Introduction And Modern Concept Of Child Care Short Answer Questions
Question 1. Role of a Pediatric Nurse
Answer:
Role of a Pediatric Nurse:
A nurse is a person skilled or trained in caring for sick or injured people.
The role of the pediatric nurse is constantly changing. These changes are a result of expanding medical and nursing practice, emerging challenges in different aspects of child care, consumer demands, and technological advancements.
Read And Learn More: Bsc Nursing 3rd Year Child Health Nursing Previous year Question And Answers
“Understanding modern concepts of child care through FAQs: Principles, trends, and uses explained”
Role of a Pediatric Nurse Primary Caregiver:
- Provides preventive, promotive, curative, and rehabilitative care at all levels of health services.
- Care of sick children, comfort, feeding, bathing, safety, etc
- At community setup, basic responsibilities include health assessment, immunization, primary health care and referral, etc.
Role of a Pediatric Nurse Health Educator:
- Delivers planned and incidental health teaching and information to the parents and significant others about the prevention of illness, promotion, or health maintenance.
- Creates awareness about healthy lifestyles and practices regarding child care.

“Importance of studying child care for BSc Nursing students: Questions explained”
Characteristics of a nurse teacher include 4 Cs:
- C- Confidence
- C – Competence
- C – Communication
- C- Caring and empathy.
Role of a Pediatric Nurse Counselor:
- Provides – guidance to parents on health hazards of children.
- Helps – the parents and family members with independent decision-making in different
situations. - Problem-solving approach.
- Active listener to establish a therapeutic relationship between parents and the child, making health care plans easier.
Role of a Pediatric Nurse Social Worker:
- Alleviate the social problems related to child health.
- Refers the child and family for social support.
- Participates in social services.
Role of a Pediatric Nurse Team Coordinator:
- Works along with other health team members.
- Coordinates the nursing care with other services for meeting the needs of the child; for example, physician, social worker, surgeon, physiotherapist, dietician, etc.
- Maintain good interpersonal relationships with the child, family, and health team members.
Role of a Pediatric Nurse Manager:
Organize care, monitor, and evaluate patient treatment for successful outcomes in the pediatric care units in hospitals, clinics, and communities.
Role of a Pediatric Nurse Care Advocate:
- The pediatric nurse acts as an advocate to safeguard the child’s rights, to assist, and to provide the best care from the health care team.
- The nurse acts as a representative for the child, family, and other health care providers, for example, it can range from consulting the dietary department for special foods to arranging team meetings to discuss a plan of care with other health team members.
Role of a Pediatric Nurse Researcher:
- Research is an integral part of professional nursing.
- Participate in research projects related to child health.
- Provide the basis for the changes in the nursing practice and care of the children.
- Nurses are expected to be sensible enough in voicing out the needs of their patients.
“Common challenges in mastering child health nursing effectively: FAQs provided”
Role of a Pediatric Nurse Independent Practitioner:
- It is an expanded role.
- Work in rural areas as a nurse midwife and primary—care giver.
- Jointly practicing with the physician or independently.
Role of a Pediatric NurseTherapeutic Nurse:
- Identifies the problem areas in their interaction with the family and child.
- Establishment of therapeutic relationship.
Role of a Pediatric NurseRecreationist:
- The pediatric nurse plays a supportive role for the child by providing play facilities for recreation and diversion.
- It helps to decrease crises imposed by illness or hospitalization.
Role of a Pediatric Nurse Community Health Nurse:
- Monitors anticipates, and responds to public health problems in population groups.
- Evaluates health risk factors of population groups. Participates in assessing and evaluating health care services.
Question 2. Qualities of a pediatric nurse.
Answer:
Qualities of a Pediatric Nurse: A good pediatric nurse must be:
- Good observer
- Honest and truthful
- Sympathetic, kind, patient, and cheerful
- Love to work with children
- Interested in family care
- Able to provide teaching to children and their families
- Friendly and diligent
- Scientific knowledge, skill, and expertise.
“Factors influencing success with child health nursing: Q&A”
Question 3. Define pediatric nursing.
Answer:
Pediatric Nursing:
Pediatrics is the branch of medical science that deals with the care of children from conception to the adolescent in health and illness, A Paediatric Nurse (also known as a Children’s Nurse) is a nursing professional who cares for children and teens suffering from a variety of different conditions.
