Different Types Of Oral Pathology Slides Notes
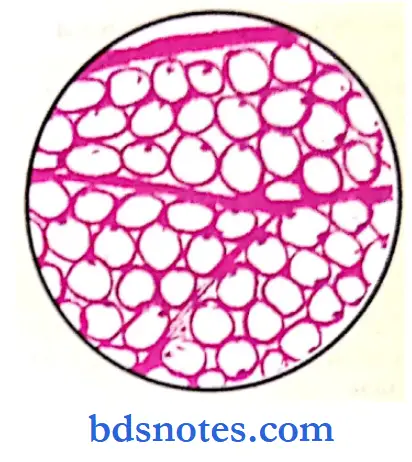
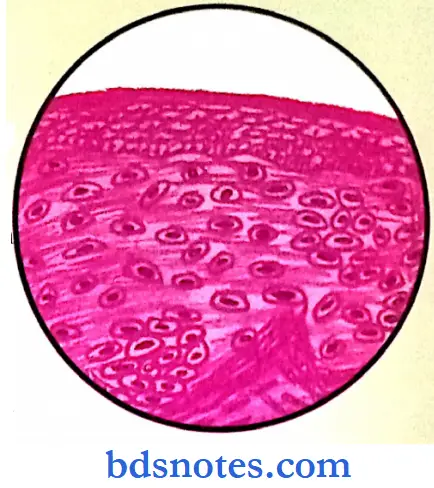
Oral Pathology Slides Lipoma
G/A: Irregularly lobulated, greasy yellow color.
C/S: Yellow and greasy.
“Understanding the role of oral pathology slides in dental education: Q&A explained”
M/E:
- An encapsulated tumor composed of normal fat cells.
- Fibrous separate containing blood vessels may run in between the lobules.
- Adipocytes are small round cells with clear cytoplasm and peripherally pushed flat nuclei.
“Importance of studying oral pathology slides for better diagnostic outcomes: Questions explained”
Special stains:
- Oil Red
- Fat-Bright Red
- Nucleus Blue.
- Sudan black B
- Fat Black.
- Nucleus Red.
“Common challenges in interpreting oral pathology slides effectively: FAQs provided”
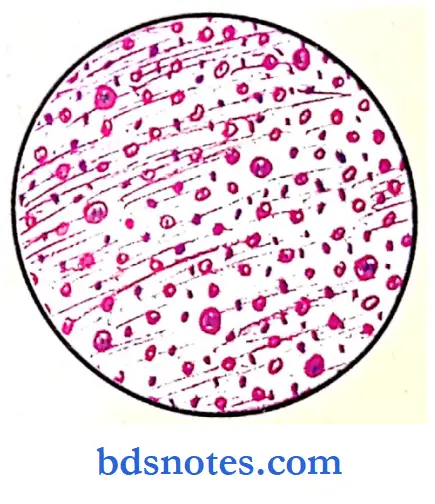
Fibrosarcoma
- These arise most commonly on fascia; intermuscular septa, subcutaneous tissue, and sometimes periosteum.
G/A: These tumors are large hemorrhagic, tan-white masses and tend to destroy the underlying soft tissues.
M/E:
- Fibro sarcomas are composed of malignant fib arranged in a “herringbone” pattern.
- The stroma is scanty and may have tumor gian Areas of hemorrhage and necrosis are seen.
- Mitotic figures of the fibroblasts are frequently seen.

