Chapter 4 Pathogenic Organisms Question And Answers
Question 1. Pathogenicity of staphylococcus aureus.
Answer:
Pathogenesis Staph. aureus is an important pyogenic organism and lesions are localised in nature in contrast to streptococcal lesions which are spread in nature
Thick creamy pus is formed in staphylococcal infections Staphylococcal diseases may be classified as:
Cutaneous and deep infections; food poisoning, nosocomial infections, skin exfoliative diseases and toxic shock syndrome.
- Cutaneous Infections: Superficial infections include pustules, boils, carbuncles, abscesses, styes, impetigo, pemphigus neonatorum, and wound and burn infections.
- Deep Infections: These include osteomyelitis, tonsillitis, pharyngitis, sinusitis, pneumonitis, empyema, endocarditis, meningitis, bacteriaemia septicemia, and pyemia.
- Food Poisoning: Staphylococcal food poisoning may follow 2-6 hours after the ingestion of contaminated food which contains preformed enterotoxin of Stap. aureus.
- Nosocomial Infections: They are an important cause of hospital-acquired infections.
- Skin Exfoliative Diseases: These diseases are produced by the strains of Staph. aureus that produce exfoliative toxin. Stripping of the superficial layers of the skin from the underlying tissue occurs in the various exfoliative syndromes caused by staphylococci (bullous impetigo, pemphigus neonatorum, Ritter’s disease). Staphylococcal scalded skin syndrome (SSSS) is one example of an exfoliative disease in which toxin spreads systemically.
- Toxic Shock Syndrome (TSS): It is caused by toxin shock syndrome toxin (TSST-1). Although TSS became widely known in association with the use of tampons by menstruating women, it occurs in other situations also.
“Understanding pathogenic organisms through FAQs: Q&A explained”
Question 2. Pathogenicity of Streptococcus pyogenes.
Answer:
Pathogenesis: Str. Pyogenes produces pyogenic infections with a tendency to spread locally. Nonsuppurative sequelae of, local infections include acute glomerulonephritis are rheumatic fever
1. Pyogenic Infections
Respiratory infections: Sore throat (acute tonsillitis and/ or pharyngitis) is the most common of streptococcal diseases. Scarlet fever It consists of a combination of sore throat and generalised erythematous rash. It is caused by a strain producing the erythrogenic toxin.
Skin infections: Str. Pyogenes causes suppurative infections of the skin with a predilection to produce lymphangitis and cellulitis. The two typical streptococcal skin infections are erysipelas and impetigo. These skin infections are the main cause leading to acute glomerulonephritis children in the tropics.
Other pyogenic infections
- Puerperal sepsis: Str pyogenes was an important cause of puerperal sepsis, It used to take a heavy toll of life before antibiotics became available.
- Sepsis: Infections of skin lesions (eczema, psoriasis, scabies), wounds and burns. Pyaemia, septicemia, abscess in internal organs (brain, lung, liver, and kidney).
2. Non-Suppurative Complications: Str. Pyogenes infections are sometimes followed by two important non-suppurative sequelae, acute rheumatic fever and acute glomerulonephritis. These complications occur one to four weeks after the acute infection. Str. pyogenes is no longer detectable when these complications set in.
- The latent period suggests an immune response. Rheumatic fever is often preceded by sore throat while acute glomerulonephritis by the skin infection.
- These sequelae or complications are believed to be the result of hypersensitivity to some streptococcal components. Rheumatic fever may follow infection with any serotype of Str. pyogenes while acute glomerulonephritis is caused by only few nephritoginic type.
“How do pathogenic organisms cause diseases? FAQ answered”
Question 3. Difference between exotoxins and endotoxins.
Answer:
Exotoxins
- They are lipopolysaccharides in nature.
- They are heat labile
- They are actively secreted by living cells into medium.
- Highly antigenic stimulates the formation of antitoxin that neutralizes.
- They are converted into toxoid by formaldehyde.
- Enzymic in action.
- They have specific pharmacological effect to each toxin.
- They have very high potency.
- They are highly specific for particular tissue example, tetanus toxin for the central nervous system.
- They do not produce fever in host.
- They are mainly produced by Gram-positive bacteria and also by some Gram-negative bacteria.
Endotoxins
- They are protein (polypeptide) and molecular weight 10,000 to 900,00.
- Heat stable
- Form integral part of the cell wall and released on disruption of the bacterial cell.
- Weakly antigenic: antitoxin is not formed but antibodies against polysaccharides are raised.
- They can not be toxoided.
- No enzymic in action.
- Nonspecific action of all endotoxins.
- They have low potency
- They are nonspecific in action
- They produce fever in host
- They are produced by Gram-negative bacteria.
“Importance of studying pathogenic organisms for BSc Nursing students: Questions explained”
Question 4. Pathogenicity of pneumococcus pneumonia.
Answer:
Pneumococci colonize the human nasopharynx and may cause infection of the middle ear, paranasal sinuses, and respiratory tract by direct spread.
Pneumonia: Pneumococci are one of the most common bacteria causing pneumonia, both lobar and bronchopneumonia. They also cause acute tracheobronchitis and empyema. Bacteremia may complicate pneumococcal pneumonia. This can result in metastatic involvement of the meninges, joints, and, rarely, the endocardium.
Lobar Pneumonia: In adults, types 1-8 are responsible for about 75 percent of cases of pneumococcal pneumonia. In children, types 6, 14, 19, and 23 are frequent causes. Pneumonia results from aspiration of pneumococci contained in upper airway secretions into the lower respiratory tract.
- When the normal defences are compromised by viral infection, anesthesia, chilling or other factors, pneumococci multiply, penetrate the bronchial mucosa, and spread through the lung along peribronchial tissues and lymphatics.
- Contiguous spread commonly results in inflammatory involvement of the pleura. This may progress to empyema. Pericarditis is another uncommon but well recognized complication.
Bronchopneumonia: Bronchopneumonia is almost always a secondary infection. This may be caused by any serotype of pneumococcus. Other causative agents responsible for bronchopneumonia include Staph. aureus, K. pneumoniae, Str. pyogenes, H. influenzae, Fusobacterium species, and Bacteroides. Bronchopneumonia is frequently a terminal event in aged and debilitated patients
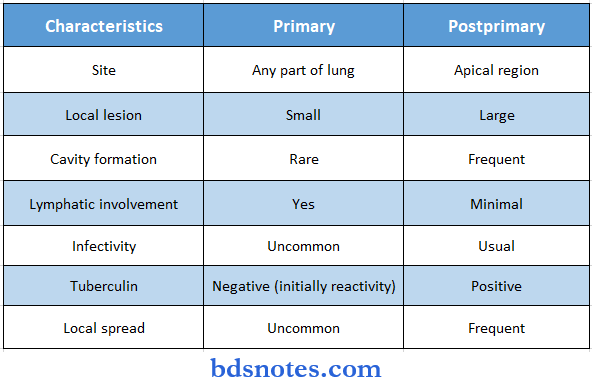
Question 5. Difference between primary and secondary tuberculosis.
Answer:
Difference between primary and secondary tuberculosis.
“Common challenges in understanding pathogenic organisms effectively: FAQs provided”
Question 6. Laboratory diagnosis for mycobacterium tuberculosis.
Answer:
Laboratory Diagnosis: Bacteriological diagnosis can be established by microscopy, culture examination, or by animal inoculation test. established by
1. Specimen: Specimen collection depends on the site of involvement. Tuberculosis may involve lungs (pulmonary) or sites other than lungs (extrapulmonary).
