Non-Odontogenic Tumors Of Oral Cavity
Epithelial Tissue
Epithelial Tissue Benign Tumors
- Papilloma
- Keratoacanthoma
- Squamous acanthoma
- Nevus
“Importance Of Understanding Non-Odontogenic Tumor Classification”
Epithelial Tissue Malignant Tumors
- Squamous cell carcinoma
- Mucoepidermoid carcinoma
- Adenocarcinoma
- Basal cell carcinoma
- Transitional cell carcinoma
- Melanoma
- Verrucous carcinoma
- Intraepidermoid carcinoma
“Risk Factors For Developing Non-Odontogenic Tumors In The Oral Cavity”
Fibrous Connective Tissue Benign tumors
- Fibroma
- Fibrous hyperplasia
- Fibrous epulis
- Giant cell firoma
- Myxoma
- Myxofiroma.
Fibrous Connective Tissue Malignant tumors
- Fibrosarcoma
Cartilage Tissue
Cartilage Tissue Benign Tumors
- Chondroma
- Chondroblastoma
- Chondromyxoid firoma.
“Early Signs Of Non-Odontogenic Tumors In The Mouth”
Cartilage Tissue Malignant Tumors
- Chondrosarcoma
Adipose Tissue
Adipose Tissue Benign Tumors
- Lipoma
- Angiolipoma.
Adipose Tissue Malignant Tumors
- Liposarcoma
Bone
Bone Benign Tumors
- Osteoma
- Osteoid osteoma
- Osteoblastoma
“Can Non-Odontogenic Tumors Be Treated Without Surgery”
Bone Malignant Tumors
- Osteosarcoma
- Osteochondrosarcoma
Vascular Tissue
Vascular Tissue Benign Tumors
- Hemangioma
- Hereditary hemorrhagic telangiectasia
- Lymphangioma
Vascular Tissue Malignant Tumors
- Hemangioendothelioma
Neural Tissue
“Difference Between Odontogenic And Non-Odontogenic Tumors”
Neural Tissue Benign Tumors
- Neurofibroma
- Neurilemmoma
- Schwannoma
Neural Tissue Malignant Tumors
- Neurosarcoma
- Neurofirosarcoma
Muscles
Muscles Benign Tumors
- Leiomyoma
- Rhabdomyoma
Muscles Malignant Tumors
- Leiomyosarcoma
- Rhabdomyosarcoma
“Role Of Biopsy In Classifying Non-Odontogenic Tumors”
Giant Cell Tumor
- Central and peripheral giant cell tumor
- Giant cell granuloma
- Giant cell tumor of hyperthyroidism.
Teratoma
Salivary Gland Tumor
Salivary Gland Tumor Benign tumors
- Adenoma
- Warthin’s tumor
- Pleomorphic adenoma.
“Understanding The Role Of Biopsy In Non-Odontogenic Tumor Classification”
Salivary Gland Tumor Malignant tumors
- Mucoepidermoid carcinoma
- Adenocystic carcinoma
- Adenocarcinoma
- Acinic cell carcinoma
- Malignant change in pleomorphic adenoma
Lymphoid Tissue
Lymphoid Tissue Malignant tumors
- Hodgkin’s and non-hodgkin’s lymphoma
- Lymphosarcoma
- Reticular cell sarcoma
- Ewing’s sarcoma
- Burkitts lymphoma
- Multiple myeloma
- Leukemia.
“Comprehensive Overview Of Non-Odontogenic Tumors And Their Types”
Lymphoid Tissue Malignant melanoma
Malignant melanoma is a neoplasm of epidermal melanocytes.
It is the third most common cancer of the skin.
Lymphoid Tissue Etiology
- Sun exposure: Persons who are exposed to the excess of sunlight develops malignant melanoma.
- Artifial UV source: PUVA thearpy has been reportedly associated with risk of melanoma.
- Socioeconomic status: It is seen in high socioeconomic status since people of high socioeconomic status go for holidays.
- Fare skin, freckles, red hair: These characteristics increased the risk of melanoma.
- Melanotic nevi are the strong risk factors.
- Genetic factors: Familial melanoma and xeroderma pigmentosum are considered to be strong genetic factors for development of malignant melanoma.