“Why are oral pathology slides critical for dental students? Answered”
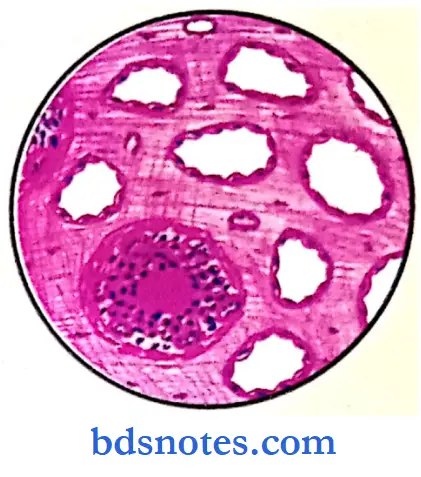
Capillary Haemangioma
- It is a benign tumor of blood vessels.
- It is usually seen in the skin and subcutaneous tissue. Most develop during childhood and consists of one of several bright red, soft often lobulated tumor.
M/E:
- The section shows the epidermis and dermis.
- Dermis shows numerous narrow capillary lumina, lined by regular and hyperplastic endothelial cells, which are filled with RBCs.
- Larger capillary hemangiomas show lobulations, separated by connective tissue septae.
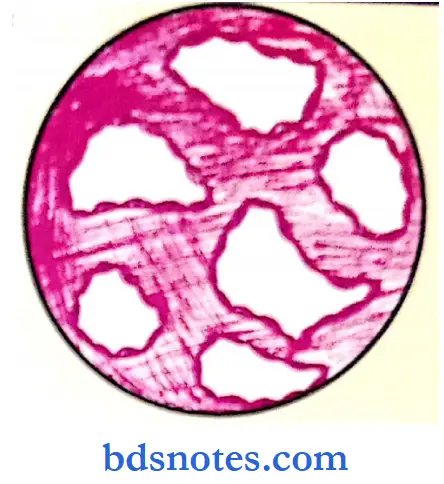
- Cavernous Haemangioma
- Site: occurs in the liver, cerebellum spleen, and other organs apart from skin and soft tissues.
oral pathology slides
M/E:
- Consists of large irregular spaces lined by a single layer of endothelial cells, filled with blood.
- They are separated by thin fibrous wall septae and some show inter-communications between each other.

“Factors influencing success with oral pathology slide interpretation: Q&A”
Actinomycosis
The center of each ulcer has a bacterial colony and sulfur granular, radiating filaments with hyaline club-like ends representing secreted immunoglobins
Chronic Venous Congestion Liver (Nutmegliver)
G/A: Liver is enlarged with a uniformly smooth surface having alternate tiny light and dark areas.
C/S: Gives typical nutmeg-like appearance with alternate dark areas representing the congested center of each lobule and light areas having the fatty peripheral part.
M/E:
- Central vein and avascular sinusoids of centrilobular regions distended with blood.
- Central hepatocytes have fatty changes and some atrophic changes due to chronic hypoxia.
- Peripheral hepatocytes (suffer from less hypoxia) develop mild fatty changes.
- Alternate fatty changes and normal hepatocytes are seen.
types of oral pathology slides

“Steps to identify types of oral pathology slides: Benign vs malignant lesions: Q&A guide”
Cvc Spleen
- Thickened capsule and trabeculae.
- sinuses are dilated and congested.
- Siderotic nodules/Gamma gandy bodies in white pulp (formed due to organization of hemorrhage and show diffuse fibrosis together with iron-pigment and calcium deposits).
- Increased fibrosis in the red pulp. Capsule and trabeculae.

Cirrhosis Liver
G/A: Liver is tan-yellow, enlarged, in early stages, later becomes atrophic, brown, and firm, due to a large amount of fibrous tissue, Surface shows nodules (fine or coarse).
C/S: Shows yellow-mahogany brown nodules of various sizes.
M/E:
- Normal architecture is lost, with an increase of connective tissue forming septae that divide into many pseudolobules.
- Fibrosis could be portal to central vein; Portal tract to portal tract, or central vein to central vein. With lymphocytic infiltrate in septae.
- Vascular architecture is reorganized due to parenchymal damage and the formation of abnormal interconnections between vascular inflow and hepatic vein outflow. Regeneration of nodules is seen.

Fatty Change: Liver
G/A: Enlarged, Soft, Yellow, rounded with smooth edges and greasy. C/S: Yellow and Greasy.
M/E:
- Liver cells are distended with fat, which appears as fat globules with their nuclei pushed to the periphery or with the nuclei in the center and surrounded by multiple tiny vacuoles of fat, giving an empty appearance.
- These fat globules are demonstrated by special stains like oil red ‘O’ Sudan Black ‘B”, Osmium tetraoxide. May have some peripheral fibrosis.
Red Hepatization
G/A: Affected lobe of the lung is voluminous, airless, brick red, firm, and consolidated, with petechial subpleural hemorrhages.
C/S: Pinkish Red surface, dry granular, with liver-like consistency.
M/E:
- Section show marked congestion of alveolar wall capillaries, with intra-alveolar exudates.
- Exudates include red cells, neutrophils, and fibrin, bacteria that fill the whole of alveolar spaces.
- Neutrophils may show ingested bacteria.
- Extravasated red cells give the red color.