- Pulmonary tuberculosis: Sputum is the most common specimen. It is collected in a clean wide-mouthed container. A morning specimen may be collected on three consecutive days. If sputum is scanty, a 24-hour specimen may be collected. When sputum is not available, laryngeal swab or bronchial washings are collected. In children, gastric washings may be examined as they tend to swallow sputum.
- Meningitis: Cerebrospinal fluid (CSF) from tuberculous meningus (TBM) often forms a spider web clot on standing examination of which may be more useful than of fluid.
- Renal tuberculosis: Three consecutive days morning samples of urine are examined.
- Bone and joints tuberculosis: Aspírated fluid
- Tissue: Blopsy of tissue.
2. Direct Microscopy: Smear is made from the specimen and stained by the Ziehl-Neelsen technique It is examined under oil immersion lens.
- The acid-fast bacilli (AFB) are bright red bacilli against a blue background. appear as A negative report should not be given till at least 300 fields have been examined.
- Grading of smears is done according to number of bacilli seen. If a large number smears are to be examined, fluorescent microscopy is more convenient.
- Smears are stained with fluorescent dyes such as auramine ‘O’ or auramine rhodamine and examined under ultraviolet light. The bacilli appear as bright bacilli against a dark background.
3. Concentration of Specimens Concentration of a specimen is done to achieve:
- Homogenization of the specimen
- Decontamination i.e. To kill other bacteria present in the specimen.
Read And Learn More: Bsc Nursing 1st Year Microbiology Previous year Question and Answers
- Concentration i.e. To concentrate the bacilli in a small volume without inactivation.
- Such concentrate is used for culture and animal inoculation tests besides smear preparation. Several concentration methods are in use.
4. Serology Serology includes the detection of anti-mycobacterial antibodies in patient serum. Various methods such as enzyme-linked immunosorbent assay (ELISA), radioimmunoassay (RIA), and latex agglutination assay have been employed. The diagnostic utility of these antibodies is equivocal. WHO has banned the use of these tests for the diagnosis of active tuberculosis.
5. Molecular Methods Polymerase chain reaction (PCR) is a rapid method in the diagnosis of tuberculosis. It is based on DNA amplification and has been used to detect M. tuberculosis directly in clinical specimens.
Question 7. Pathogenesis of Tuberculosis.
Answer:
Pathogenesis of Tuberculosis: The source of infection is usually an open case of pulmonary tuberculosis. The mode of infection is by direct inhalation of aerosolized bacilli contained in droplet nuclei of expectorated sputum tubercle bacilli are acquired from persons with active disease who are excreting viable bacilli by means of coughing, sneezing, or talking.
- Airborne droplet nuclei containing bacteria, 1 to 5 µm, enter the respiratory tract of an exposed individual and are deposited in the lung alveoli.
- Infection also occurs infrequently by ingestion, for example, through infected milk, and rarely by inoculation.
- The initial infection with M. tuberculosis is referred to as a primary infection. Subsequent disease in a previously sensitized person, either from an exogenous source or by reactivation of a primary infection, is known as postprimary (secondary or reinfection) tuberculosis with quite different pathological features.
“Why is early learning of pathogens critical for nursing success? Answered”
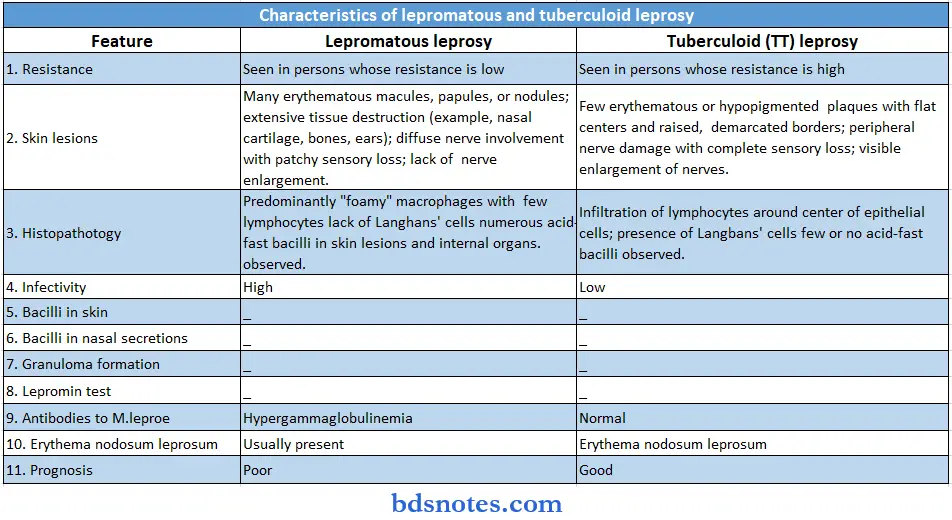
Question 8. Difference between lepromatous and tuberculoid leprosy.
Answer:
Question 9. Pathogenesis of Salmonella Typhi. or enteric fever.
Answer:
Pathogenesis: S. typhi, S. paratyphi A, and usually S. paratyphi B are confined to human beings. The majority of other salmonellae are primarily infective for animals and human beings are secondarily infected.
Salmonellae causes three types of clinical syndrome in human beings, enteric fever, septicaemia, and gastroenteritis.
Enteric Fever: The term enteric fever includes typhoid fever (S. typhi) and paratyphoid fever (S. paratyphoid A, B, C). Infections due to S. typhi and S. paratyphi A are prevalent in India.
Typhoid fever: The infection is acquired by ingestion through contaminated food and water. The incubation period is usually 7-14 days.
The clinical course may vary from mild pyrexia to a fatal Culminating disease. The characteristic features are hepatosplenomegaly, stepladder pyrexia with relative bradycardia, and leucopaenia. Skin rashes known as rose spots may appear during the second or third week.
Paratyphoid fever: Paratyphoid fever resembles typhoid fever but is milder, S. paratyphi A, B, and C cause paratyphoid fever.
“Steps to explain types of pathogenic organisms: Bacteria vs fungi: Q&A guide”
Question 10. Laboratory diagnosis of Enteric Fever.
Answer:
Laboratory Diagnosis: Bacteriological diagnosis of enteric fever consists of
- Isolation of bacilli.
- Demonstration of antibodies.
1. Isolation of Bacilli: This may be done by culture of specimens like blood, feces, urine, aspirated duodenal fluid, etc. The selection of relevant specimens depends upon duration of the illness which is very important for the laboratory diagnosis of enteric fever
2. Demonstration of Antibodies.
Widal Test: It is an agglutination test for the detection of agglutinins (H and 0) in patients with enteric fever. Salmonella antibodies start appearing in the serum at the end of first week and rise sharply during the third week of enteric fever. Two specimens of sera at an interval of 7 to 10 days are preferred to demonstrate a rising antibody titre.
Question 11. Shigella dysentriae.
Answer:
Shigellae cause bacillary dysentery. Humans are the only known reservoir of Shigella organisms infection occurs by ingestion. The infection is highly communicable because of the low infective dose required to produce the disease.
The minimum infective dose is low, as few as 10-100 bacilli being capable of initiating the disease, probably because they survive gastric acidity better than other enterobacteria.
- Shigella spp. are pathogens of man and other primates, and the pathogenesis of infection with these bacteria and entero-invasive E. coli (EIEC) is very similar.
- Shigella cause disease by invading and replicating in cells lining the colonic mucosa. After reaching the large intestine, the shigellae multiply in the gut lumen.
