Furcation Involvement And Its Management
Write short note on classification of furcation involvement.
Or
Describe and classify furcation involvement.
Or
Describe and classify furcation involvement. Write in detail on various treatment modalities.
Or
Define furcation involvement and classify. Write in detail the etiology and treatment of furcation.
Or
Define, classify, write clinical features, radiographic features and treatment of furcation involvement.
Or
Write short note on classification of furcation.
Or
Explain management of periodontal furcation involvement.
Answer. Definition: “Furcation involvement refer to invasion of bifurcation and trifurcation of multirooted teeth by periodontal disease.”
Classification of Furcation Involvement
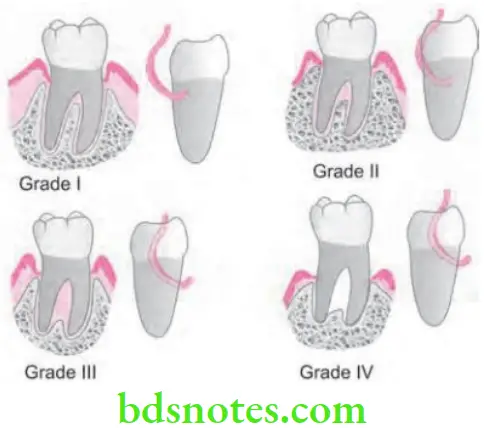
Glickman’s Classification
- Grade 1: It is the incipient or early lesion. The pocket is suprabony involving soft tissue.
- Slight bone loss
- No radiographic changes.
- Grade 2: Inter-radicular bone is destroyed.
- Partial penetration of probe into the furcation.
- The lesion is essentially a cul-de-sac.
- Radiography may or may not reveal.
“Understanding the role of furcation involvement in periodontal disease”
- Grade 3: Complete loss of inter-radicular bone. Not seen clinically because facial and lingual surfaces are included by gingival tissues. There is through and through tunnel is present. Lesion will appear as a radiolucent area between the roots.
- Grade 4: In grade 3 lesions, the inter-radicular bone is completely lost, but in grade IV-involvement the gingival tissues recede apically so that furcation opening is visible clinically. Radiographic changes are same as of grade 3 lesion.
“Importance of studying furcation involvement for dental professionals”

“Common challenges in diagnosing furcation involvement”
Read And Learn More: Periodontics Question And Answers
“Steps to classify furcation involvement using Glickman’s classification”
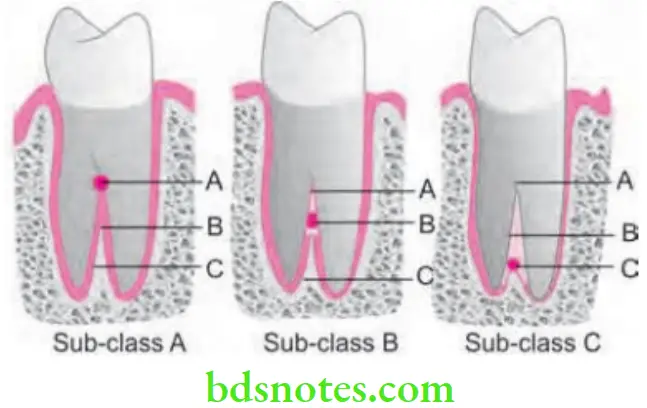
According to Tarrow and Fletcher
- Sub-class A: Vertical destruction of bone to one-third of the total inter-radicular height (1–3 mm).
- Sub-class B: Vertical destruction of bone reaching two-third of inter-radicular height (4–6 mm).
- Sub-class C: Vertical destruction beyond the apical third (> 7 mm).
“Role of Grade I, II, and III furcation involvement in treatment planning”
“Early warning signs of untreated furcation involvement”
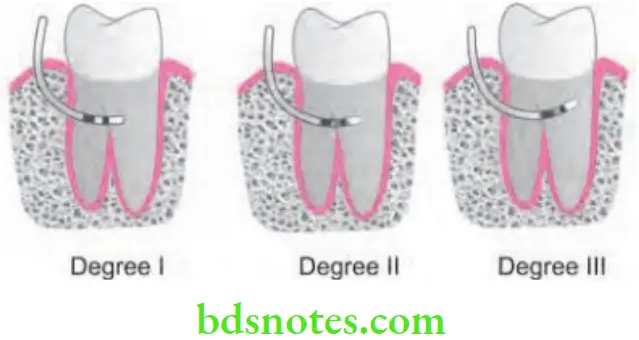
According to Hamp and Co-workers
- Degree 1: Horizontal bone loss of less than 3 mm.
- Degree 2: Horizontal bone loss of more than 3 mm.
- Degree 3: Through and through horizontal incision.
“Asymptomatic vs symptomatic stages of furcation defect progression”
Etiology of Furcation Involvement
- Primary factor
- Bacterial plaque: It is the most common cause of marginal periodontitis, which invades one or more furcation areas to varying degrees which results in irreversible bone loss in inter-radicular area.
- Local anatomical factors
- Root trunk length: It is a key factor that affects the development and treatment of furcation involvement. Teeth with shorter root trunk lead to early furcation involvement and has long roots that support the tooth and potentiate corrective therapy. Teeth with longer root trunk are less likely to develop furcation involvement, but as the furcation is developed these teeth have poor prognosis due to the presence of short roots.
- Root length: It is directly related to the quantity of attachment supporting the tooth. Teeth having long root trunks as well as short roots may have lost a majority of their support by the time furcation becomes affected.
