Facial Nerve: What It Is, Function & Anatomy
Describe the facial nerve under the following headings: (a) functional components, (b) origin and course, (c) branches and distribution and (d) applied anatomy.
Answer. The facial nerve is the CN 7. It is a mixed cranial nerve (i.e. motor and sensory) but predominantly motor.
Facial Nerve Functional components
- Special visceral event (SVE) fibres supply the muscles of facial expression, etc.
- General visceral event (GVE) fibres supply the lacrimal, submandibular and sublingual salivary glands.
- Special visceral of event (SVA) fibres, which carry taste sensations from the anterior two-thirds of the tongue, except those from vallate papillae.
- General somatic of event (GSA) fibres, which carry general sensation from the concha of the external ear.
“Understanding the anatomy and functions of the facial nerve through FAQs: Q&A explained”
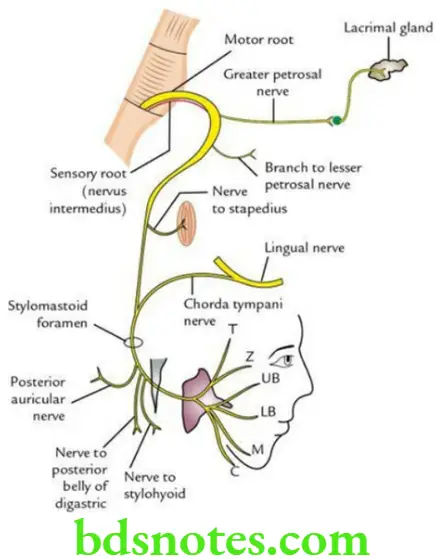
Facial Nerve Origin and Course The facial nerve has two roots:
- A large medial motor root and
- A small lateral, sensory root – the nervus intermedius.
“Importance of studying the facial nerve for medical students: Questions explained”
The motor root arises from the motor nucleus of the facial nerve in the pons. The sensory root (nervus intermedius) arises from the nucleus tractus solitaries and superior salivatory and lacrimatory nuclei in the pons.
The two roots of the facial nerve emerge on the anterior surface of the brainstem at the lower border of the pons. They pass forwards and laterally in the posterior cranial fossa along with the vestibulocochlear nerve and enter the internal acoustic meatus.
At the distal end of the internal acoustic meatus, the two roots join to form a single nerve. At the bottom of the meatus, the nerve enters the facial canal. Now, it takes a dubious course in the facial canal through the temporal bone and comes out of the skull through the stylomastoid foramen.
Now it winds around the lateral aspect of the styloid process to enter the parotid gland, where it divides into five terminal branches.
“Common challenges in understanding facial nerve anatomy effectively: FAQs provided”
Facial Nerve Branches and distribution
In the facial canal:
- Greater petrosal nerve, which joins the deep petrosal nerve to form the nerve of the pterygoid canal (Vidian’s nerve). This nerve carries parasympathetic secretomotor fibres to the lacrimal, nasal and palatine glands.
- Nerve to stapedius.
- Chorda tympani nerve: It arises about 5 cm above the stylomastoid foramen and joins the lingual nerve in the infratemporal fossa. The chorda tympani nerve serves the following functions:
- Carries taste sensations from the anterior two-thirds of the tongue, except from vallate papillae.
- Supplies secretomotor fibres to the submandibular and sublingual salivary glands.
At the stylomastoid foramen (after emerging from the facial canal):
- Nerve to the posterior belly of digastric
- Nerve to stylohyoid
- Posterior auricular nerve to supply occipital belly of occipitofrontalis
“Factors influencing success with facial nerve knowledge: Q&A”
The parotid gland, gives rise to five terminal branches to supply muscles of facial expression:
- Temporal
- Zygomatic
- Buccal (upper and lower buccal)
- Mandibular
- Cervical
Facial Nerve Applied anatomy
“Early warning signs of gaps in understanding facial nerve basics: Common questions”
- Facial nerve paralysis:
The effects of paralysis of CN VII depend on the site of the lesion. The complete paralysis of the facial nerve manifests as follows:- Loss of lacrimation due to involvement of lacrimal nerve and inability to close the eye to paralysis of orbicularis oculi. This leads to:
- Inability to close the eye on the affected side due to paralysis of orbicularis oculi.
- Exposing the cornea to the air and loss of lacrimation due to the involvement of secretomotor fibres to this gland leads to corneal dryness and keratitis.
- The angle of the mouth goes down and the dribbling of saliva due to paralysis of orbicularis oris.
- Accumulation of food bolus in the vestibule of the mouth on the affected side due to paralysis of the buccinator muscle.
- Speech becomes defective due to paralysis of lip muscles.
- Hyperacusis is a result of loss of control of movements of the stapes following paralysis of the stapedius.
- Loss of taste sensations in the anterior two-third of the tongue, due to paralysis of the chorda tympani nerve.
- Loss of lacrimation due to involvement of lacrimal nerve and inability to close the eye to paralysis of orbicularis oculi. This leads to:
- Bell palsy: It is a lower motor neuron type of facial palsy, which occurs due to compression of the facial nerve into the facial canal just above the stylomastoid foramen following its inflammation and swelling, probably due to viral infection.
“Steps to explain the anatomy of the facial nerve: Origin vs branches vs course: Q&A guide”
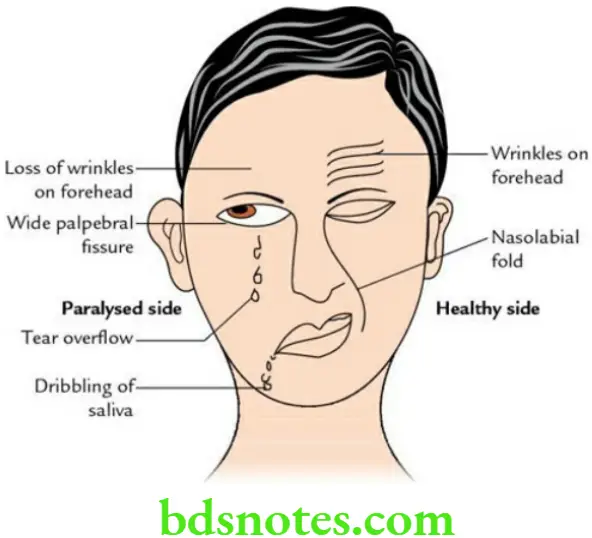
Facial Nerve Clinical features
Facial asymmetry, i.e. face of the paralysed side is pulled to the opposite/healthy side
- Loss of wrinkles on the forehead
- The inability to close the eye causes a wide palpebral fissure
- The inability of the angle of the mouth to move up while laughing
- Loss of nasolabial furrow
- Accumulation of food in the vestibule mouth
- Dribbling of saliva from the angle of the mouth
- Inability to inflate/blow the cheek properly
“Role of the facial nerve in taste sensation: Questions answered”
Leave a Reply