“Role of histopathology slides in oral cancer diagnosis: Questions answered”
Grey Hepatization
G/A: This stage follows red hepatization affected lobe is firm, and heavy, with grayish-brown color, dry surface, and is covered by fibrinous exudates.
C/S: Dry, Granular, Grey in color with liver-like consistency.
M/E:
- The fluid portion of exudates is reduced and a large amount of fibrin is left behind.
- Exudates are separated from alveolar walls by a thin clear space. Bacteria and red cells are scanty.
- Alveolar walls are thin, with decreased vascularity, degenerating neutrophils, and increased mononuclear cells within alveolar spaces.

Secondary Deposits – Lymph Node
G/A: Single or multiple, large lymph node, solid and firm to hard. C/S: Solid, grey-white, with areas of hemorrhage and necrosis.
M/E:
- Partial loss of normal architecture with the presence of non-native tumor tissue.
- Tumor tissue is composed of cells arranged in sheets, papillary process, and glandular pattern.
- Tumor cells are large, round to polygonal with a moderate amount of eosinophilic cytoplasm and large hyperchromatic nuclei, with atypical mitoses.

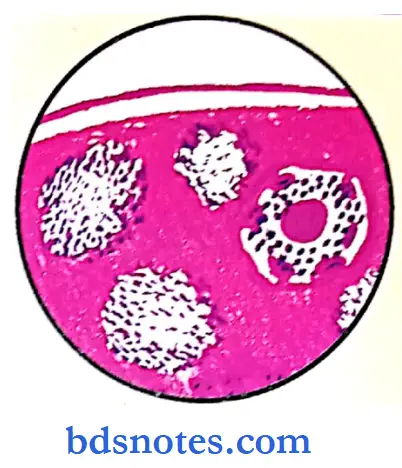
Tuberculosis Lung
G/A: Common site Apex and subapical region of the lung. Lungs show intense congestion and minute millet seed sized
yellowish-white lesions or cavity formation.
C/S: Shows varying-sized cystic spaces, to a large cavity filled with caseous materials, and thickened walls.
M/E:
- The section shows the structure of the lung with varying-sized tubercles. Tubercle is composed of epitheloid cells, lymphocytes, and Langhans giant cells, with or without central caseation necrosis and surrounding fibrous tissue.
- Surrounding alveoli and bronchioles may be empty or contain cellular exudates.
- The characteristic histological lesion in tuberculosis is the granuloma, which in this case is known as a tubercle. Shows an entire tubercle at an early stage, and illustrates a sector of the same tubercle at higher magnification.
- At the center of the tubercle is an area of caseous necrosis containing tubercle bacilli; these can only be demonstrated by specific staining methods for acid-fast bacillus.
- The caseous area is surrounded by a zone of epitheloid macrophages with abundant eosinophilic cytoplasm. Some of the macrophages fuse to produce multinucleate giant cells called Langhan’s giant cells; a typical Langhan’s giant cell is shown in more detail. Peripheral to the macrophages, there is a rim of lymphocytes.
- With further development, spindle-shaped fibroblasts appear in the peripheral lymphocytic zone of the tubercle where they are stimulated by factors produced by epitheloid cells to lay down collagen in the extracellular site
“How do healthcare providers classify oral pathology slides based on features? FAQ explained”
Hodgkins Disease
G/A: Lymph nodes are enlarged, discrete & rubbery, and firm. C/S: Solid, grey white, and homogenous.
M/E:
- The lymph node shows a loss of normal architecture.
- The characteristic neoplastic cell is the Reed-Steinberg cell.