“The Role Of Imaging In Diagnosing Non-Odontogenic Tumors Accurately”
Clinical types of Malignant Melanoma
- Superficial spreading melanoma: Exists in a radial growth phase. Lesion present as tan, brown or black admixed lesion on sun exposed skin. Radial growth phase may last for several months to years.
- Nodular melanoma: It exists in a vertical growth phase. It present sharply delineated nodule with varying degrees of pigmentation. They may be pink or black.
- Lentigo maligna melanoma: Exists in a radialgrowth phase. The lesion occur as macular lesion on malar skin of Caucasians.
Acral lentiginous melanoma: Melanoma developing on the palms and soles as well as toe and figers. It is characterized by macular lentiginous pigmented area around nodule. - Mucosal lentiginous melanoma: Develops from mucosal epithelium that lines respiratory, gastrointestinal and genitourinary systems. It is more aggressive.
- Amelanotic melanoma: It is an erythematous or pink sometimes eroded nodule.
Malignant Melanoma Clinical Features
- Oral melanomas initiate as macular pigmented focal lesions.
- Most of the lesions are pigmented excepting few nonpigmented lesions which referred to as “amelanotic melanomas”, which appear as “slightly” inflamed looking areas.
- Pigmented lesions are often darkbrown, bluishblack or simply black in appearance.
- Initial macular lesions grow very rapidly and often result in a large, painful, diffse mass.
- Surface ulceration is very common and beside; this, hemorrhage, paresthesia and superficial fungal infections are often present.
- As the tumor continues to grow, small satellite lesions can develop at the margin of the primary tumor.
- Like other epithelial malignant tumors, melanomas exhibit litte or no induration at the periphery.
- Oral melanomas often cause rapid invasion and extensive destruction of bone. This often results in loosening and exfoliation of the regional teeth in the jaw.
- Widespread dissemination of the tumor cells occurs frequently in the lymph nodes as well as in the distant sites,e.g. the lung, liver, bone and brain, etc.
“Why Early Intervention Is Critical For Non-Odontogenic Tumor Outcomes”
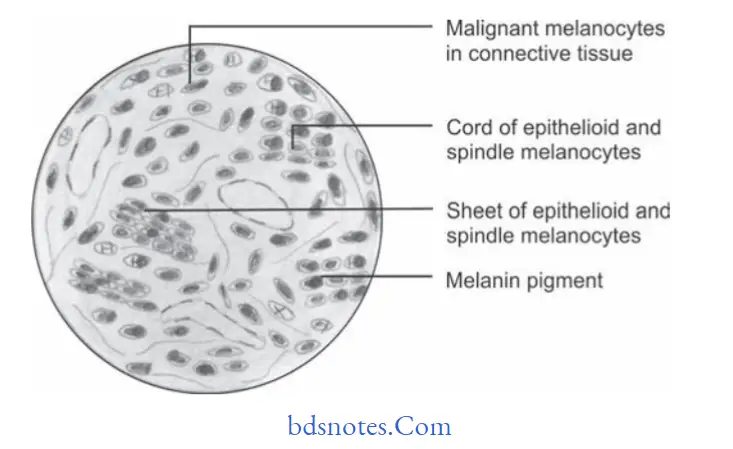
Malignant Melanoma Histopathology
- Microscopically the malignant cells lie in nest or cluster of groups in an organoid fashion.
- Melanoma cells have large nuclei, often with prominent nucleoli and show nuclear pseudoinclusion.
- Cytoplasm of the cell is abundantly eosinophilic or optically clear.
There is presence of large, epithelioid melanocytes distributed in pagetoid manner. - When melanocytes penetrate the basement membrane a flrid host cell response of lymphocytes develop.
- Macrophages or melanophages may be present.
- Vertical growth phase is characterized by the proliferation of malignant epithelioid melanocytes in the underlying connective tissues.
- These malignant melanocytes often exhibit extensive cellular pleomorphism and nuclear hyperchromatism.
- However, in some lesions melanin production by the tumor cells can be very little and on few occasions there can be virtually no melanin production.
“Best Practices For Treating Non-Odontogenic Tumor Symptoms Safely”
Malignant Melanoma Treatment
- Radical surgery with prophylactic neck dissection is often advised.
Leave a Reply