- The shigellae multiply within the epithelial cells and spread laterally into adjacent cells, where cell-to-cell passage occurs, and deep into the lamina propria. The infected epithelial cells are killed and the lamina propria and submucosa develop an inflammatory reaction with capillary thrombosis.
- Bacillary dysentery has a short incubation period (1-7 days, usually 48 hours). The onset and clinical course are variable and are largely determined by the virulence of the infecting strain.
- The clinical manifestations of shigellosis vary from asymptomatic to severe forms of the disease. The main clinical features are frequent passage of loose, scanty feces containing blood and mucus, along with abdominal cramps and tenesmus.
- Fever and vomiting may be present. Infection is usually self-limited, although antibiotic treatment is recommended to reduce the risk of secondary spread to family members and other contacts. In dysentery caused by S. dysenteria type 1, patients experience more severe symptoms.
“Role of viruses in causing infectious diseases: Questions answered”
Question 12. Pathogenesis of E.coli.
Answer:
Pathogenesis Esch. coli forms a part of the normal intestinal flora of man and animal. There are four major types of clinical syndromes which are caused by Esch. coli:
- Urinary, Tract Infection
- Diarrhea
- Pyogenic Infections, And
- Septicaemia.
1. Urinary Tract: Infection Esch. coli is the most common organism responsible for urinary tract infection (UTI). Esch, coli that cause UTI often originates in the intestine of the patient.
2. Diarrhoea Esch. coli causing diarrhoeal diseases are of four groups. They produce
diarrhea with different pathogenic mechanisms.
- Enteropathogenic Esch, coli (EPEC): EPEC adheres tightly to enterocytes, leading to inflammatory reactions and epithelial degenerate changes.
- Enterotoxigemic Esch. coli (ETEC): These are the strains that form a heat-labile enterotoxin (LT) a heat-stable enterotoxin (ST) or both. They are now known to be a major cause of diarrhea in children in developing countries and are the most important cause of travellers diarrhea. The name travelers diarrhea refers to diarrhea in persons from developed countries within a few days of their visit to one of the developing countries.
- Enteroinvasive Esch. coli (EIEC): Some strains of Esch. coli invade the intestinal epithelial cells as do dysentery bacilli and produce disease identical to shigella dysentery. These have been named enteroinvasive Esch. coli (EIEC). On instillation into the eyes of guinea pigs, EIEC cause keratoconjunctivitis, This diagnostic test for EIEC is called Sereny test.
- Enterohaemorrhagic Esch coli (EHEC) or Verocytotorin-producing Esch, coli (VTEC) hemorrhagic These strains cause haemolytic uraemic syndrome (HUS). The toxin responsible is called Verotoxin’ because of its effect Vero cells in culture.
3. Pyogenic Infections Esch. coli may cause wound infection, peritonitis, cholecystitis, and neonatal meningitis. It is an important cause of neonatal meningitis.
4. Septicaemia Esch. coli is a very common cause of septicaerria in many hospitals. This condition usually occurs in debilitated patients and mortality is very high.
“How do pathogenic organisms invade the human body? FAQ explained”
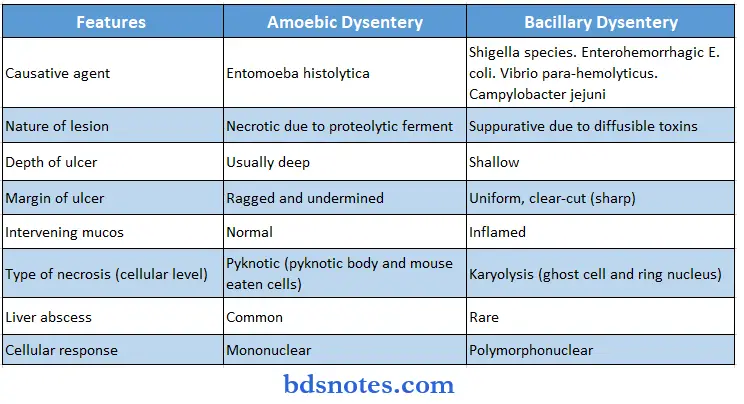
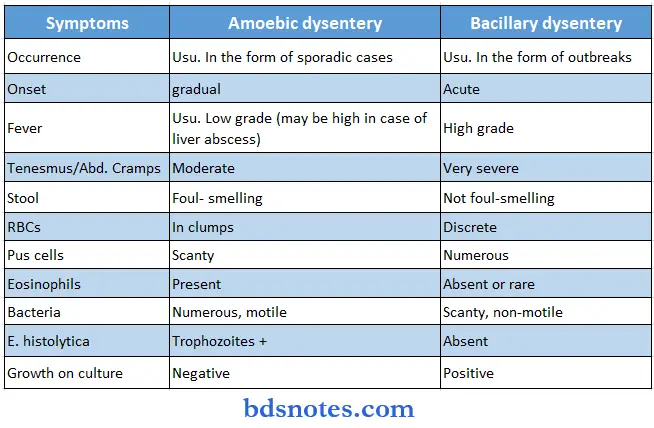
Question 13. Difference between Amoebic and Bacillary dysentery.
Answer:
Question 14. Pathogenesis of diarrhea.
Answer:
Diarrhoea Esch. coli causing diarrhoeal diseases are of four groups. They produce diarrhea with different pathogenic mechanisms.
Enteropathogenic Esch, coli (EPEC): EPEC adheres tightly to enterocytes, leading to inflammatory reactions and epithelial degenerate changes.
Enterotoxigemic Esch. coli (ETEC) These are the strains that form a heat-labile enterotoxin (LT) a heat-stable enterotoxin (ST) or both. They are now known to be a major cause of diarrhea in children in developing countries and are the most important cause of travelers diarrhea. The name travelers’ diarrhea refers to diarrhea in persons from developed countries within a few days of their visit to one of the developing countries.
Enteroinvasive Esch. coli (EIEC): Some strains of Esch. coli invade the intestinal epithelial cells as do dysentery bacilli and produce disease identical to shigella dysentery. These have been named enteroinvasive Esch. coli (EIEC). On instillation into the eyes of guinea pigs, EIEC causes keratoconjunctivitis, This diagnostic test for EIEC is called the Sereny test.
Enterohaemorrhagic Esch coli (EHEC) or Verocytotorin producing Esch, coli (VTEC) hemorrhagic These strains cause hemolytic uraemic syndrome (HUS). Toxin responsible is called Verotoxin’ because of its effect Vero cells in culture.
Question 15. Enlist organisms causing diarrhea
Answer:
Bacteria
- Vibrio cholera
- V. parahaemolyticus
- Escherichia coti (ETEC, EPEC) – Cryptosporidium panrum
- Salmonella Enteritidis
- S. Typhimurium
- Other Salmonella sp.
- Campylobacter sp.
- Yersinia enterocolitica
- Shigella sp.
- Clostridium perfringens
- C. difficile
- Staphylococcus aureus
- Bacillus cereus
- Aeromonas hydrophilia
- Plesiomonas shigelloides
Viruses
- Rotavirus
- Astrovirus
- Calicivirus
- Norwalk virus
- Adenovirus
Protozoa
- Entamoeba histolytica
- Oiardia lambda
- Isospora belli
Cestodes: Hymenolepis nana
Nematodes
- Trichuris trichiura
- Strongyloides stercoralis
- Ascaris lumbricoides
- Hookworms
Trematodes: Schistosoma mansoni
“Early warning signs of gaps in understanding pathogenic organism basics: Common questions”
Question 16. Write a short note on laboratory diagnosis of diarrhea.
