyrotoxicosis
Thyrotoxicosis in the elderly wherein pulse rate is low, they appear hypothyroid rather than hyperthyroid.
Neoplastic Goitre Adenoma
- The benign tumours of the thyroid gland are not uncommon. They present as a solitary nodule, thus causing worry to the clinician. Adenomas are of follicular type.
- The diagnosis is established by histological examination.
- Adenomas are treated by hemithyroidectomy/lobectomy.
- However, FNAC cannot distinguish between a follicular adenoma and follicular carcinoma.
- Hence a frozen section has to be arranged.
Malignant Tumours¹
- The thyroid is the only endocrine gland wherein malignant tumours are easily accessible for clinical examination.
- The thyroid is the only endocrine gland wherein malignant tumours occur in children, young age, middle age, old age and in both sexes.
- The thyroid is the only endocrine gland wherein malignant tumours are spread by all possible routes —local, lymphatic and blood spread.
- The thyroid is the only endocrine gland wherein malignant tumours are usually non-functional.
Malignant tumours of the thyroid are common. They are interesting tumours, having good prognosis if diagnosed early.
Papillary and follicular carcinoma are well differentiated, medullary carcinoma are moderately differentiated and anaplastic carcinomas are poorly differentiated.
Thyroid Malignancy Incidence
- Papillary carcinoma 60–65%
- Follicular carcinoma 15–20%
- Anaplastic carcinoma 10–12%
- Medullary carcinoma 5–10%
- Others 10%
Papillary Carcinoma
Aetiology
- Irradiation to the neck during childhood.
- Radiotherapy given for benign conditions such as acne in teenagers or enlarged tonsils or thymus gland in children increases the risk.
- Low-dose therapeutic radiation (6.8–2000 cGy) in infancy or childhood is associated with an increased incidence of thyroid cancer (about 10%).
- It can be a complication of Hashimoto’s thyroiditis.
- Syndromes
- Papillary thyroid cancer occurs more often in patients with Cowden’s syndrome,
Gardner’s syndrome or Carney’s syndrome.
- Papillary thyroid cancer occurs more often in patients with Cowden’s syndrome,
“Early warning signs of gaps in understanding hyperthyroidism symptoms: Common questions”
Neck radiation increases the risk not only for carcinoma thyroid but also for parotid gland tumours and hyperparathyroidism.
Pathology
It is made up of colloid-filled follicles with papillary projections. In some cases (60%), calcified lesions are found which are called psammoma bodies. These are diagnostic of papillary carcinoma of the thyroid.
Characteristic pale, empty, nuclei are present in a few cases which are described as Orphan Annie eyed nuclei. Tumour spreads via intraglandular lymphatic plexus within the gland and then to the subcapsular and pericapsular lymph nodes. Papillary carcinoma can be unifocal or multifocal.
“Asymptomatic vs symptomatic effects of ignoring hyperthyroidism principles: Q&A”
- Papillary microcarcinoma: They measure 1 cm or less in diameter. Distant metastasis is extremely rare. Hence, a simple hemithyroidectomy is the treatment of choice.
- Follicular variant of papillary cancer: This is a mixed lesion with a predominance of follicles over papillae. They are treated by near-total thyroidectomy.
- Tall cell papillary cancer: This is an aggressive tumour, rapidly growing, occurs in elderly patients and should be treated by near-total thyroidectomy.
Clinical Presentation
- Young females are commonly affected (at the age of 20–40 years).
- It can present as a solitary nodule.
- Very often, the lymph nodes in the lower deep cervical region are involved and the thyroid may or may not be palpable. When the thyroid gland is not palpable, it is called occult (hidden).
- However, papillary carcinoma less than 1.5 cm in diameter is also called “occult”.
- A few patients present late to the hospital with fixed nodes in the neck, and fixed thyroid to the trachea with or without recurrent laryngeal nerve paralysis.




“Can targeted interventions reduce risks of complications? FAQs provided”
“It should be noted that papillary carcinoma can be offered as a clinical diagnosis only in the presence of significant lymph nodes in the neck along with a thyroid swelling.”
Prognostic Criteria
There are many prognostic criteria that have been used in cases of well-differentiated carcinoma. They are helpful in explaining the prognosis to the patient and relatives.
Ages Criteria Investigations
- All routine investigations such as blood examination, chest X-ray, and laryngoscopy have to be done. A large mediastinal shadow suggests mediastinal nodes.
- Ultrasound of the neck is the first investigation of choice in the majority of thyroid swellings.
- Here it can pick up a solid nodule, and lymph nodes and it can guide fine needle aspiration cytology (FNAC) of the nodule. A thyroid scan may demonstrate a cold nodule (Not routinely done nowadays).
- Fine Needle Aspiration Cytology (FNAC) can demonstrate colloid-filled follicles with a papillary process. Thus, preoperative diagnosis of papillary carcinoma is possible with FNAC. If the lymph nodes are enlarged, FNAC can be taken from the lymph nodes.
