Tuberculosis
Tuberculosis is a infectious granulomatous disease caused by Mycobacterium tuberculosis.
Tuberculosis Pathogenesis
“Importance Of Early Detection Of Tuberculosis”
Tuberculosis Clinical Features
- Patient suffers from episodic fever and chills, easy fatigability and malaise.
- There is gradual loss of weight with persistent cough with or without hemoptysis.
- Choroid tubercles are seen in children.
- Lupus vulgaris may occur in children.
cervicofacial actinomycosis
Tuberculosis Oral Manifestation
- Tongue is the most common site involved followed by palate, lips, buccal mucosa, gingiva and frenula.
- There is presence of irregular, superfiial or deep ulcer which is painful and will increase in size.
- There is presence of diffse hyperemic, nodular or papillary proliferation of gingival tissues.
- Tuberculous osteomyelitis occurs in the later stages of disease.
oral actinomycosis
“Early Signs Of Tuberculosis Infection”
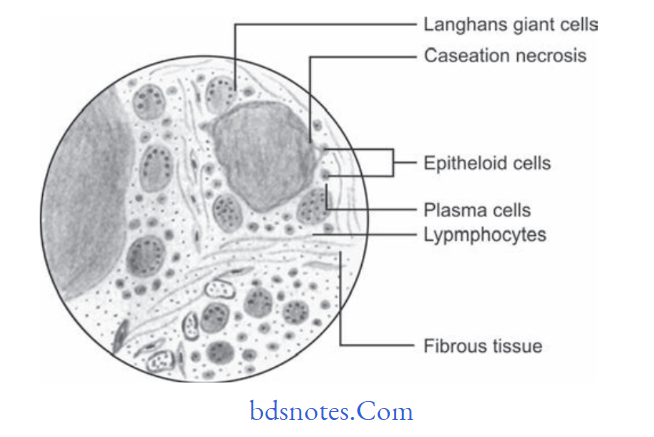
Tuberculosis Histological Features
There is formation of granuloma exhibiting, foci of caseous necrosis surrounded by epithelioid cells, lymphocyte and occasionally multinucleated giant cells.
- Epithelioid cells are morphologically altered macrophages and appear like epithelial cells.
- Multinucleated giant cells are of LanghAns type.
- Area of caseous necrosis appears eosinophilic.
- Granuloma is surrounded by firous tissue and lymphocytes. At times dystrophic
- calcifiation is seen.
“Role Of The Bcg Vaccine In Preventing Tuberculosis”
Tuberculosis Treatment
Multidrug therapy (MDT) is recommended.
Oral Manifestations of Tuberculosis
Following are the oral manifestations of tuberculosis:
Tuberculous infection in oral cavity may produce nodules, vesicles, fissures, plaque, granulomas or verrucal papillary lesions.
- Tuberculous lesions of oral cavity are tuberculous ulcers, tuberculous gingivitis and tuberculosis of salivary gland.
- Tongue is most common location for the occurrence,besides this palate, gingiva, lips, buccal mucosa,alveolar ridge and vestibules may also be affcted.
- Tongue lesion: Tuberculous lesion of tongue develops on the lateral borders and appears as single or multiple ulcers which are well defied, painful and fim in consistency. Ulcers are deep and are painful.
Margins of ulcer are undermined with no induration.
Area surrounding the ulcer remains inflmed and edematous. Base of the ulcer is yellowish.
“Understanding The Role Of Mycobacterium Tuberculosis In Tb”
- Lip lesions: Lesions produce small, nontender, granulating ulcer at mucocutaneous junction.
Gingival lesions: These lesions produce small granulating ulcers. Gingiva appear diffuse, hyperemic and nodular papillary proliferation is seen. - Tuberculous lesion of jaw bone: Chronic Osteomyelitis of maxilla and mandible may occur and infection reaches to bone via blood or root canal or extraction socket. Tuberculous osteomyelitis of jaw bone produces pain, swelling, sinus or fitula formation. As jaw bone is involved patient complains of swelling and diffilty in eating.
- Miliary lesion of oral mucosa in military tuberculosis is a small grey colored tubercle which breakdown and ulcerate.
- Periapical tissue can also be involved by the tubercle.
Tooth socket is filed with tuberculous granulation tissue and has small pink and red elevations.
“Step-By-Step Guide To Diagnosing Tuberculosis Effectively”
Question.10. Write short note on pathogenesis of tuberculosis.