Answer:
Laboratory Diagnosis
- Collection of Specimens: In most cases the stool is sent for bacterial culture. Because there are many other potential pathogens, the laboratory must be informed which tests to perform.
- Direct Microscopy: Microscopic examination of the stool may reveal white blood cells if the patient has inflammatory diarrhea. The bacterial pathogen may be visible on direct microscopic examination of the stool.
- In general, a wet film of a concentrate of the feces should be examined for protozoa, protozoal cysts, and helminth ova, and a stained film for the oocysts of Cryptosporidium.
- Culture: Selective and differential culture media are commonly used to attempt to identify bacterial pathogens in stool. The differential aspect of the media often allows differentiation of bacterial species based on colony morphology the differences in colony appearance are usually due to different biochemical characteristics of the organisms.
- Vibrios Culture: Selective media such as TCBS or bile salt agar are used. Culture plates are incubated at 37°C for 24-48 hours. Vibrio parahaemolyticus is a halophilic vibrio in media containing sodium chloride.
- Vibrios Identification: Identification of isolates is done by colony morphology, biochemical reactions
and slide agglutination test.- Esch. coli
- ETEC
- EPEC
- EIEC
- EAEC
- Esch. coli Culture: Cuture is done on blood agar and MacConkey’s agar. These media are incubated at 37°C for 24 hours.
- Esch. coli Identification: Identification of isolates is done by colony morphology, biochemical reactions, slide agglutination with antisera. For the identification of EIEC strains Sereny test is used. Another method for the identification of these strains is invasion of cultured HeLa cells.
Production of verocytotoxin (VT) is confirmed by testing the strains on Vero cells, in which they cause cytopathic effects.
Question 17. Blood Culture.
Answer:
A blood culture is a medical laboratory test used to detect bacteria or fungi in a person’s blood. Blood is normally sterile, and the presence of microbes in the blood often indicates a serious bloodstream infection such as a bacteremia, or fungemia, that can result in sepsis.
- The test involves drawing the blood into bottles containing chemicals that encourage microbial growth, which are then placed in an incubator for several days to allow the organisms to multiply.
- If microbial growth is detected, a Gram stain is made from the blood culture bottle to confirm that bacteria are present and to provide a preliminary identification.
- The blood is then inoculated onto an agar plate to isolate the organisms for further testing. A positive Gram stain from a blood culture is considered a critical result and must immediately be reported to the clinician.
- To ensure accurate results, blood cultures are drawn using sterile technique. If the sample is contaminated with skin flora, the person will appear to have those organisms in their blood.
- When a blood culture is performed, it is usually drawn in at least two different sets (one set of bottles from each arm) so that contamination is easier to detect. If an organism only appears in one of the two sets, it is more likely to be a contaminant.
- When a patient shows signs or symptoms of a systemic infection, results from a blood culture can verify that an infection is present, and they can identify the type (or types) of microorganism that is responsible for the infection.
- For example, blood tests can identify the causative organisms in severe pneumonia, puerperal fever, pelvic inflammatory disease, neonatal epiglottitis, sepsis, and fever of unknown origin (FUO). However, negative growths do not exclude infection.
Question 18. Blood smear
Answer:
A blood sample is used to look for abnormalities in the number and shape of blood cells, presence of parasites. blood smear, also referred to as a peripheral smear for morphology, is an important test for evaluating blood-related problems, such as those in red blood cells, white blood cells, or platelets.
It has a wide range of uses, including distinguishing viral infections from bacterial
infections, evaluating anemia, looking for causes of jaundice, and even diagnosing malaria. Unlike automated tests (such as a CBC), a technician or physician looks at a blood smear under a microscope in order to detect a wide range of changes that give clues to underlying diseases.
Blood Smear Purpose Of Test: A blood smear involves looking at a sample of blood under the microscope after applying special stains and looking for abnormalities or changes in red blood cells, white blood cells, and platelets.
There are many reasons why your doctor may order a blood smear. Some of these include:
- To further evaluate abnormalities found on a complete blood count (CBC) such as a high or low red blood cell count, white blood cell count, or platelet count.
- To evaluate an infection (identifying the types of white blood cells present can help determine if an infection is viral, bacterial, or parasitic, as well as the severity)
- To look for causes of unexplained jaundice
- As part of a workup for people who have unexplained weight loss (defined as a loss of 5 percent of body weight over a 6 month period without trying)
- To evaluate symptoms of lightheadedness and palor (paleness)
- To look for causes of petechiae, bruising, or excess bleeding
- With a low platelet count, to determine if the cause is increased degradation or decreased production (based on the size)
- To investigate findings suspicious for blood-related cancers
- To look for malaria
- To confirm sickle cell disease
- To evaluate symptoms of bone pain
- To look for causes of enlargement of the spleen, liver, or lymph nodes.
A blood smear looks for the numbers and characteristics of the three types of blood cells:
- Red blood cells (RBCs) are the cells that transport oxygen to the tissues
- White blood cells (WBCs) are cells that fight infection among several other functions
- Platelets are cell fragments that play an important role in blood clotting.
“Asymptomatic vs symptomatic effects of ignoring pathogenic risks: Q&A”
Question 19. Enumerate the organism causing urinary track infection.
Answer:
E. coli and coliforms account for the large majority of naturally acquired urinary tract
infections. Those acquired in the hospital, following instrumentation, are more often caused by other bacteria such as Pseudomonas and Proteus.
The most frequently encountered O serotypes of E. coli in UTI include O1, O2, O4, O6, O7, O18, and O75. These are also known as nephritogenic strains. E. coli that cause UTI often originate in the gut of the patient. The bacteria may gain access to the urinary tract by the ascending or the hematogenous route.
- Other members of the family Enterobacteriaceae that usually cause UTI are Klebsiella, Proteus, and Citrobacter, and those that rarely produce UTI are Salmonellae, Edwardsiellae, and Enterobacter.
- The gram-positive organisms that can cause UTI are Staphylococcus aureus, coagulase-negative staphylococci, Streptococcus faecalis, S. pyogenes, S. agalactiae, S. milleri, other streptococci, and anaerobic streptococci.
- Rarely, Gardnerella vaginalis may cause UTI.
- Candida albicans may cause UTI in diabetic and immunocompromised patients.
- The hospital-associated infection following instrumentation and catheterization is mostly caused by Pseudomonas and Proteus.
Question 20. Write down the laboratory diagnosis of Urinary track infection (UTI).
Answer:
Laboratory Diagnosis: Urinary Tract Infection: Normal urine is sterile, but during voiding may become contaminated with commensals of genital
- Specimen Collection Midstream urine specimen (MSU): collected preferably prior to administration of antibiotics.
- Specimen is collected in a sterile container. (Before collecting a sample, genitalia should be cleaned with soap and water and men are instructed to retract the foreskin of glans penis whereas women should keep the labia apart.
- (The first portion of urine is allowed to pass, then without interrupting the urine low, mid-portion of the stream is collected. The first portion of urine adequately lushes out the normal urethral flora.)
- Catheter specimen: Urine should be collected directly from the catheter and not from the collection bag, The catheter should hot-touch the container. Although a catheter specimen yields excellent results but catheterization to obtain urine is not justified because of risk of introducing infection.
- Urine specimens from infants: A clean catch specimen after cleansing of genitalia is preferred. 2. Transport As urine is a good culture medium, specimens after collection should reach the laboratory with minimum delay, if it is not possible, the specimen is to be refrigerated at 4°C.
- Laboratory Methods Part of the specimen is used for bacteriological culture and the rest is examined immediately under the microscope.