- It is a large cell 15-45 Microns in diameter abundant amphophilic cytoplasm, binucleate or bilobed nuclei, which appear as mirror images, may be multinucleated or polypoid. These cells have large, owl eye, eosinophilic nucleoli, surrounded by a clear halo.
- These RS cells, with a background of non-neoplastic inflammatory cells like lymphocytes, plasma cells eosinophils are
Seen.
Four types: lymphocyte predominance, lymphocyte depletion, mixed cellularity, and nodular sclerosis.
T.B. Lymphadenitis
G/A: Lymph nodes are enlarged, matted.
oral pathology notes
C/S: Usually shows areas of caseous necrosis, appearing like granular, soft necrotic material resembling dry cheese.
M/E:
- The normal architecture of lymph nodes is partially affected.
- any granulomas with or without caseation are noted.
- The central zone of caseous necrosis (structure less eosinophilic and granular debris) is surrounded by large numbers of slipper-shaped epitheloid cells, few multinucleated and occasional Langhan’s giant cells, with peripheral fibrous tissue infiltrated with lymphocytes and plasma cells are seen.
- With the formation of a Ghon focus in a child’s lung, tubercle bacilli pass via lung lymphatics to regional lymph nodes where they initiate caseous necrosis and tubercle formation similar to that in the lung.
- The combination of a Ghon focus in the lung and tuberculous regional (peribronchial) lymph nodes is called a primary complex, or Ghon complex.
- The outcome of infection in a child depends on the fate of the lymph node lesion. If the child’s defenses are strong (as in most cases), healing of all the tubercles occurs by fibrosis as described previously; All that remains is a small fibrocalcific nodule in the lung periphery and similar lesions in the regional lymph nodes. The necrosis has almost reached the lymph node capsule; rupture is imminent.
Non-Hodgkin’s Lymphoma
G/A: Lymph nodes are markedly enlarged, non-tender and discrete, and firm.
C/S: Solid gray-white.
M/E: Shows loss of normal architecture of lymph node.
- It’s replaced by a monotonous cell population.
- Cells have the appearance of small lymphocytes 6-12, microns in diameter, with scant cytoplasms, round to irregular nuclei, having condensed chromatin.
- These cells are mixed with a variable number of larger cells called prolymphocytes or other neoplastic cells depending on the type of the NHL. The degree of nuclear atypia is variable. Histiocytes, eosinophils, granulocytes, and RS cells are not found.
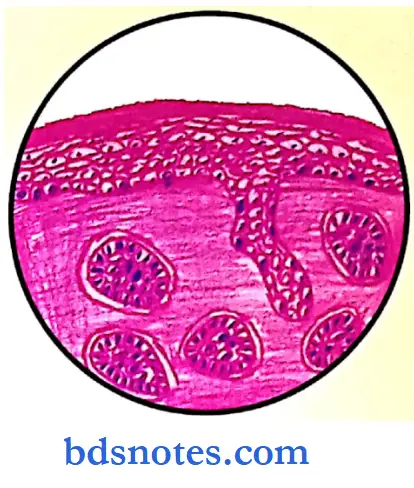
Squamous Cell Carcinoma
G/A: Appear as warty outgrowth with an infiltrating base or as a hard nodular mass. Both types normally ulcerate with raised edges and indurated base. Many have a cauliflower-like appearance.
M/E:
- Has high atypical cells in all levels of the epidermis; can be in situ or invasive. Consists of irregular masses of atypical squamous cells that proliferate & invade deeper structures.
- Tumor cells contain hyperchromatic nuclei in moderate to abundant eosinophilic cytoplasm, with atypical mitosis. These cells produce variable amounts of keratin seen as horn pearls and cornified masses, seen as epithelial pearls in well-differentiated tumors. Intercellular bridges are seen in many cases.