Question 4. Difference between adult and child care.
Answer:
Difference Between Adult And Child:
Children are not little adults. There are many differences between children, adolescents, and adults – physiological, anatomical, cognitive, social, and emotional, which all impact on the way illness and disease present in children and young people, as well as the way healthcare is provided.
Anatomical and Physiological Differences:
1. Larger BSA:
Children have a proportionately larger body surface area (BSA) than adults do. The smaller patient has a greater ratio of surface area (skin) to size. As a result, children are at greater risk of excessive loss of
2. Thinner skin:
Children have thinner skin than adults. Their epidermis is thinner and under-keratinized, compared with adults.
3. Rapidly dividing cells:
Children’s cells divide more rapidly than adults to assist in their rapid rate of growth. As a result, children are more susceptible to the effects of radiation than adults.
4. Higher HR and RR:
Children have higher heart rates and respiratory rates than adults
In newborns, the heart rate is 110-160 beats/min, and the respiratory rate is 35- 40 breaths/min. Higher respiratory rates lead to proportionately higher minute volumes. Hence, children have a greater risk of infection through the pulmonary route.
5. Immature blood-brain – barrier:
Children have immature blood-brain barriers and enhanced central nervous system ( CNS ) receptivity. As a result, children may exhibit a prevalence of neurological symptoms
6. Higher metabolic rate:
More susceptible to contaminants in food or water and has a greater risk for increased loss of water when ill or stressed.
“Steps to explain modern trends in child care: Telehealth vs personalized care plans vs family-centered approaches: Q&A guide”
7. Immature immune system:
Greater risk of infection, less hard immunity from some infection
8. Mouth:
The infant’s tongue is large. Nasal and oral airway passages are relatively small making the baby more prone to airway obstruction. Nose breathers till 6 infections ). months of age ( breathing difficulty in respiratory infections. )
9. Eyes:
- No tears in early infancy due to poor functional development of the lachrymal gland.
- Eustachian tube: It is short and straight in children (10 ° in children and 40 ° in adults). Air sinuses are not fully developed.
- The sore throat extends to otitis media because of the closeness of it to the throat.
10. Trachea:
Short and narrow trachea under 5 years. Hence they are susceptible to foreign body aspiration.
11. Glomerular filtration rate:
- The concentration of urine in newborns is 800 mOsmol / L, whereas in adults it is 1400 mOsmol / L.
- GFR and tubular functions are lower in neonates than in adults because of lower blood supply to the kidney, smaller pore size and less filtration power across the nephron.
- GFR is 38 mL/min in neonates and 125 mL/min in adults.
12. Alimentary tract:
- Water absorption is poor. The feces of the child are watery.
- Dehydration leads to circulatory failure within 24 hours if treatment is inadequate.
13. Hepatic function:
The liver is immature in newborns. Production of albumin, clotting factors, and vitamin K are less. The iron reserve is less.
14. Central nervous system:
- 90% of brain growth takes place by 2 years of age. Nerve endings in the retina (rods and cones) are not fully developed.
- Thus, the images are blurred and colorless for a few weeks.
“Role of telehealth in improving pediatric access: Questions answered”
Question 5. Factors Affecting Child Health
Answer:
Child Health:
Children are the most vulnerable population who face unusually high health risks as they grow.
Major contributors to child health are:
1. Maternal health:
A healthy mother with good nutritional status gives birth to a healthy baby. Child health may be impaired in case of inadequate nutrition or health problems during pregnancy.
2. Low birth weight:
Children born with low birth weight often have an impaired immune function, which puts them at higher risk of infection and death.
3. Nutrition:
Children get adequate quantity and quality of food to grow healthy and are less prone to develop health problems. Malnutrition causes poor growth and more chances of infection. Inadequate breastfeeding and poor complementary feeding may lead to malnutrition.
4. Environment:
Environmental health factors contribute significantly to the incidence of child mortality around the world. Inadequate sanitation, poor ventilation and housing conditions, unsafe water supply, and lack of mental health problems. Good personal hygiene practices add to the develop
5. Socioeconomic conditions:
Parental education, profession, income, housing, and urban and rural living have a great impact on the health of children. The economic condition of the family aids in good health facilities and therefore children encounter fewer health problems.