- Microscopy Urine is centrifuged and the deposit is examined under the microscope to detect pus cells, erythrocytes, epithelial cells, and bacteria.
- Culture Most laboratories use a semiquantitative method (standard loop technique) for the culture of urine specimens.
- Identification The organisms are identified by colony characters Grams staining, motility, biochemical reactions and slide agglutination test.“
- Antibiotic sensitivity test Esch. coli and other common urinary pathogens develop multiple drug resistance. Antibiotic sensitivity is necessary to administer proper antibiotics.
Question 21. Widal Test.
Answer:
Widal test: In the Widal test used for the diagnosis of enteric fever, two types of antigens are used: the flagellar antigens (H) and somatic (O) antigens. H antigen is a formolised suspension of the organisms which combined with its antibody, forms large, loose, and fluffy clumps resembling wisps of cotton wool.
- Conical Dreyer’s tubes are used for H agglutination. O (somatic) antigen is prepared by treating the bacterial suspension with alcohol.
- It forms tight, compact deposits resembling chalk powder at the base of round-bottomed (Felix) tubes on combination with antibody. Agglutinated bacilli spread out in a disk-like pattern at the bottom of the tube, whereas, the negative reaction shows a compact button-like deposit.
“Can targeted interventions improve outcomes using pathogenic knowledge? FAQs provided”
Question 22. Describe the normal microbial flora of different body parts.
Answer:
Normal Flora refers to the population of microorganisms that inhabit the skin and mucous membranes of normal human body. A healthy fetus in utero is free from micoorganisms. During birth the infant is exposed to vaginal flora.
Within a few hours of birth, oral and nasopharyngeal flora develops and in a day or two resident flora of the lower intestine appears. The normal microbial flora is more or less constant for each species of animal.
- Normal Flora Of The Skin: The skin contains 102 to 101 organisms per cm2. Bathing has little effect on the resident flora of the skin. Staph epidermidis and diphtheroids are numerous and most constant in the skin. Other microorganisms include Peptococcus, Str viridans, Enterococcus, Micrococcus, Esch. coli, Proteus, Candida albicans, and Propionibacterium aono. Penicillin-resistant staphylococci are seen in individuals working in hospitals.
- Normal Flora Of The Conjunctiva: The conjunctiva is relatively free from bacteria due to the flushing action of tears and due to the presence of lysozyme in it. The predominant organisms are Corynebacterium xerosis, Staph. epidermidis, Moraxella species, and non-hemolytic streptococci.
- Normal Flora Of The Nose And Nasopharynx: The flora of the nose harbors diphtheroids, staphylococci, streptococci, and Haemophilus species. The nasopharynx of the infant is sterile at birth but, within 2-3 days after birth, acquires the flora carried by the mother and the attendants. The nasopharynx is a natural habitat of the common pathogens that cause infections of the nose, throat, bronchi, and lungs.
- Normal Flora Of The Mouth: The mouth contains micrococci, Gram-positive aerobic spore-bearing bacilli, coliforms, Proteus, and lactobacilli. The gum pockets between the teeth have a wide spectrum of anaerobic bacilli, anaerobic micrococci, microaerophilic and anaerobic streptococci, vibrios, fusiform bacilli.
- Corynebacterium species, actinomyces, mycoplasma and Bacteroides are all found in varying extents. The mouth of an infant is not sterile at birth. It generally contains the same organisms as those present in the mother’s vagina i.e. a mixture of micrococci, streptococci, coliform bacilli, and Doderlien’s bacilli. These organisms diminish in number during the first 2-5 days after birth and are replaced by the bacteria present in the mouth of the mother.
- Normal Flora Of The Upper Respiratory Tract: Within 12 hours after birth alpha haemolytic streptococci are present in the upper respiratory tract. They become the dominant organism of the oropharynx and remain so for life. In the pharynx and trachea, flora is similar to that of the mouth. A few bacteria are present in normal bronchi, but smaller bronchi and alveoli are normally sterile.
- Normal Flora Of The Gastrointestinal Tract: The gastrointestinal tract of the foetus in utero is sterile. It becomes contaminated with organisms shortly after birth. In breastfed infants, the intestine contains lactobacilli, enterococci, colon bacilli, and staphylococci.
- In bottle-fed infants, the intestine contains Leptotrichia, anaerobic lactobacilli, colon bacilli, and aerobic and anaerobic spore-bearing organisms. Due to the low pH of the stomach, it is virtually sterile except soon after eating, As the acidic pH of the stomach becomes alkaline in the intestine, the number of bacteria increases progressively beyond the duodenum to the colon. The bacterial count is low in the small intestine compared to that in the large intestine.
Question 23. Describe the Organisms causing sore throat.
Answer:
Sore throat is essentially an acute tonsillitis or pharyngitis. It is characterized by edness and edema of the mucosa, exudation of tonsils, pseudomembrane formation, edema of the uvula, gray coating of tongue, and enlargement of cervical lymph nodes.
Causative agents of sore throat are given:
Bacteria
- Streptococcus β-hemolytic group A and occasionally groups C and G
- Corynebacterium diphtheriae
- Haemophilus influenza
- Bordetella pertussis
- Neisseria gonorrhoeae
- Treponema vincentii
- Leptotrichia buccalis
Fungi
- Candida albicans
- C. Viruses
- Epstein-Barr virus
- Adenoviruses
- Coxsackievirus A
Question 24. Write a Short Note on Food poising.
Answer:
The term bacterial food poisoning is restricted to acute gastroenteritis due to the presence of bacteria, usually in large numbers, or their products in food. It is of three types.
Infective type: In this type, the multiplication of bacteria occurs in vivo when infective doses of microorganisms are ingested with food. The incubation period is generally 8 to 24 hours. A typical example of this type of food poisoning is by Salmonella.
Toxic type: In this type, the disease follows ingestion of food with preformed toxin. The incubation period is short (2 to 6 hours). An example is staphylococcal food poisoning.
Causative agents of food poisoning
1. Infectlve type
- Salmonella typhimurium
- S. Enteritidis
- S. Heidelberg
- S. Indiana
- S. Newport
- S. Dublin
- Vibrio parahaemolyticus
- Campylobacter jejuni
2. Toxic type
- Staphylococcus aureus.
- Bacillus cereus
- Clostridium botulinum
3. Infectlve—toxic type: Clostridium perfringens
Infective-toxic type: In this type, bacteria release the toxin in the bowel. The incubation period is 6 to 12 hours. A typical example is C. perfringens food poisoning. For the laboratory diagnosis. It has also been described earlier under “Laboratory Diagnosis of Diarrhea”.
“Differential applications of opportunistic vs primary pathogens: Questions answered”
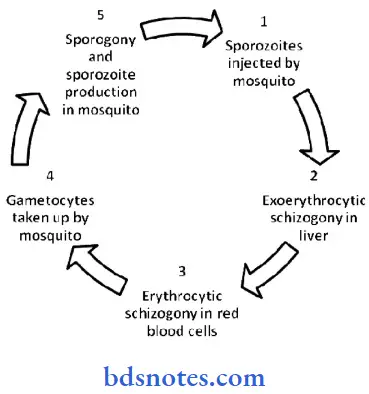
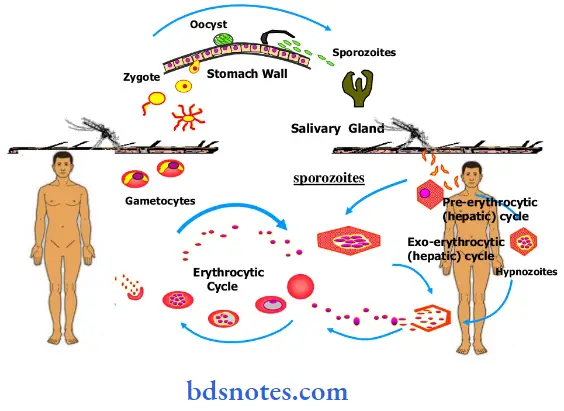
Question 25. Describe life cycle of a malarial parasite.