Risk Group Stratification In Differentiated Thyroid Carcinomas (Ages)
Low-Risk- High risk
- Age Women younger than 50 years > 50 years Men < 40 years > 40 years
- Grade Well differentiated Poorly differentiated (fibrous, insular, mucoid, tall variant)
- Extent Confined to thyroid Invasive to adjacent tissues or distant metastasis
- Size Diameter < 4 cm > 4 cm diameter
Papillary Carcinoma Treatment
It can be Discussed Under 3 Headings. Treatment Of The Primary, Treatment Of The Secondaries In The Lymph Nodes And Suppression Of Tsh.
1. Treatment of the primary—Total or Near-total thyroidectomy
- Total thyroidectomy is the most ideal surgery for thyroid carcinomas. However, in an attempt to preserve recurrent laryngeal nerve and parathyroid glands, small amounts of thyroid tissue are usually left behind, which amounts to or is called near-total thyroidectomy.
- (Lobectomy on the side of the lesion and a subtotal on the opposite side.) The purpose of the surgery is to preserve at least one recurrent laryngeal nerve and one parathyroid gland and at the same time, remove the primary.
- If FNAC is inconclusive, a hemithyroidectomy specimen or a good portion of the diseased lobe is sent for a frozen section. If a frozen section is reported as malignant, near-total thyroidectomy is completed If clinically strong suspicion is present, one need not wait for a frozen section, a total thyroidectomy is done.
- Histological surprise: If a subtotal thyroidectomy is reported as papillary carcinoma of the thyroid, re-exploration and completion of thyroidectomy should be done after explaining the high risks of recurrent laryngeal nerve palsy and hypocalcaemia.
After total thyroidectomy, thyroxine is not given for a period of 6 weeks so that thyroid remnants can be ablated with radioiodine—30-100 mCi.
2. Treatment of secondaries in the lymph nodes
- Lymph node secondaries are treated by functional block dissection. (Berry picking means removal of enlarged lymph nodes only. It is no longer followed).
- Other structures such as the internal jugular vein, sterno-mastoid muscle etc are not removed because lymph nodes are slow growing and they rarely spread/outside the capsule of the lymph node.
- Lateral aberrant thyroid: Initially was thought to be thyroid tissue. However, it is metastasis into Level 3 and 4 lymph nodes from papillary carcinoma thyroid.
- No role for prophylactic neck dissection except in children.
3. Suppression of the TSH
This is an important aspect in the postoperative period because papillary carcinoma is a TSH-dependent tumour.
To prevent the patient from developing hypothyroidism in the postoperative period and to suppress TSH, thyroxine is 0.3 mg/day.
“Differential applications of traditional vs modern diagnostic tools: Questions answered”
Hyperparathyroidism—A Disease Of
- Bones
- Stones
- Abdominal groans
- Psychic moans
3. Abdominal groans
- Calcium stimulates gastrin which is the powerful stimulator of acid. This may result in pain abdomen due to peptic ulcer. The patient can present with dyspeptic symptoms.
- Calcium can cause pancreatitis, resulting in pain radiating to the back.
- Metastatic calcification is also a feature.
4. Psychiatric moans
- These patients, more often a woman, mostly of middle age, having bony pains, backaches and behavioural abnormalities are thought to have a psychiatric illness.
- They are referred to mental institutions, orthopaedic departments, and gynaecology departments and are shunted from doctor to doctor.
Other Features
- Corneal calcification/band keratopathy may be seen in the eye on slit lamp examination.
- Proximal myopathy and muscle wasting are also seen.
- Interestingly, clinical examination of the neck may not reveal any parathyroid enlargement. Hence, the diagnosis should be suspected by the various symptoms.
- A high index of suspicion is necessary in arriving at a proper diagnosis.
Causes Of Hypercalcaemia
- Multiple bone secondaries1
- Multiple myeloma
- Hyperparathyroidism
- Oat cell carcinoma2
- Sarcoidosis
- Vitamin D intoxication
Investigations
It can be classified into:
1. To prove hyperparathyroidism
- Serum calcium, phosphate, albumin
- Serum PTH assay
- Alkaline phosphatase
- X-ray of bones
2. To localise parathyroid glands
- Ultrasound of neck
- Thallium and technetium subtraction scan
- Selective venous sampling with PTH assay is the most reliable but more difficult.
- Sestamibi scanning.
“Steps to explain treatment of hyperthyroidism: Antithyroid medications vs radioactive iodine vs surgery: Q&A guide”
1. To prove hyperparathyroidism
- Serum calcium levels are always raised above normal limits (9–11 mg %). There are many causes of hypercalcaemia which are depicted. Hence, the estimation of serum calcium alone will not give the diagnosis.
- Albumin is the main calcium-binding protein in the plasma, hence it also should be measured.
- Serum PTH level which is estimated by immunoassay is the diagnostic investigation. It is called a tumour marker for hyperparathyroidism. Estimation of PTH is difficult, costly and needs a sophisticated setup.
- Serum phosphorus levels are decreased.
- Alkaline phosphatase is increased when bones are involved.
- X-ray of the hand may reveal decalcification cysts in the phalanges, telescoping of fingertips, etc.