6. Health policy of government: The sound health policy of the government helps in reducing health problems in children.
“How does personalized care benefit children? FAQ explained”
Question 6. Rights of Children’s
Answer:
Rights of Children:
The child is defined as a person in the 0 – 18 years of age group.
The general assembly affirmed that the declaration of the rights of the child aims to ensure that he may have a happy childhood and enjoy it. the right and freedom for his own good and for a good society.
The following are the rights of the child:
Special rights for the child as per commission recommendations are
- Right to a safe environment.
- Right to food
- Right to health care.
- Right to education
- Right to freedom
- Right against child marriage.
- Right to be free from any discrimination
- Right to be protected from any abuse.
- Right to be heard and participate freely.
- Right to family life.
- Right to leisure and free time.
Question 7. Child welfare policy and explain about anyone.
Answer:
National Child Welfare Policy:
Keeping in view the problems and challenges faced by the Indian children, laws have been introduced and various policies and programs are being implemented for the welfare of children in India.
Child Welfare Policy:
- UN Convention on the Rights of the Child, 11th Dec, 1992.
- HMBU The National Policy for Children, Aug 22, 1974
- National Policy on Education, 1986
- The National Policy on Child Labor, August 1987
- National Nutrition Policy, 1993
- National Plan for SAARC Decade for the Girl Child 1990 – 2000
- UN Millennium Summit – MDG ( Sep 30, 2000)
- National Health Policy, 2002 National Charter for Children, 2003
- National Plan of Action for Children, 2005
- The Commissions for Protection of the Child Rights Act, 2005
- The National Policy for Children, 2013
The National Policy for Children, 1974:
- The National Policy for Children, 1974 was adopted on 22nd August 1974 in order to address the emerging challenges relating to child rights.
- The nation’s children are a supremely important asset. Their nurture and solicitude are our responsibility.
The following policy measures were taken up by the government:
- Services before and after birth
- Comprehensive health services.
- Nutrition services with the objective of removing deficiencies in the diet of children.
- Free and compulsory education for all children up to the age of 14.
- Informal education to dropouts.
- Promotion of physical education, games, sports, and other types of recreational, as well as cultural and scientific activities in schools and community centers.
- Protection against neglect, cruelty, and exploitation.
- Equal opportunity to weaker sections, physically challenged, and delinquent children
The National Policy on Child Labor (August, 1987):
The National Policy on Child Labour declared in August 1987, contains strategies for tackling the problems of child labour.
1. It includes:
- Child Labour (Prohibition and Regulation) Act, 1986 to prohibit the engagement of children in certain employments and to regulate the conditions of work of children in certain other employments.
- General development programs for benefiting children wherever possible.
- Launching of projects for the welfare of working children in areas of high concentration of child labor.
- Rehabilitation of child labor.
2. The special schools/rehabilitation centers provide:
- Non-formal / bridge education Skilled/vocational training
- Mid-day meal
- Stipend @ Rs.150 / – per child per month
- Health care facilities through a doctor appointed for a group of 20 schools.
National Nutrition Policy, 1993:
It provides the following strategies:
- Nutrition intervention for especially vulnerable populations.
- Fortification of essential foods.
- Popularization of low-cost nutritious food.
- Control of the micronutrient deficiencies amongst vulnerable groups.
- Various nutritional programs
- Nutritional surveillance.
“Early warning signs of gaps in understanding modern trends: Common questions”
Question 8. Child welfare agencies and explain about anyone.
Answer:
There are many national and international organizations working for the welfare of the most vulnerable population of our country. Following are a few of them.
Indian Council for Child Welfare:
It was established in 1952 to secure the rights and protection of Indian children.
Their activities are:
- Advocating children’s rights
- Creches for children of working and ailing mothers.
- Training programs for child care workers Sponsorship for the school education of underprivileged children M L Iron / Hb status.
- Programs for children in difficult circumstances.
- Programs with a special focus on the girl child education centers and support services.
- Honoring children for bravery.
- Honoring child artists.
- Projects for street and working children.
- Scrutiny of adoption cases.
- Rehabilitation of abandoned children.
- Institutional and daycare services for differently abled children
Childline India Foundation:
- Childline India Foundation (CIF) is the nodal agency of the Union Ministry of Women and Child Development acting as the parent organization for setting up, managing, and monitoring the Childline 1098 service all over the country.