Answer:
Malaria is a mosquito-borne infectious disease of humans. Malaria is caused by a parasite that is passed from one human to another by the bite of infected Anopheles mosquitoes.
After infection, the parasites (called sporozoites) travel through the bloodstream to the liver, where they mature and release another form, the merozoites which introduces the protists via its saliva into the circulatory system, and ultimately to the liver where they mature and reproduce.
Intermediate host: human
- Final host: mosquito
- Infective stage: sporozoite
- Infective way: mosquito bites skin of human
- Parasitic position: liver and red blood cells
- Transmitted stage: gametocytes
- Schizogonic cycle in red cells: 48 hrs/P.v
- Sporozoite: tachysporozite and bradysporozite
“Difference between bacteria and viruses in pathogenic organisms: Q&A explained”
Question 26. Write a short note on lab diagnosis of malaria.
Answer:
Lab Diagnosis of Malaria: Method used to diagnose
- Microscopy Serology
- Rapid Diagnostic Tests
- Molecular biology method (PCR)
Microscopy
- Gold standard
- Highly sensitive, specific
- Laboratory diagnosis of malaria can by made through microscopic examination of thick or thin blood smear.
- Thick smears are used for screening purposes Thin smears are for morphological detail and species identification.
- The mainstay of malaria diagnosis has been the microscopic examination of blood, utilizing blood films Although blood is the sample most frequently used to make a diagnosis, both saliva and urine have been investigated as alternative, less invasive specimens.
- More recently, modern techniques utilizing antigen tests or polymerase chain reactions have been discovered, though these are not widely implemented in malaria-endemic regions.
- Areas that cannot afford laboratory diagnostic tests often use only a history of subjective fever as the indication to treat for malaria.
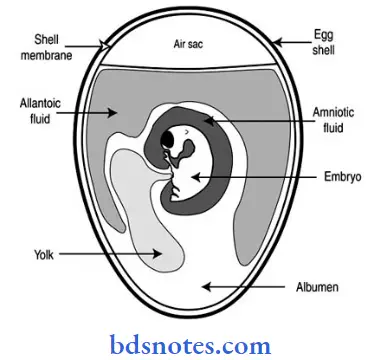
Question 27. Draw a well-labeled diagram of the embryonated egg.
Answer:
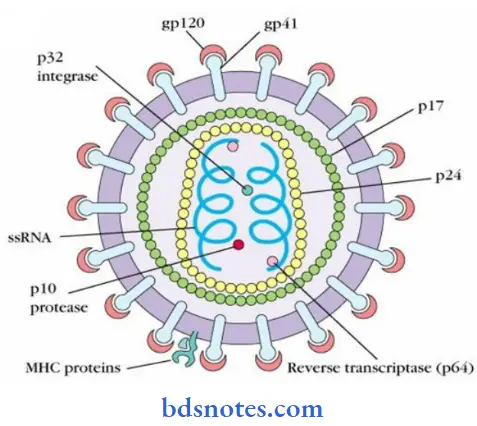
Question 28. Draw a good diagram of HIV viruses.
Answer:
“Most common complications of poorly understood pathogenic organisms: FAQs”
Question 29. Write down the causes and Routes and Modes of HIV infection.
Answer:
Routes of Transmission: Virus is present in the blood, semen, and cervical and vaginal secretions, and these sources are important in transmission. HIV is spread only by three modes
- Sexual contact with infected persons (heterosexual or homosexual)
- By blood and blood products
- From infected mother to babies (intrapartum, perinatal, postnatal).
The modes of transmission of HIV and their relative risks are shown in Tables
1. Sexual Intercourse: HIV is primarily a sexually transmitted infection. Heterosexual transfer of virus is the route by which the great majority of infections are spread, accounting for 90 percent of the global total.
- Both sexes are affected equally. Transmission in developing countries is almost always heterosexual and can take place in both directions.
- The presence of other sexually transmitted diseases such as syphilis, gonorrhea, or herpes simplex type 2 increases the risk of sexual HIV transmission as much as a hundred-fold.
- Sex workers are at high risk due to their large number of partners. Most early studies established that unprotected anal intercourse was a particular risk, especially to the passive, receptive partner. The risk increases in proportion to the number of sexual encounters with different partners.
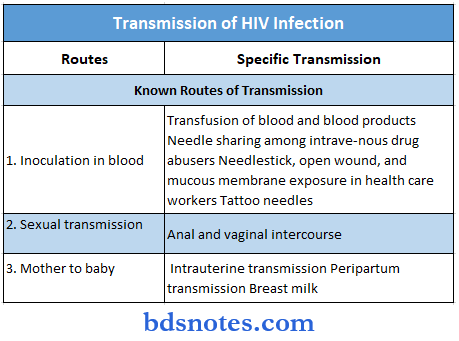
2. Blood and Blood Products: Transfusion of infectious blood or blood products is an effective route for viral transmission.
- Contaminated Needles
- This is particularly relevant in drug addicts who share syringes and needles. Drug and sexual routes merge when misusers support their habit by prostitution.
- The use of unsterile syringes and needles by qualified and unqualified health workers makes iatrogenic.
- Contamination of eyes and mucous membranes is another possible route, but this is seldom confirmed.
- Tattoo needles and contaminated inks are other potential means by which HIV can be transmitted.
3. Mother-to-Child Transmission: Transmission of infection from mother to baby can take place before, during, or after birth.
Mother-to-infant transmission rates vary from 13 to 40 percent in untreated women Infants can become infected in utero, during the birth process, or, more commonly, through breastfeeding. Transmission during breastfeeding usually occurs early (by 6 months).
Question 30. Write the stages of the HIV infection
Answer:
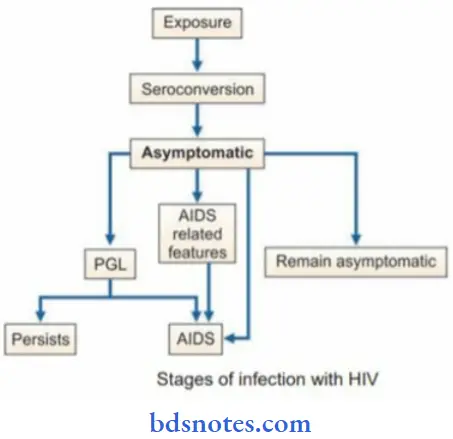
The natural evolution of HIV infection can be considered in the following stages.
- The acute seroconversion illness resembles glandular fever, with adenopathy and flu-like symptoms. Within 3-6 weeks of infection with HIV, about 50 percent of persons experience low grade fever, malaise, headache, lymphadenopathy, sometimes with rash and arthropathy resembling glandular fever.
- During this period there is a very high level of virus replication occurring in CD4+ cells. Tests for HIV antibodies are usually negative at the onset of the illness but become positive during its course. Hence this syndrome has been called ‘seroconversion’ illness.
“Why are pathogenic organisms often misunderstood in practice? Questions answered”
Asymptomatic or Latent Infection: A clinically asymptomatic or “latent” period follows the acute infection. During this time, there is a high level of ongoing viral replication.
