Herpes Virus
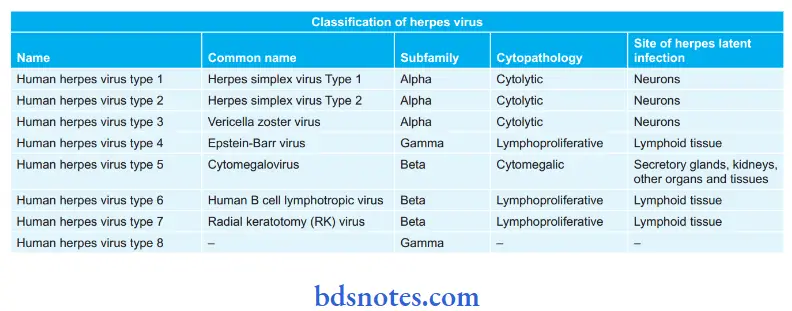
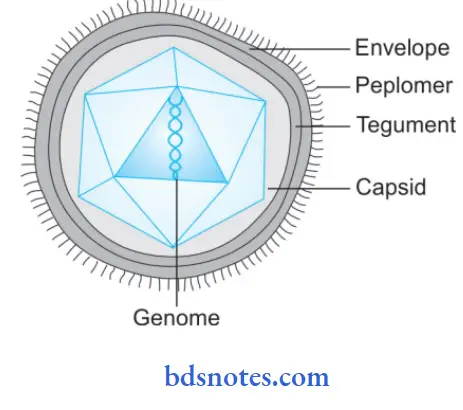
Question 1. Enumerate, classify, and draw a schematic labeled diagram of the herpes virus.
Answer:
See the table classification of herpes virus:
“Importance of studying herpes viruses for medical students: Questions explained”
“Understanding herpes viruses through FAQs: Q&A explained”
Read And Learn More: Microbiology Question And Answers
Question 2. Write about laboratory diagnosis of herpes virus infections.
Answer:
Herpes Virus Infections Specimens Collected
- Vesicle fluid
- Skin swab
- Corneal scrapings
- Throat swab
- Saliva
- CSF
- Brain biopsy
“Common challenges in understanding herpes viruses effectively: FAQs provided”
Herpes Virus Infections Microscopic Examination
- Tzanck smear: It is a rapid, sensitive, and inexpensive diagnostic method. Smears are prepared from the lesions, preferably from the base of vesicles, and stained with 1% aqueous solution of toluidine blue for 0 to 15 seconds. Multinucleated cells with faceted nuclei and homogeneously ‘ground glass’ chromatin (Tzanck cells) constitute the positive smear.
- Giemsa’s stain: It demonstrates intranuclear inclusion bodies in smear.
- Electron microscopy: It demonstrates virus particles in the smear.
- Direct immunofluorescence test: It demonstrates viral antigens in smears.
- Fluorescent antibody test by using brain biopsy material: It is used for rapid diagnosis of encephalitis.
Herpes Virus Infections Virus Isolation
- Tissue culture is the method of choice used for virus isolation.
- The specimen should be inoculated on tissue culture.
- The appearance of typical CPE in cell culture under 2 or 3 days is indicative of the presence of the herpes virus.
- Viral agents should be identified by neutralization test or immunofluorescence test along with specific sera.
- The difference between HSV-1 and HSV-2 is done by using specific antisera.
“Factors influencing success with herpes virus knowledge: Q&A”
Herpes Virus Infections Serological Test
- Serological methods are useful in the diagnosis of primary infections.
- Antibodies develop within a few days of infection, and a rise in the titer of antibodies is seen in 2 to 4 weeks.
- In recurrent or reinfection herpes, there may be little change in the antibody titer.
- Antibodies can be measured by ELISA, radioimmunoassay, immunofluorescence test neutralization, or complement fixation tests.
- Serological methods are not widely used as their diagnostic value is less.
Question 3. Describe salient features of pathogenecity related to herpes simplex and varicella zoster virus.
Answer:
Pathogenecity Related to Herpes Simplex:
- Herpes simplex is one of the common viral infections in humans, with about 60-90% of adults showing detectable antibodies.
- Primary infection is usually acquired in early childhood, between 2 and 5 years of age.
- Humans are the only natural hosts and the sources of infection are saliva, skin lesions, or respiratory secretions.
- Asymptomatic carriers form the more important source of infection, especially in genital infection with type 2 strains.
- Transmission occurs by close contact and may be venereal in genital herpes.
- The virus enters through defects in the skin or mucous membranes and multiplies locally with cell-to-cell spread.
- The virus enters cutaneous nerve fibers and is transported intra-axonally to the ganglia, where it replicates.
“Early warning signs of gaps in understanding herpes basics: Common questions”
- Centrifugal migration of the virus can take place from the ganglia to the skin and mucosa to cause cutaneous and mucosal lesions.
- The virus remains latent in the ganglia, particularly in the trigeminal (HSV type 1) and sacral (HSV type 2) nerves, to be reactivated periodically in some individuals, causing recurrent oral and genital lesions.
- Antibodies may not prevent recurrences, but can reduce the severity of clinical disease. Cell-mediated immunity is more important in resistance to and recovery from herpes simplex infections.
- Herpes virus diseases are more frequent and severe in HIV-infected and other immunodeficient subjects.
“Steps to explain types of herpes viruses: HSV-1 vs HSV-2 vs VZV vs CMV vs EBV: Q&A guide”
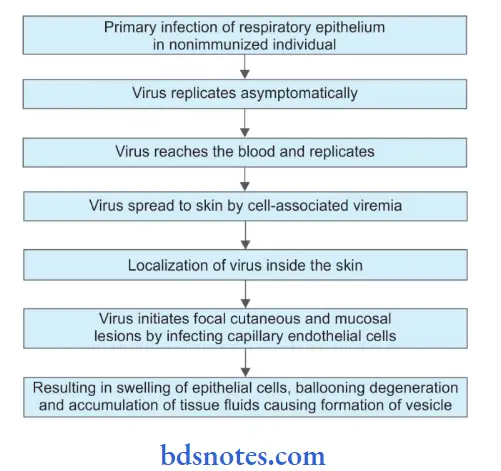
Pathogenecity Related to Varicella-Zoster
- Varicella (Chickenpox) and herpes zoster (Shingles) are caused by a single virus, which it is named a varicella-zoster virus.
- Chickenpox follows primary infection in a non-immune individual, while herpes zoster is the reactivation of the latent virus when immunity falls to an ineffective level.
In Children:
“Role of latency in herpes virus infections: Questions answered”
In Old Age:
In persons who had chickenpox earlier, the virus remains latent in the sensory ganglia. The virus is held in check by residual immunity. Years after, when immunity falls, the virus may get reactivated and triggered by some precipitating stimulus.
Leave a Reply