- Childline 1098 service is a 24-hour free emergency phone outreach service for children in need of care and protection.
Unicef:
- Unicef has been working in India since 194This is the largest international organization in the country working exclusively for children.
- Unicef is fully committed to working with the Government of India to ensure that every child born in this vast and complex country gets the best start in life, thrives, and develops to his or her full potential.
- They work in the fields of health, education, nutrition, environmental hygiene, HIV, protection, and emergency.
Goals are:
- To ensure the necessary reduction in maternal, infant, and young child mortality.
- To reduce and prevent malnutrition and to improve the development of children under 3 years of age, especially those in marginalized groups.
- To introduce a range of replicable models for sanitation, hygiene, and water supply.
- To build a protective environment in which children can live and develop in the full respect of their fundamental rights.
There are many other child welfare agencies such as Save the Children Fund, Child in Need Institute, CARE, WHO, UNESCO, USAID, FAO, etc.
“Asymptomatic vs symptomatic effects of ignoring modern principles: Q&A”
Question 9. Impact of hospitalization on the child.
Answer:
Impact of hospitalization on the child:
Illness and hospitalization are stressful experiences for children and families. Long-term illness and hospitalization have the potential to negatively impact a child’s motor, cognitive, emotional, and social development.
Impact of hospitalization on children:
- Illness and hospitalization have the potential to negatively.
- Each child perceives illness and hospitalization uniquely. Common stressors in child care include
Separation anxiety, loss of control, Bodily Injury, and Pain.
1. Infant:
Separation anxiety:
- The infant passes through the three phases of
Separation anxiety. In the initial phase, infants demonstrate protest by crying and rejecting the attention of another caregiver. - Then the infant moves to the next phase of despair, he becomes quiet and withdrawn, refuses food, and appears sad, listless, and lonely.
- If the separation continues the infant enters the final phase of separation anxiety known as detachment, showing interest in surroundings, forming new relations, reluctance to meet parents, etc. In this phase, the infant is actually showing signs of resignation.
Loss of Control:
According to Erikson, the infant develops trust or mistrust during care given by parents or significant others. The infant develops a reduced sense of control due to preference given to the hospital routines, their treatment needs, and neglect of their emotional needs.
2. Toddlers:
Separation anxiety:
- Separation anxiety causes the greatest stress to hospitalized toddlers and preschoolers. During the pro-test phase, the toddler asks for parents all the time, shows temper tantrums on parents’ departure or return, and refuses to maintain routines of mealtime, bedtime, or toileting.
- During the second phase, the toddler withdraws self, engages in thumb sucking, and bedwetting although previously toilet trained, and develops sleep disturbances. Toddlers do not protest any painful procedure.
- In the final phase, the toddler does not react to parents’ visit or departure, accepts all hospital routines, and during discharge may turn away from parents and become suspicious.
Loss of Control:
- The sense of autonomy, which develops during toddlerhood is disturbed or threatened due to hospitalization.
- Hindrance to normal daily activities, and forceful confinement in bed may cause negativism in terms of temper tantrums. It exhibits regression like refusing food other than usual food at home, demanding a bottle, etc.
- This regression to earlier behavior in search of security and comfort, maybe threatening to future development.
Loss of Bodily Injury and Pain:
- Fear of the unknown, discomfort with restraints, and anticipated fear of bodily injury or pain cause toddlers to resist physical examination and diagnostic or therapeutic procedures.
- They react more than infants if they are separated from parents, restrained, watching parental apprehension, or have previous traumatic experiences.
3. Preschoolers:
Separation Anxiety:
- Preschoolers can tolerate brief periods of separation from parents as they are more secure interpersonally than toddlers.
- They express protest by crying quietly and sometimes refusing food, and medication, constantly asking when the parents will come to visit.
- They exhibit anger by breaking toys, hitting others, etc. Some children can regress in behavior and become overly dependent on their parents.
Loss of Control:
- Preschoolers expect to maintain their independence during hospitalization. They experience loss of control by mobility restriction, change of daily routine, and enforced dependency.
- They view everything from their own egocentric perspective. Hence, they perceive hospitalization as the punishment for real or imagined misdeeds, which develops a sense of shame or guilt in them.