They show positive HIV antibody tests during this phase and are infectious. The infection progresses in the course of time through various stages, including CD4 lymphocytopenia, minor opportunistic infections, persistent generalized lymphadenopathy, and AIDS-related complex (ARC), ultimately terminating in full-blown AIDS, with its characteristic infections and malignancies. The time from infection to death may be as long as 10 years and is inevitable in 70 percent of infected persons.
Persistent Generalized Lymphadenopathy (PGL ): Persistent generalized lymphadenopathy (PGL) is present in 25-30 percent of patients who are otherwise asymptomatic. This has been defined as the presence of enlarged lymph nodes, at least 1 cm in diameter, in two or more noncontiguous extra inguinal sites, that persist for at least three months, in the absence of any current illness or medication that may cause lymphadenopathy. The rate of progression of patients with PGL to AIDS is no greater than in those without adenopathy. This by itself is benign but the cases may progress to ARC or AIDS.
AIDS Related Complex (ARC): This group includes patients with considerable immunodeficiency, suffering from various constitutional symptoms or minor opportunistic infections. The typical constitutional symptoms are fatigue, unexplained fever, persistent diarrhea, and marked weight loss of more than 10 percent of body weight. ARC patients are usually severely ill and many of them progress to AIDS in a few months. With no treatment, the interval between primary infection with HIV and the first appearance of clinical disease is usually long in adults, averaging about 8-10 years. Death occurs about 2 years later.
AIDS: This is the end-stage disease representing the irreversible breakdown of immune defense mechanisms, leaving the patient prey to progressive opportunistic infections and malignancies. AIDS may be manifested in several different ways, including lymphadenopathy and fever, opportunistic infections, malignancies, and AIDS-related dementia.
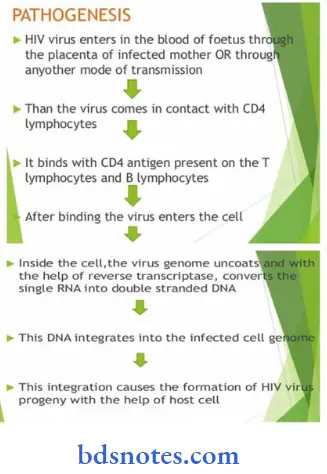
Question 31. Pathogenesis of HIV and AIDS.
Answer:
Pathogenesis of HIV and AIDS
“Cost of ignoring pathogenic risks vs benefits of systematic prevention: Q&A”
Question 32. Write down the laboratory diagnosis of HIV/ Aids.
Answer:
Laboratory Diagnosis: Specific Tests for HIV Infections
- Antigen detection: The p24 antigen is the earliest virus marker to appear in the blood. ELISA can be used for the detection of this antigen. Virus isolation is an important test for diagnosis in the window period when antibodies are absent in the serum of a patient.
- Virus isolation: For diagnosis, the virus is not routinely isolated. It can be isolated from CD4 lymphocytes of peripheral blood, bone marrow, and serum. Virus isolation is an important test for diagnosis in the window period when antibodies are absent in serum of the patient.
- Detection of viral nucleic acid: Viral nucleic acid can be detected by polymerase chain reaction (PCR). The test is highly sensitive and specific. It is also useful for diagnosis in the window period.
- Antibody detection: Demonstration of antibodies is the simplest and most commonly employed technique for diagnosis. It may take several weeks to months for antibodies to appear after infection. HIV-infected persons remain negative for antibodies during window period, when initial viral replication takes place for about 2-3 weeks. There are two types of serological tests-screening and supplemental.
Laboratory Diagnosis Screening tests
1. ELISA test: ELISA is the method most commonly used. It is a highly sensitive and specific test. It is an extremely good screening test and most laboratories use a commercial ELISA kit that contains both HIV-1 and HIV-2. Saliva is an acceptable alternative to serum for antibody testing by ELISA.
2. Rapid tests: These tests take less than 30 minutes and do not require expensive
equipment. The rapid tests include dot-blot assay, particle agglutination, HIV spot, and comb tests.
3. Simple tests: They take 1-2 hours and do not require expensive equipment.
Laboratory Diagnosis Supplemental test
Western blot test: In this test, HIV proteins are separated and these proteins are blotted onto strips of nitrocellulose paper. These strips are reacted with test sera. Antibodies to HIV proteins, if present in test serum, combine with different fragments of HIV. The position of the color band on the strip indicates the fragment of antigen with which antibodies have reacted.
Question 33. The life cycle of Ascaris Lumbricoid ( Round Worm).
Answer:
Life Cycle Ascaris lumbricoides pass its life cycle in only one host, man. No intermediate host is required. Man is the only definitive host. Adult worms live the jejunum of man. Fertilized eggs containing the unsegmented ova are passed in the feces. These eggs are not immediately infective to man.
Egg undergo development in soil. A rhabditiform larva is developed from an unsegmented ovum and undergoes first molting within the eggshell. These eggs containing rhabditiform larvae are pathogenic to man. Man acquires infection by ingestion of food, drink of raw vegetables contaminated with eggs containing rhabditiform larvae (embryonated eggs).
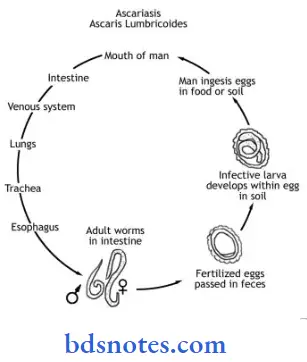
In the upper Part of the small intestine (duodenum), rhabditiform larvae are liberated from the embryonated eggs. These newly hatched larvae then burrow their way through the mucous membrane of the small intestine and are carried by the portal circulation to the liver.
They then pass out of the liver and via right heart enter the pulmonary circulation. In the lungs they grow much bigger in size and moult twice. They break through the capillary wall and reach the lung alveoli. From the larvae crawl up the bronchi and trachea and propelled into the larynx and pharynx and are Srallowed.
They pass down the esophagus to the stomach and localize in the upper part of the small intestine, their normal abode. Another molting takes place. The larvae grow into adult worms and sexual maturity occurs. The gravid female begins to discharge eggs in the stool and the life cycle is again repeated.
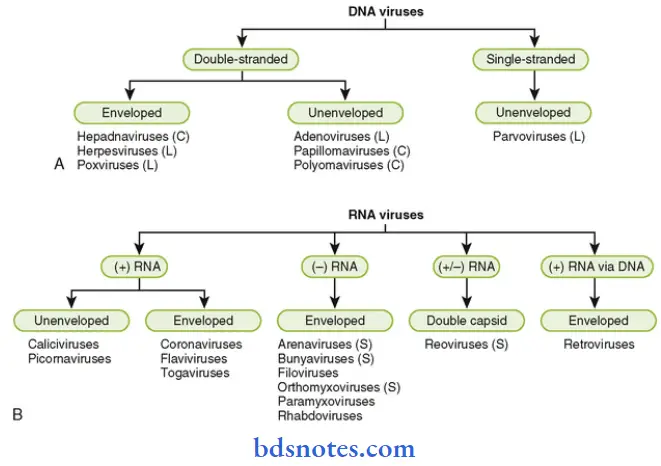
Question 34. List 4 DNA viruses and 4 RNA viruses.
Answer:
DNA Viruses: Sometimes referred to as the happy viruses
- Herpes
- Hepadna
- 4/3 Adeno
- 4/3 Papova
- 4/3 Parvo
- 4/3 Pox
- 4/3 Most
DNA viruses are double-stranded, show icosahedral symmetry, and replicate in the nucleus.
