Cysts Of Jaw Questions and Answers
Question 1. Classify cyst of oral cavity. Describe in details clinical features, radiographic feature and differential diagnosis of dentigerous cyst.
Or
Classify cysts of orofacial region. Describe clinical features radiographic features and differential diagnosis of dentigerous cyst.
Or
Write short note on dentigerous cyst.
Or
Classify cysts. Write clinical features, radiological features and management of dentigerous cyst.
Answer.
Classification of Cysts of Oral Cavity By Mervin Shear
Cysts of the Jaws
Dentigerous Cyst Epithelial:
Keratocystic Odontogenic Tumors
Cysts of the Jaw: Types, Symptoms, Diagnosis, and Treatment
“Understanding jaw cysts through FAQs: Q&A explained”
Cysts of the Jaws Developmental:
- Odontogenic
- Gingival cyst of infants
- Odontogenic keratocyst (neoplasm)
- Dentigerous cyst
- Eruption cyst
- Lateral periodontal cyst
- Gingival cyst of adults
- Botryoid odontogenic cyst
- Glandular odontogenic cyst
- Calcifying odontogenic cyst (neoplasm)
“Importance of studying jaw cysts for better diagnostic outcomes: Questions explained”
Cysts of the Jaws Non-odontogenic:
- Nasopalatine duct cyst
- Nasolabial cyst
- Midpalatal raphe cyst of infants
- Median palatine, median alveolar
- Median mandibular cyst
- Globulomaxillary cyst
Cysts of the Jaws Inflammatory:
- Radicular cyst, apical and lateral
- Residual cyst
- Paradental cyst and mandibular infected buccal cyst
- Inflammatory collateral cyst
“Common challenges in diagnosing jaw cysts effectively: FAQs provided”
Nonepithelial (pseudocysts):
- Solitary bone cyst
- Aneurysmal bone cyst
Cyst Associated with Maxillary Antrum
- Benign mucosal cyst of the maxillary antrum
- Postoperative maxillary cyst
Cyst of the Soft Tissues of Mouth, Face and Neck
- Dermoid and epidermoid cyst
- Lymphoepithelial cyst (branchial cyst)
- Thyroglossal duct cyst
- Anterior medial lingual cyst (intralingual cyst of foregut origin)
- Oral cyst with gastric or intestinal epithelium
- Cystic hygroma
- Nasopharyngeal cyst
- Thymic cyst
- Cyst of salivary glands: Mucous extravasation cyst, mucous retention cyst, ranula, polycystic disease of the parotid.
- Parasitic Cyst: Hydatid cyst, cysticercus cellulosae, trichinosis
“Steps to explain causes of jaw cysts: Odontogenic vs non-odontogenic factors: Q&A guide”
Read And Learn More: Oral Medicine Question And Answers
Dentigerous Cyst
It is also called as follicular or pericoronal cyst. It is most common type of odontogenic cyst which encloses the crown of impacted teeth.
Dentigerous Cyst Clinical Features
- It is found in children and adolescents with incidence in 2nd and 3rd decade.
- Mandibular 3rd molars and maxillary canines are most commonly impacted.
- Teeth adjacent to developing cyst and involved teeth are severely displaced and resorbed.
- Generally, it is painless but may be painful, if it gets infected.
- When dentigerous cyst expands rapidly to compress sensory nerve, then it produces pain which is referred pain.
- Dentigerous cyst has a potential to become an aggressive lesion with expansion of bone and subsequent facial asymmetry.
- Lesion has potential to expand. Cystic involvement of an unerupted third molar resulting in hollowing out of entire ramus extending to coronoid process and condyle.
“Role of epithelial remnants in causing jaw cysts: Questions answered”
Keratocystic Odontogenic Tumors
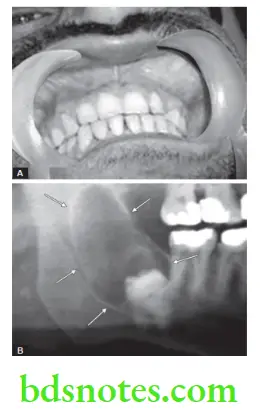
Dentigerous Cyst Radiographic Features
- It is a well-defined radiolucency which is associated with hyperostotic borders unless it is secondarily infected and is seen around an unerupted tooth.
- The cyst is unilocular but, it can be multilocular too. Multilocularity is caused by ridges in the bony wall.
- Bony margins are well-defined and sharp.
- Dentigerous cyst may involve the crown symmetrically but it can expand laterally from the crown. Cyst is attached to cementoenamel junction. Tooth which is associated with the cyst can be displaced in any direction. Mainly direction of displacement is in apical region
- Large cysts are confined to mandible. There may be resorption of roots of the adjacent teeth.
- Floor of maxillary sinus can get displaced, if cyst encroaches on it.
Dentigerous Cyst Diagnostic Features
Dentigerous Cyst Clinical diagnosis: Presence of expansive swelling over posterior region of mandible provide clinch to the diagnosis.
- Content of cystic lumen is usually thin watery yellow fluid and is occasionally blood tinged.
“Early warning signs of issues addressed by understanding jaw cyst pathogenesis: Common questions”
Dentigerous Cyst Differential Diagnosis
- Ameloblastoma or ameloblastic fibroma: They are multilocular and not associated with crown of an unerupted teeth.
- Adenomatoid odontogenic tumor: They are rare and occur in maxillary anterior region.
- Calcifying odontogenic cyst: It occurs as pericoronal radiolucency and contains evidences of calcification.
- Developmental primordial and follicular primordial cyst: It occurs in the crown of unerupted tooth and superimposition of image which may cause cyst- like radiolucency to appear as dentigerous cyst on radiograph.
- Hyperplastic follicle: Normal size of dental follicle is 2 to 3 mm. If the size of follicular space is more than 5 mm, then dentigerous cyst is most likely the diagnosis.
- Odontogenic keratocyst: OKC does not expand the bone as dentigerous cyst does. OKC is attached more apically as compared to dentigerous cyst.
“Asymptomatic vs symptomatic effects of ignoring jaw cyst triggers: Q&A”
Dentigerous Cyst Management
- Surgical: Small lesions should be surgically removed. Larger lesion consists of the surgical drainage as well as marsupialization. It causes relief in pressure and gradual shrinking of the cystic lesion by peripheral apposition of the new bone.
- Decompression: Place a small acrylic button or the short section of rubber in preformed surgical opening inside the cyst which keeps opening open and leads to drainage.
- Orthodontic treatment: For patients who want to retain the tooth, orthodontic tooth movement should be done.
Leave a Reply