Loss of Bodily Injury and Pain:
- The loss of interest in other activities and center of attention on the affected part of the body.
- Preschoolers are sensitive to the bodily changes caused by diseases and their treatment.
“Can targeted interventions reduce risks of outdated practices? FAQs provided”
4. School Age Children:
Separation Anxiety:
- School-age children have a better understanding and coping ability. Young school-age children need parental security and undergo phases of separation anxiety as they have just started going to school and still struggling to cope with that separation.
- This can be demonstrated as enuresis, night terrors, insomnia or nail biting, etc.
- Older school-age children feel more separated from peers and detached from daily activities in school.
- Feeling boredom, isolation, and exam tension are common in school-aged hospitalized children.
Loss of Control:
- According to Erikson’s stage of industry vs inferiority, school-age children feel helpless, and dependent on others due to physical limitations.
- Dependence in the form of enforced bed rest, use of bedpan, food of hospital choice, lack of privacy, strict bedtime routine, moving in a stretcher or wheelchair, etc. causes inferiority among them.
- They also fear losing friends during the course of hospitalization.
Loss of Bodily Injury and Pain:
- The hospitalized school-age child is apprehensive about bodily injury and pain.
- However, they are relaxed during physical examination as their understanding of body parts and functions is better than younger children.
- They express less overt behavior like crying or motor aggression. They fear death and mutilation as they understand the cause and effect of illness.
5. Adolescence:
Separation Anxiety:
- Response to hospitalization is varied in the case of adolescents.
- Some may feel confused about whether to seek parental presence some others may enjoy freedom or a period of independence.
- Loss of peer group contact may cause frustration among them.
Loss of Control:
- Hospital rules constrain their independence and lead to frustration.
- The demands of treatment interfere with the normal activities of the adolescents, Further interfering with social development and consequently, this may result in depression and feelings of hopelessness.
- They may react with rejection, uncooperativeness, or withdrawal.
“Differential applications of traditional vs modern child care methods: Questions answered”
Question 10. Pre and post-operative care of the child
Answer:
Pre and post-operative care of the child:
General Aspects of Pre – and Postoperative Pediatric Care Preoperative Care The nursing activities in the preoperative period include assessment, identification of health problems, preoperative health teaching, and preparation of the child.
Pre – and Postoperative Pediatric Care Preoperative Psychological Preparation:
- Reduce fear of separation, physical harm, pain, or death by giving simple concise, and age-appropriate information to the child and family.
- Explain the procedure and postoperative equipment in a playful way to prevent fear of the unknown.
- Clarify doubts and queries of parents and children.
Pre – and Postoperative Pediatric Care Preoperative Physical Preparation:
Physical preparation is necessary for preventing perioperative complications.
- Except in emergency situation children should preferably be free of respiratory complications and signs of malnutrition.
- Children must have nothing by mouth before surgery for the prescribed period according to their age.
- Good hydration is needed before NPO.
- Bathe the child and give mouth care in the morning.
- The incision over or the part involved in surgery must be washed and inspected. Shaving may be needed.
- Mouth should be checked for loose teeth, particularly in children. If present it should be reported to the anesthetist to prevent aspiration.
- Remove clips or pins from the hair.
- The child should be given a warm and loose hospital gown.
- Allow eyeglasses or hearing aids to the operation theatre and keep them in the recovery room for postoperative use.
- Check the identification band to see whether it is legible and secure. Premedication like sedatives and analgesics are usually given 2 hrs before surgery, except in emergency situations.
- The nurse should chart whether the child has passed urine and had a bowel movement.
- Enemas are not given regularly, except in certain conditions. Nostrils should be cleansed carefully before surgery especially in newborns and infants (hard crusts may be softened with a solution of sodium bicarbonate, Normal saline, or even warm water) as crusts may obstruct the airway.
- Ensure that the consent form is signed by parents; All laboratory test reports are included in the chart.
- The child may take their favorite toy with him to the opera theater and may be allowed to keep it until he is under anesthesia.
- Parents should be allowed to accompany the child to the operation site if they desire.
- Parents should be informed where to wait till the surge is over and whether the child will be shifted to the recovery room after surgery or to his unit directly.
Pre – and Postoperative Pediatric Care Preoperative Postoperative Care:
- Nursing activities in the postoperative phase include monitoring of the child for response to surgery, preventing complications, promoting early recovery, health teaching for post-operative exercises, and care at home after discharge.