Answer. Following is the pathogenesis of tuberculosis:
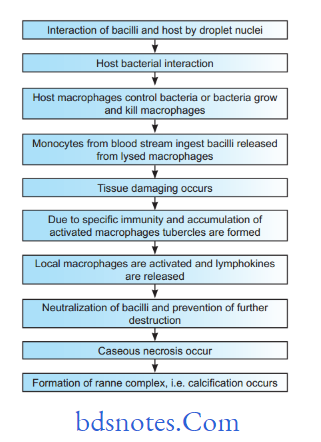
Pathogenesis Of Tuberculosis
- The interaction of the bacilli and the host begins when droplet nuclei from infectious patients are inhaled.
- The majority of the bacilli are trapped and exhaled by ciliary action and a fraction less than 10% enters alveoli.
- In the initial stage of the hostbacterial interaction, either host’s macrophages control the multiplication of the bacteria or the bacteria grow and kill the macrophages.
- Non-activated monocytes attacted from bloodstream to the site by various chemotactic factors ingest the bacilli released from the lysed macrophages.
- Initial stages are asymptomatic; about 2-4 weeks after infection tissue damaging and macrophage activating responses develop.
- With the development of specifi immunity and accumulation of a large number of activated macrophages at the site of primary lesion, granulomatous reaction or tubercles are formed.
“Comprehensive Overview Of Tuberculosis And Its Global Significance”
- The hard tubercle consists of epithelioid cells, LanghAns giant cells, plasma cells, and firoblasts. These lesions develop when host resistance is high.
- Due to cellmediated immunity in the majority of individuals, local macrophages are activated and lymphokines are released, which neutralize the bacilli and prevent further tissue destruction.
- The central part of the lesion contains caseous, soft, and cheesy necrotic material (caseous necrosis). This necrotic material may undergo calcification at a later stage called Ranne complex, in the lung parenchyma and hilar lymph nodes in few cases.
- Caseous necrotic material under goes liquefaction and discharges into the lungs leading to the formation of a cavity. Spontaneous healing of the cavity occurs either by firosis or collapse.
- Calcification of the cavities may occur in which bacteria persist.
- In early stages, the spread of infection is mainly by macrophages to lymph nodes, other tissues, and organs.
However, in children with poor immunity hematogenous spread results in fatal miliary TB or tuberculous meningitis.
“The Role Of Chest X-Rays In Diagnosing Tuberculosis Infections”
Question.11. Enumerate bacterial lesion involving oral cavity. Describe clinical features, investigations, histopathology and management of tuberculosis.
Answer.
Enumeration Of Bacterial Lesions Involving Oral Cavity
- Syphilis
- Nonvenereal treponematoses
- Gonorrhea
- Streptococcal tonsillitis and pharyngitis
- Leprosy
- Tuberculosis
- Actinomycosis
- Noma
- Scarlet fever
- Diphtheria
- Cat scratch disease
- Tularemia
- Tetanus
- Rhinoscleroma
- Botryomycosis
- Melioidosis
- Granuloma Inguinale
- Lymphogranuloma venereum
- Myiasis.
Investigations
- Serology: In this ELISA technique is used which helpful in diagnosis of tuberculosis in children. PCR technique is more specifi and sensitive serological test than ELISA,but PCR is less used due to its high cost.
- Chest X-ray: Presence of multiple nodular infiltrations or ill-defied opacities in one of upper lobes is characteristic for pulmonary tuberculosis.
An area of translucency in radiopacities is indicative of cavitation. Presence of cavity is indicative of an active lesion.
In some of the patients, multiple thickwalled cavities can be seen. At the time of firosis, trachea and mediastinum shift to same side.
Fibrosis can also cause calcification. - Pathological tests:
- Blood examination: Peripheral blood examination shows monocytosis, i.e. 8 to 12%
- ESR is elevated.
- Tuberculin test: It is a test to recognize prior tubercular infection, and is done by injecting one unit of purifid protein derivative (PPD) on the forearm and readings taken after 48 hours. Induration of more than l5 mm indicates a positive test.
The younger is the patient, greater is signifiance of positive test.
A negative test does not always exclude tubercular infection since it may be negative in patients of blood malignancies, malnourishment and those on immunosuppressive therapy.
Tuberculin test is nonspecific and only indicates prior infection. Its sensitivity wanes with age.
Management
Chemotherapy.