1. Parvoviridae Family: Three genera have been described: Parvovirus, Adenosatellovirus, and Densovirus.
2. Hepadnaviridae Family: This consists of the human hepatitis type B virus and related viruses of animals and birds. (The name comes from hepa = liver, and DNA for DNA core). Three viral types are known that infect mammals (humans, woodchucks, and ground squirrels) and another that infects ducks.
3. Papovaviridae Family: Two genera have been recognized—Papillomavirus and Polyomavirus. Papillomavirus are also a former member of the Papovaviridae family. Polyomaviruses were formerly a part of the Papovaviridae family before it was split into two families.
4. Adenoviridae Family: Members have been classified into two genera: Mastadenovirus (mammalian adenoviruses) and Aviadenovirus (adenoviruses of birds)
5. Poxviridae Family: The family is divided into several genera. All poxviruses tend to produce skin lesions. Some are pathogenic for humans (smallpox, vaccinia, molluscum contagiosum); others that are pathogenic for animals can infect humans (cowpox, monkeypox).
RNA Viruses: There are certain generalities about RNA viruses, most of which are the opposite of DNA viruses. Most RNA viruses are single-stranded (half are positive [+1 stranded, half negative [-1), enveloped, show helical capsid symmetry, and replicate in the cytoplasm
- 4/3 Toga
- 4/3 Corona
- 4/3 Retro
- 4/3 Picorna
- 4/3 Calici
- 4/3 Reo
- 4/3 Orthomyxo
- 4/3 Paramyxo
- 4/3 Rhabdo
- 4/3 Bunya
- 4/3 Arena
- 4/3 Fibo.
Paramyxoviridae Family: Three genera have been recognised
- Paramyxovirus which consists of the Newcastle disease virus, mumps virus and
parainfluenza viruses of humans, other mammals, and birds. - Morbillivirus, containing measles, canine distemper, rinderpest, and related viruses.
- Pneumovirus, containing respiratory syncytial virus of humans and related viruses.
Paramyxoviridae Family: Three genera have been described
- Alphavirus, consisting of viruses formerly classified as Group A arboviruses.
- Rubivirus, consisting of the rubella virus has no arthropod vector.
- Pestivirus, consisting of the mucosal disease virus, hog cholera virus, and related viruses.
- Coronaviridae Family Only one genus of Coronavirus has been recognized.
Members include human coronavirus causing upper respiratory disease, avian infectious bronchitis virus, calf neonatal diarrhea coronavirus, murine hepatitis virus, and related viruses. Most human coronaviruses cause mild acute upper respiratory tract illnesses (colds) but a new coronavirus identified in 2003 causes a severe acute respiratory syndrome (SARS). Toroviruses, which cause gastroenteritis, form a distinct genus.
Reoviridae Family: Icosahedral, nonenveloped viruses, medium-sized (6080 nm), with double-layered capsids. The genome consists of double-stranded RNA in 10-12 pieces. Three genera have been recognised.
- Reovirus, containing reoviruses from humans, other mammals, and birds.
- Orbivirus, containing several species of arboviruses such as bluetongue virus, and African horse sickness virus.
- Coltivirus includes the Colorado tick fever virus of humans.
- Rotavirus including human rotaviruses, calf diarrhea virus, and related agents. Other genera may have to be defined to include plant and insect viruses belonging to this family.
“Is pathogen-related risk reversible if addressed promptly? Answer provided”
Question 35. General Characteristics or properties of Viruses.
Answer:
Viruses are the smallest known infective agents and are perhaps the simplest form of life known. Viruses do not possess a cellular organization and they do not fall strictly into the category of unicellular microorganisms.
Even the simplest of microorganisms are cells enclosed within a cell wall, containing both types of nucleic acid (DNA and RNA), synthesizing their own macromolecular constituents and multiplying by binary fission.
Main properties of viruses
- Viruses do not have a cellular organization.
- They contain only one type of nucleic acid, either DNA or RNA but never both.
- They are obligate intracellular parasites.
- They lack the enzymes necessary for protein and nucleic acid synthesis and are dependent
for replication on the synthetic machinery of host cells. - They multiply by a complex process and not by
binary fission. - They are unaffected by antibacterial antibiotics.
Question 36. Explain the various methods of the cultivation of viruses.
Answer:
Cultivation Of Viruses: Because viruses are obligate intracellular parasites, their growth requires susceptible host cells capable of replicating them. They cannot be grown on any inanimate culture medium. Three methods are employed for the cultivation of viruses:
- Animal inoculation
- Embryonated eggs
- Cell culture.
1. Animal Inoculation: Uses of Animal Inoculation
- Primary isolation of certain viruses
- For the study of pathogenesis, immune response, and epidemiology of viral diseases
- For the study of oncogenesis.
Monkeys: Monkeys were used for the isolation of the poliovirus but find only limited application in virology due to their cost and risk to handlers.
Mice: The use of white mice, pioneered by Theiler (1903) extended the scope of animal inoculation greatly. Infant (suckling) mice are very susceptible to coxsackie and arboviruses, many of which do not grow in any other system.
Mice may be inoculated by several routes— intracerebral, subcutaneous, intraperitoneal, or intranasal. The growth of the virus in inoculated animals may be indicated by death, disease, or visible lesions. The viruses are identified by testing for neutralization of their pathogenicity for animals, by standard antiviral sera.
2. EmbrYonated Eggs: The embryonated hen’s egg was first used for the cultivation of viruses by Goodpasture (1931) and the method was further developed by Burnet. The embryonated egg (8-11 day old) are inoculated by several routes for the cultivation of viruses such as chorioallantoic membrane (CAM), allantoic cavity, amniotic cavity, and yolk sac. After being inoculated, eggs are incubated for 2-9 days.
3. Tissue Culture: Three types of tissue cultures are available
- Organ Culture: Small bits of organs can be maintained in vitro for days and weeks, preserving their original architecture and function. Organ cultures are useful for the isolation of some viruses which appear to be highly specialized parasites of certain organs. For example, the tracheal ring organ culture is employed for the isolation of coronavirus, a respiratory pathogen.
- Explant Culture: Fragments of minced tissue can be grown as ‘explant’ embedded in plasma clots and was originally known as ‘tissue culture’. This method is now seldom employed in virology. Adenoid tissue explant cultures were used for the isolation of adenoviruses.
- Cell Cultures: This is the type of culture routinely employed for growing viruses. Tissues are dissociated into the component cells by the action of proteolytic enzymes such as trypsin and mechanical shaking. The cells are washed, counted and suspended in a growth medium. Such media will enable most cell types to multiply with a division time of 24-48 hours.
“Success rate of interventions using modern pathogen techniques: FAQ”
Question 37. Classification of viruses.
Answer:
Classification Of Viruses: Viruses began to be classified into groups based on their physicochemical and structural features from the early 1950s. Nomenclature and classification are now the official responsibility of the International Committee on Taxonomy of Viruses.
Main Criteria Used for the Classification of Viruses:
- Type of nucleic acid: Viruses are classified into two main divisions depending on the type of nucleic acid they possess: riboviruses are those containing RNA and deoxyriboviruses are those containing DNA.
- Number of strands of nucleic acid: Single- or double-stranded, linear, circular, circular with breaks, segmented.
- The polarity of the viral genome: RNA viruses in which the viral genome can be used directly as messenger RNA are by convention termed ‘positive-stranded’ and those for which a transcript has first to be made are termed ‘negative-stranded
- The symmetry of the nucleocapsid.
- The presence or absence of a lipid envelope
Leave a Reply