- Immediate Postoperative Care
- Receive the child in the recovery room with detailed information.
- Position appropriately to maintain a patent airway and prevent aspiration preferably on his side or abdomen.
- Monitor vital signs every 15 min. Observe conditions and placement of dressing.
- Check and mark any apparent drainage from the operated site. Monitor IV fluid for an accurate rate of infusion and possible infiltration.
“Steps to explain preventive care in child health nursing: Immunization vs nutrition vs hygiene practices: Q&A guide”
Pre – and Postoperative Pediatric Care Preoperative Care after Recovery:
The child should be carefully handled and protected from injury. The urinary catheter should be connected to a drainage bag and stabilized properly to the bed.
- Check the activity level, general condition, and adequacy of ventilation.
- Adequate pain management according to the child’s needs.
- Observe the time of voiding and monitor intake and put out.
- Reunite parents and children to reduce anxiety. Oral fluids may be started after the following criteria are observed:
- Color Of The Aspirate Is Clear,
- Peri Staltic Movements Are Heard,
- Flatus are passed.
- Oral fluid should be started while the infusion is still going on. If well tolerated, the infusion is gradually discontinued. Diet can be started with clear liquid, full liquid, soft and then regular diet.
- Change position frequently.
- Progressive ambulation is advised to restore gastrointestinal function and prevent complications of pneumonia, thrombosis, and pressure ulcers.
Observe for Postoperative Complication:
- Observe the patient’s skin color and temperature changes.
- Watch for signs of shock such as low blood pressure, rapid pulse, cold moist pale, or cyanotic skin, dilated S pupils, and restlessness. Observe for other signs such as hemorrhage from the wound, vomiting, hypoxia, abdominal distension, hypostatic pneumonia, retention of urine, wound infection, or thrombophlebitis.
- Notify the physician if any of the above signs are present.
Pre – and Postoperative Pediatric Care Preoperative Health Teaching:
- Demonstrate postoperative exercises and encourage performing.
- Educate the dietary requirements for the child.
- Teach home care of the child depending on the surgical procedure.
“Role of immunization in reducing childhood diseases: Questions answered”
Question 11. ICDS Scheme
Answer:
ICDS Scheme Introduction:
- Integrated Child Development Services is a government program in India that provides nutritional meals, preschool education, primary healthcare, immunization, health check-ups, and referral services to children under 6 years of age and their mothers.
- ICDS Scheme represents one of the world’s largest and most unique programs for early childhood development.
- ICDS is the foremost symbol of India’s commitment to her children.
The main beneficiaries of the program were aimed to be the girl child up to her adolescence, all children below 6 years of age, and pregnant and lactating mothers.
ICDS Scheme Purpose of initiation:
Routine MCH services do not reach the target population. Nutritional components not covered by health services. Need for community participation.
ICDS Scheme Objectives:
- To improve the nutritional status of preschool children 0-6 years of age group.
- To lay the foundation for the proper psychological development of the child
- To reduce the incidence of mortality, morbidity malnutrition, and school dropout
- To achieve effective coordination of policy and implementation in various departments to promote child development
- To enhance the capability of the mother to look after the normal health and nutritional needs of the child through proper nutrition and health education
ICDS Scheme Package Of Services:
- Beneficiaries Services Pregnant women Health check-ups, immunization, supplementary nutrition, health and nutrition education.
- Nursing mother’s Health check-up, supplementary nutrition, health, and nutrition education
- Other women 15 – 45 years Nutrition and health education Children less than 3 yrs Health check-up, immunization, supplementary nutrition, referral services
- Children in age 3 -6 yrs Health check-ups, immunization, supplementary nutrition, referral services, nonformal education
- Adolescent girls 11 – 18 yrs. Supplementary nutrition and health education
ICDS Scheme Component :
- Health Check-ups.
- Immunization.
- Growth Promotion and Supplementary Feeding.
- Referral Services.
- Early Childhood Care and Pre-school Education.
- Nutrition and Health Education.
ICDS Scheme Supplementary Nutrition:
Supplementary nutrition is given to children below 6 years, and nursing and expectant mothers from low-income groups.