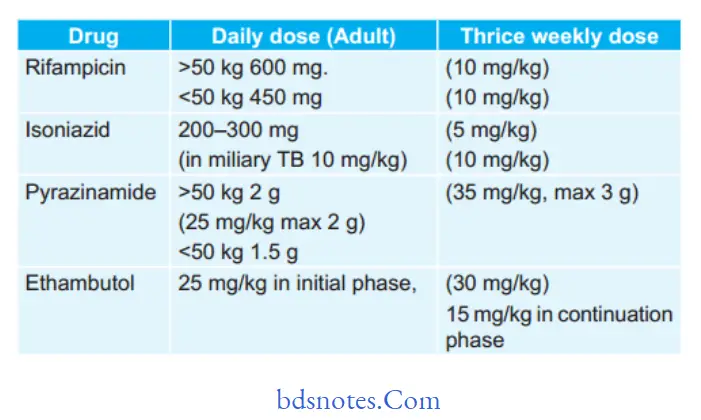
Drugs for primary Chemotherapy
(First Line Anti-Tubercular Drugs)
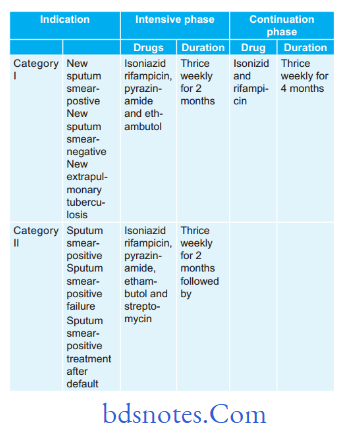
Under Dots following treatment regimen is used
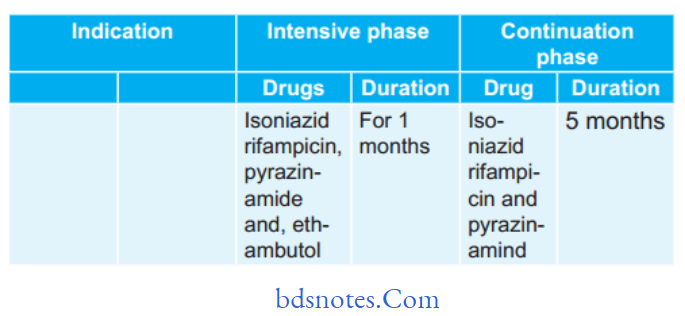
Second-line anti-tuberculous Drugs
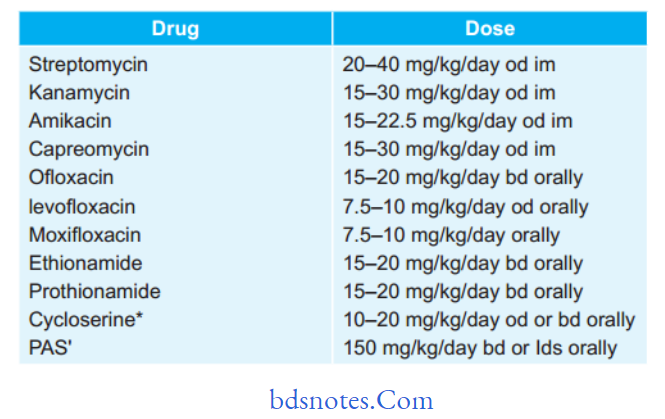
“Best Practices For Managing Tuberculosis Symptoms Safely”
Treatment regimen under rNTCP for MDr-TB (Multi- drug-resistant TB) and XDr-TB (Extensively drug-resistant TB)
- For MDR-TB:
- Six drugs in intensive phase for 6–9 months: Kanamycin,levoflxacin, ethionamide, cycloserine, pyrazinamide and ethambutol.
- Four drugs in continuation phase for 18 months:
Levofloxacin, ethionamide, cycloserine and ethambutol. - Reserve drug is paminosalicylic acid.
- For XDR-TB:
- Seven drugs in intensive phase for 612 months:
Capreomycin, p-aminosalicylic acid, moxiflxacin,high dose isoniazid, clofazimine, linezolid, Amoxicillin and clavulanic acid. - Six drugs in continuation phase for 18 months:
paminosalicylic acid, moxifloxacin, high dose lsoniazid, clofazimine, linezolid, amoxicillin and clavulanic acid.
Reserve drugs: Clarithromycin, thiacetazone
- Seven drugs in intensive phase for 612 months:
- Corticosteroids: They are to be given in the severe cases to enable them to survive till antitubercular drugs become effctive. Oral prednisolone is given in doses of 20 mg orally for 6 to 8 weeks. Steroids produce euphoria and increase appetite in the patients.
- Surgery: Surgical resection of infected lobe is feasible.
- Symptomatic treatment:
- Cough: If it is irritative, linctus codeine is given.
Smoking should be stopped - Laryngitis: Rest is given to the voice. If pain is present
anesthetic powders, spray and lozenges are given.
- Cough: If it is irritative, linctus codeine is given.
Leave a Reply