“Early warning signs of complications from misinterpreting oral pathology slides: Common questions”
Basal Cell Carcinoma
G/A: Ulcer could be Nodular, ulcerative superficial, erythematous, multicentric, and sclerosing; ulcer is rimmed by a waxy, smooth, firm rolled border. It erodes the deeper, structure.
M/E:
- Cells resemble those in the normal basal cell layer of the epidermis and epidermal attachment is present in nearly all cases.
- These cells form solid masses with prominent peripheral palisading & cleft-like retracting spaces around these nests of cells. Intervening stroma in loose, with fibroblasts with mucinous change and few lymphocytes.
- Individual cells are small, basophilic, and fusiform with hyperchromatic nuclei.
- Basal cell carcinoma is a common tumor composed of cells with deep blue-staining nuclei centrally located in sparse, poorly defined cytoplasm.
- The cells at the periphery of the tumor clumps are characteristically arranged in a palisading pattern, whereas the central cells are more haphazardly arranged.
- Basal cell carcinoma arises from the basal cells of the epidermis or epidermal appendages;
- It behaves as a malignant tumor in that it invades the dermis and any deeper underlying structures, but almost never metastasizes. Basal cell carcinomas occur most frequently on the light-exposed areas of skin, particularly the face, and present as nodular lesions, which may undergo ragged ulceration giving rise to the colloquial term rodent ulcer.
Osteochondroma
G/A: It is a cartilage-capped mushroom-like outgrowth, attached to the underlying skeleton by a bony stalk.
May be solitary or multiple.
C/S: Show three distinctive layers, an innermost medullary city with bone marrow, next is the bone and this is capped.
M/E:
- The bulk of the lesion is made up of mature bone trabecula
- Next is the cartilaginous cap, resembling normal hyaline cartilage.
- At the interphase between the cartilage and the bone, there is active endochondral ossification.
- Below the bony trabeculae, bone marrow elements are seen
Malignant Melanoma
G/A: Firm, Skin nodule, varying in size with variation in pigmentation irregular border having vertical/horizontal growth.
M/E:
- Normal melanocytes are present in the basal keratinocytes, interspersed among them are melanoma cells, which are larger than normal cells.
- These tumor cells are fusiform in shape, with large nuclei having irregular margins and peripherally clumped chromatin and prominent red nucleoli.
- These tumor cells are seen as nests or alveolar or irregular branching strands.
- In the dermis, they look like balloon cells, and mitotic figures are seen.
- The tumor cells contain melanin pigment in the cytoplasm.
- Special stains:
- Mason Fontana.
- Bleaching methods.
- Special stains:
- There are no abnormal melanocytes in the dermis, although pigment can be seen within histiocytes (also called melanophages).
- In invasive superficial spreading malignant melanoma as in the micrograph, large nests of atypical melanocytes (some in mitosis) are found in both epidermis and dermis.
- The epidermal component usually forms irregular clusters on the basement membrane, with some melanocytes breaking through into the upper dermis where the invasion remains superficial with a horizontal/radial growth pattern.
- Invasive nodular malignant melanoma, as in the micrograph, is usually a raised lesion that may be ulcerated; this is composed of large pleomorphic atypical melanocytes (some in mitosis) involving and often destroying the full thickness of the epidermis and growing down vertically into the dermis as continuous sheets of cells.
“Asymptomatic vs symptomatic effects of delayed evaluation for oral pathology slides: Answered”
Osteosarcoma
G/A: Depends on the relative amount of osteoid, bone, and cartilage produced.
It’s seen as a glistening white or blue-gray, well-developed tumor, is a bony hard, firm cystic, fusiform mass at the end of a long bone, giving a typical ‘Mutton-Leg’ appearance.
C/S: Greyish white tumor tissue, with foci of irregular ossification, areas of necrosis, hemorrhage, and cyst formation.
M/E:
- Tumor cells are pleomorphic varying in size in shape. Arranged in sheets with the presence of tumor osteoid.
- Cells are small to large polyhedral to spindle-shaped with poorly defined cytoplasm and large hyperchromatic nuclei, and numerous mitoses.
- Many tumor giant cells, which may be mononuclear or multinucleate, are seen.
- Intercellular stroma varies from fibrous, cartilaginous, myomatous, and osteoid. This osteoid is produced by tumor cells and is surrounded by sarcomata cells.
- Osteoid is eosinophilic, glassy has irregular contours & is rimmed by osteoblasts. It may be fibrillary with areas of calcification.
- The tumor has a very variable appearance, but islands of delicately pink-stained osteoid Ost are usually present although some parts may be irregularly mineralized.
- The tumor cells, which are derived from osteoblasts, are usually poorly differentiated and pleomorphic with much mitotic activity.
- These tumors are generally highly vascular and early bloodstream metastasis to the lungs is common.
“Can follow-up care enhance outcomes based on oral pathology slide analysis? FAQs provided”

Leave a Reply