The aim is to supplement nutritional intake as follows:
- Each child up to 6 years of age to get 300 calories and 8-10 grams of protein
- Each adolescent girl to get 500 calories and 20-25grams of protein
- Each pregnant woman and lactating mother is to get 500 calories and 20-25 gms of protein
- Each malnourished child to get 600 calories and 16-20 grams of protein
“How does nutrition improve overall child health? FAQ explained”
ICDS Scheme Immunization:
Immunization of children against 6 vaccine-preventable diseases is being done, while for expectant mothers, immunization against tetanus is recommended.
ICDS Scheme Health Check UP:
- Record of weight and height of children at periodical intervals
- Watch over milestones
- Immunization
- Deworming
- General check-up for detection of disease
- Treatment of diseases like diarrhea, ARI
- Prophylaxis against vitamin A deficiency and anemia
- Referral of serious cases
- Antenatal care of expectant mothers
- Post-natal care of nursing mothers and care of newborn infants
Non-formal Pre-School Education (PSE):
- Children between the ages 3-6 years are imparted non-formal pre-school education in an Anganwadi in each village with about 1000 population.
- The objective is to provide opportunities to develop desirable attitudes, values, and behavior patterns among children.
- Locally produced inexpensive toys and materials are used in organizing play and creative activity.
Referral Services:
- During health check-ups and growth monitoring, sick or malnourished children, in need of prompt medical attention, are referred to the Primary Health Centre or its sub-center.
- Nutrition and Health Education: Health education is given to women so that they can look after their own health, nutrition, and development needs as well as that of their children and families.
The ICDS Team:
- The ICDS team comprises the Anganwadi Workers, Anganwadi Helpers, Supervisors, Child Development Project Officers (CDPOs), and District Programme Officers (DPOs).
- Medical officers, Auxiliary Nurse Midwife (ANM), and Accredited Social Health Activists (ASHA) form a team with the ICDS functionaries to achieve convergence of different services.
Question 12. Concept of modern pediatrics nursing
Answer:
Concept of modern pediatrics nursing:
The health of children has historically been of vital importance to all societies because children are the basic resources of the future of mankind. In any country, mothers and children constitute approximately 60% of the population.
“Early warning signs of undiagnosed preventive care gaps: Common questions”
Definition And Concept Of Pediatrics:
- The word “pediatric” is derived from the Greek word ‘pedia’ meaning child and ‘iatric’ means treatment and ‘ics’ means a branch of science.
- Thus, pediatrics is defined as the branch of medical science that deals with child development and care and with the diseases of childhood and their treatment.
- Pediatrics refers to the comprehensive and continued care of children. It serves both wellness and illness.
Modern Pediatrics:
- It is difficult to say when Pediatrics became a separate specialty. It developed gradually as the knowledge of the developmental needs of children increased in society.
- Pediatrics as a specialty developed with the establishment of the Department of Pediatrics in various medical colleges, and the establishment of separate pediatric units for children in general hospitals and fondling homes.
- Today we no longer consider children as miniature adults. Childhood is considered a separate phase of life.
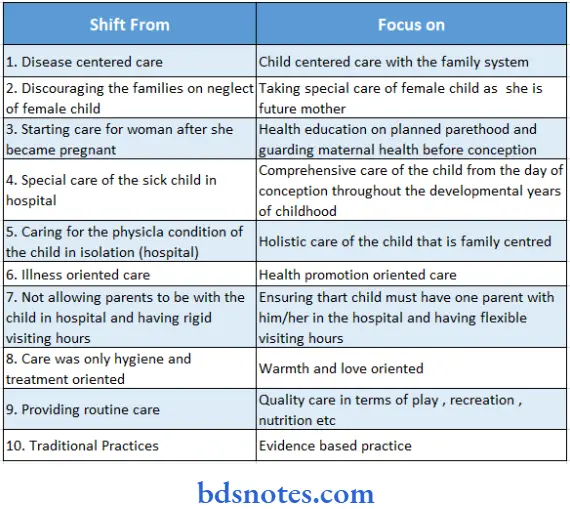
- The present concept of health care for children focuses on the prevention of illness and promotion of health rather than the treatment of illnesses alone.
- The present focus of pediatrics is shifting from a traditional to a process-oriented one that is based on sound scientific rationale.
The focus of pediatrics is shifting: Shift From Focus On:
Leave a Reply