“Differential applications of maxillary vs mandibular furcation involvement”
- Root form: Mesial root of mandibular molars and mesiobuccal roots of maxillary first molars consists of deep concavities, this affects the complete plaque removal which results in persistence of periodontal pockets and furcation involvement.
- Inter-radicular dimensions: Degree of separation of the roots is also an important factor in treatment planning. Closely approximated or fused roots preclude adequate instrumentation during scaling, root planning, and surgery. Teeth with widely separated roots present more treatment options and are more readily treated. The dimensions of furcation entrance should be taken into consideration at the time of selection of instruments.
- Cervical enamel projections (CEJ): It is an apical extension of enamel into the furcation area of a multirooted tooth. It is covered by the junctional epithelium instead of connective tissue attachment which predisposes to periodontal defect in the furcation area.
- Enamel pearls: It is an isolated small focal mass of enamel formed apical to the CEJ. Closer is the enamel pearl to CEJ, greater is the chance of periodontal breakdown.
- Complicating factors
- Accessory pulp canals: Presence of accessory canals in the furcation area of a multirooted tooth may provide an access to the products of pulpal necrosis resulting in resorption of inter-radicular bone and furcation involvement.
- Trauma from occlusion: Occlusal interferences may predispose to inter-radicular bone loss and further complicate furcation involvement when superimposed on an existing inflammation.
- Iatrogenic factors: Presence of overhanging subgingival margins and over contoured restorations can contribute to the progressive destruction of periodontium which extend into the furcation area.
“Steps to treat furcation involvement with regenerative techniques”
Furcation Involvement Clinical Features
- Mandibular first molars are the most common sites and maxillary premolars are the least common.
- Denuded furcation may be visible clinically or covered by the wall of the pocket.
- Associated with suprabony and infrabony pockets.
- Periodontal abscess.
- Root caries and tooth mobility are common.
Furcation Involvement Radiographic Features
- Grade 1: Radiographic changes are not usually found.
- Grade 2: Radiographs may or may not depict the furcation involvement.
- Grade 3: Shows a radiolucent area in the crutch of the tooth.
- Grade 4: Seen as a radiolucent area.
Treatment/Management of Furcation Involvement
Class 1 Furcation Defects
- Furcation plasty: In furcation plasty there is raising of mucoperiosteal flap to provide access to the furcation area and combining scaling and root planning, osteoplasty and odontoplasty to remove local irritants and to open the furcation to allow the patient access to clean the area. It is done in grade I and early grade II furcation lesions.
- Scaling and root planning: In grade I, furcation lesions have not lost bone within the furcation, so closed or open scaling and root planning procedures can resolve inflammation. If inflammation is not resolved then gingivectomy or apically positioned flap can be done depending upon the width of attached gingiva.
“Role of guided tissue regeneration in managing furcation defects”
- Odontoplasty: It is defined as the reshaping of a tooth coronal to the furcation. It widens and shallows the furcation by raising the roof of furcation. The rationale behind this technique is to create improved access for plaque control and maintenance. If cervical enamel projection is found then it is removed and the area is recontoured. Odontoplasty must be approached with caution due to the potential complications of hypersensitivity, pulpal exposure and increased risk of root caries.
- Osteoplasty: It is done to provide better gingival form by grooving the bone between the roots and then, festooning and beveling the bone over the roots.
- Gingivectomy/apical-positioned flap: It can be used in reducing or eliminating the soft tissue pockets over the furcation region to increase access for plaque control and allows resolution of periodontal inflammation.
Class 2 Furcation Defects
- Open flap debridement: If sufficient subgingival access is not possible with a closed approach, for furcated molars with deep lesions, then open flap debridement or modified widman flap yields more effective plaque and calculus removal.
- Guided tissue regeneration: Organic or synthetic barrier membranes are used based on the principles of guided tissue regeneration.
- Bone grafting: The strong focus on bone formation as a prerequisite for new attachment formation has led to implantation of bone grafts or different types of bone substitutes into furcation defects. Among these are bone autografts, allografts, xenografts and alloplastic materials designed as either bone substitutes or biologic barriers.
Class 3 and Class 4 Furcation Defects
- Tunnel preparation
- Tunneling is the process of deliberately removing bone from the furcation to produce an open tunnel through the furcation.
- It is a resective technique and used to treat advanced class 2 and class 3 furcation defects.
- The objective of this technique is to make the furcal area accessible to home care instruments by the patient.
“Early warning signs of treatment failure in furcation involvement”
Furcation Involvement Procedure
- Reflect buccal and lingual flaps and widen the involved area by removing the interradicular bone.
- Some of the interfurcal bone is sacrificed vertically and is recontoured to obtain a flat outline of bone.
- Following the bone resection enough space is established in furcation area to allow access for cleaning devices to be used by patient itself.
- Root resection: It is the procedure of removal of root apical to furcation without removal of crown in multirooted tooth.
- Hemisection: It is the splitting of two rooted tooth into a two separate teeth.
Advanced Grade 4 Furcation Involvement
- Tooth extraction is carried out.
Reconstructive and Regenerative Treatment Procedure
- Grade 1: Traditional treatment will do.
- Grade 2, 3 and 4: Various regenerative techniques include:
- Autogenous, bone grafting, e.g. osseous coagulum, bone blend.
- Allograft, e.g. freeze dried bone allograft (FDBA), demineralized freeze dried bone allograft (DFDBA).
- Alloplasts Hydroxyapatite, tricalcium phosfate.
- Citric acid root conditioning with coronally positioned flap.
- Guided tissue regeneration and combination technique.
Leave a Reply