- X-ray of the skull may reveal subperiosteal erosions, a hazy outline of the skull with a pepper-pot appearance.
Interesting Radiological Changes
- Osteopenia
- Bone density loss
- Bone cysts and brown tumours
- Aggregation of osteoclasts Osteoclastoma)
- Rugger jersey spine
- Generalised loss of bone density
- Pepper pot skull
- Demineralised bone
- Subperiosteal resorption (Pathognomonic)
- Seen in the radial aspect of the middle phalanges in the hand and clavicle
2. To Localise Parathyroid Glands
- Ultrasound of the neck can be very accurate in the hands of an experienced sonologist. It can also detect renal disease, pancreatic disease, etc. It cannot scan behind the sternum and cannot pick up lesions less than 0.5 cm.
- Thallium-technetium isotope scan: First outline thyroid with 99mTc and then isotope 201TiCI (thallium chloride) is administered which is taken up by both thyroid and parathyroid. By computer subtraction of the two and enlargement of images, the parathyroid appears as a hot spot.
- Sestamibi scanning: This test has been proven to be superior to Thallium and technetium subtraction scanning.
- Sestamibi is a protein labelled with technetium-99m that localises diseased glands.
- It is very sensitive to identify adenomas (90%) than hyperplasia.
- However, it is very expensive. Hence, it can be used in the re-exploration of the neck for parathyroidectomy.
To Localise Parathyroid Glands Treatment
- The surgery of the parathyroid glands needs patience, skill and expertise. The neck is explored with a collar neck incision similar to subtotal thyroidectomy. The parathyroid gland, when it is enlarged can have dark-brown or chocolate-brown colour.
- Occasionally, the surgeon is lucky to encounter a single adenoma usually located on the posterior surface of the thyroid gland, when it arises from the superior parathyroid.
- Very often, the identification of the parathyroid may be difficult because they may be intrathyroidal or within the mediastinum.
- A frozen section of parathyroid glands is essential to confirm whether it is an adenoma or hyperplasia because depending upon the pathological nature of the gland, the treatment has to be carried out
Following are a few examples of types of surgery
- Single adenoma: Excision of the gland. However, one other normal parathyroid gland is also removed for histopathological study.
- Diffuse hyperplasia: 3½ or 3¾ parathyroids are removed and a small piece is autotransplanted into the forearm muscle tissue.
- In case there is hyperactivity of this parathyroid tissue, surgical exploration becomes easy. At the same time, if this functions normally, the patient will not develop hypoparathyroidism.
- Carcinoma: All four glands should be removed along with thyroid tissue.
“Role of methimazole in managing hyperthyroidism: Questions answered”
Follow-Up
- Estimation of calcium should be done in the postoperative period to assess the functioning of the parathyroid tissue.
- Very often, after surgery for adenoma, there is a sudden drop in the levels of calcium because of the absorption of calcium by the bones.
- This is described as hungry bone syndrome. This is seen in patients who have generalised bone disease.
- In one of our patients, calcium levels dropped down to 4 mg % with severe tetany. It took 7–10 days for the calcium to return to normal levels. She required around a clock constant calcium drip.
- Absorption of calcium can be enhanced by oral administration of 1, 25 – dihydroxycholecalciferol, which is the metabolite of vitamin D.




“Early warning signs of undiagnosed treatment needs: Common questions”
Unusual Locations Of Parathyroids At Surgery
- Behind oesophagus
- Within carotid sheath
- Intrathyroidal
- Upper mediastinum
Acute Hypercalcaemic Crisis
It presents with severe abdominal pain and effortless vomiting. Dehydration, oliguria, and renal failure follow soon. Untreated cases develop coma and cardiac arrest.
Acute Hypercalcaemic Crisis Causes
- Hyperparathyroidism
- Sudden increases in PTH levels occur due to spontaneous bleeding in a parathyroid tumour or rupture of a cystic parathyroid tumour.
- Severe dehydration also precipitates a crisis
- Disseminated carcinoma with bony metastasis (usually carcinoma of the breast).
Acute Hypercalcaemic Crisis Treatment
- Restore fluid volume urgently
- The biphosphonates–Disodium pamidronate slow intravenous 15–60 mg single infusion or over 2–4 days. Maximum dose is about 90 mg. This drug stops the mobilization of calcium from the bone.
- Mithramycin
- Steroids (in cases of vitamin D intoxication and sarcoidosis).
“Asymptomatic vs symptomatic effects of delayed clinical interventions: Answered”
Types Of Hyperparathyroidism
- Primary hyperparathyroidism: It refers to the hyperactivity of parathyroids due to an adenoma or primary hyperplasia of parathyroid glands.
- Secondary hyperparathyroidism: It occurs due to persistently low levels of calcium as in chronic renal failure and malabsorption, which results in decreased levels of calcium which in turn stimulates the parathyroid gland.
- Tertiary hyperparathyroidism: This is seen in patients who undergo dialysis and transplantation for chronic renal failure. After a few years, autonomy develops and secondary hyperparathyroidism changes into tertiary hyperparathyroidism.
Leave a Reply