Gastroesophageal Reflux Disease (GERD): Causes, Symptoms & Treatment
Question. Write a short note on gastroesophageal reflux disease.
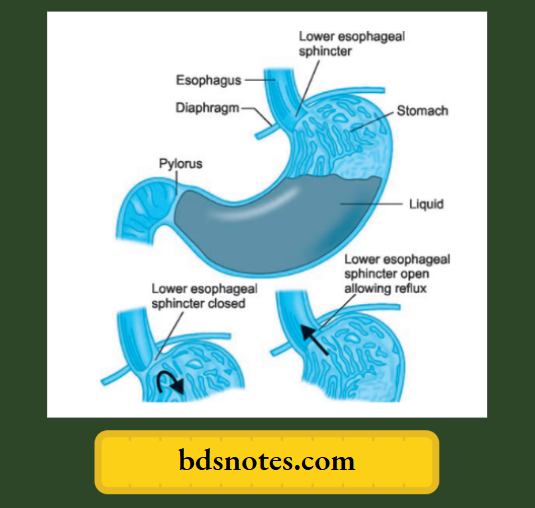
Answer. A chronic condition in which the lower esophageal sphincter allows gastric acids to reflux into the esophagus, causing heartburn, acid indigestion, and possible injury to the esophageal lining.
Mechanism
“Understanding GERD through FAQs: Causes, symptoms, and treatments explained”
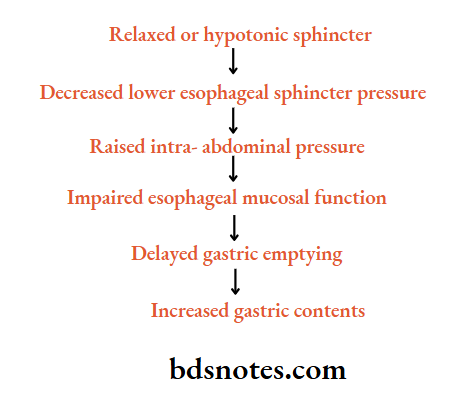
Etiology of gastroesophageal reflux disease
- Relaxed or hypotonic sphincter: It is due to diabetes mellitus, hiatus hernia, and fatty meal.
- Decreased lower esophageal sphincter pressure: This is due to prolonged gastric tube intubation, scleroderma, and the use of certain drugs such as calcium channel blockers, and nitrates.
- Raised intra-abdominal pressure: It is due to ascites, obesity, and pregnancy.
- Impaired esophageal mucosal function: It is due to the usage of alcohol and smoking.
- Delayed gastric emptying: This is due to pyloric obstruction, fatty foods, and gastroparesis.
- Increased gastric contents: It is due to large meals and ZollingerEllison syndrome.
- Sliding hiatus hernia: Where the esophagogastric junction slides up through the diaphragm resulting in:
- Loss of the obliquity of entry of the esophagus into the stomach.
- Loss of the reinforcing effect of intraabdominal pressure on the lower oesophageal sphincter.
“Importance of studying GERD for healthcare professionals: Questions explained”
These two above-mentioned factors of hiatus hernia facilitate gastroesophageal reflux but do not directly cause it.
- Cardiomyotomy and vagotomy: They decrease the efficiency of the lower esophageal sphincter.
Increased intra-abdominal pressure: Pregnancy, obesity, ascites, weightlifting, and straining increase intra-abdominal pressure. - Reduced tone of lower esophageal sphincter: Cigarette smoking, alcohol, fatty foods, and caffeine act by reducing the lower oesophageal sphincter tone.
- Impaired gastric emptying: Impaired gastric emptying due to obstruction of gastric outlet or use of anticholinergic drugs, fatty foods, and large-volume meals acts by increasing the gastric content available for reflux.
- Systemic sclerosis.
- Drugs that reduce the lower esophageal sphincter tone, e.g. aminophylline, betaagonists, nitrates, calcium channel blockers, etc.
Clinical Features of gastroesophageal reflux
- Typical symptoms: Heartburn and acid regurgitation
- Atypical symptoms: Dysphagia, Globus sensation, noncardiac chest pain, dyspepsia, or abdominal pain.
- Extra-esophageal symptoms: Hoarseness, sore throat, sinusitis, otitis media, chronic cough, laryngitis, dental erosion, and recurrent aspiration.
- Malignancy: Head and neck cancer, esophageal adenocarcinoma
“Common challenges in managing GERD effectively: FAQs provided”
Complications of gastroesophageal reflex
- Esophagitis
- Esophageal strictures
- Esophageal ulcers
- Aspiration pneumonia
- Iron deficiency anemia
- Barretts esophagus
- Carcinoma of esophagus
Investigations of gastroesophageal reflex
- Endoscopy: Enables visualization of esophagitis, strictures, and Barrett’s mucosa which all can be confirmed by biopsy.
- Barium meal can reveal a hiatus hernia.
- Bernstein test is done in patients with high clinical suspicion but with negative endoscopy.
- Resting ECG and stress ECG to rule out ischemic heart disease.
- Esophageal motility studies.
Management of gastroesophageal reflux
1. Conservative measures:
“Role of hiatal hernia in causing GERD: Questions answered”
“Why is early detection critical for preventing GERD complications? Answered”
- Abstain from eating within 2 hrs of bedtime
- Elevate the head of the bed by 6 inches
- Sleep in the left lateral decubitus position
- Avoid: Caffeine, nicotine, alcohol, chocolate, mints, carbonated beverages, highfat foods, tomato or citrus-based products
- Avoid if possible medications that can worsen GERD anticholinergic, theophylline, prostaglandin, calcium channel blockers, alendronate
- Weight loss if obese
- Rabeprazole and esomeprazole provide superior gastric acid suppression.
“Steps to explain GERD: Causes vs symptoms vs treatment: Q&A guide”
2. Medical treatment of gastroesophageal reflux
- In mild cases liquid antacid is used, i.e. 10 to 15 mL, one to three hours after the meal which provides relief from heartburn.
- In moderate cases, H 2 receptor antagonist, i.e. ranitidine 150 mg BD or QID with meals and before bedtime for 6 weeks.
- In severe cases, proton pump inhibitors are given, i.e. omeprazole 20 to 40 mg/day, pantoprazole 40mg/day, and rabeprazole 10 to 20 mg/day is given.
These should be given for 6 to 8 weeks.
For maintenance therapy treatment should be given for 6 to 8 months. - Metoclopramide or domperidone 10 mg TID increases lower esophageal sphincter tone and promotes gastric emptying.
- Repeated dilatations are used to treat esophageal strictures.
- In anemics oral iron or blood transfusion is given.
“Factors influencing success with GERD knowledge: Q&A”
3. Surgical treatment of gastroesophageal reflux
- Surgical resection of strictures should be carried out.
- Surgical return of lower esophageal sphincter to the abdomen in a patient with sliding hiatus hernia, construction of an additional valve mechanism is done.
Leave a Reply