Leukoplakia in Oral Pathology – From White Patches to Cancer Risk
Write a short note on leukoplakia.
Answer:
Leukoplakia is defined as a predominantly white lesion of the oral mucosa that cannot be characterized as any other defiable lesion. WHO (1997)
Leukoplakia should be used to recognize white plaques of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer. Warnakulasuriya et al (2008)
“Understanding the role of leukoplakia in oral pathology”
Leukoplakia Etiology
- Tobacco: It is used by a large number of people in various forms such as smoking cigarettes, cigars, biddies and pipes.
- All these types of tobacco habits are important for the development of leukoplakia.
- It is believed that during smoking a large amount of tobacco end products are produced in the oral cavity.
- The products in association with heat cause severe irritation to the oral mucus membrane and finally result in the development of leukoplakia.
- Alcohol: Many people develop leukoplakia that consume alcohol leukoplakia as well as use tobacco in some form.
“Importance of studying leukoplakia for better oral health outcomes”
“Common challenges in diagnosing and managing leukoplakia”
- Candidiasis: Chronic candidal infections are associated with leukoplakia.
- Dietary Deficiency: A deficiency of vitamin A causes metaplasia and hyperkeratinization of epithelium which may result in the development of leukoplakia.
- Syphilis: Syphilitic infections play a minor role in the causation of leukoplakia.
- Hormonal imbalance: Imbalance or dysfunction of both male and female sex hormones causes keratinogenic changes in the oral epithelium.
- These changes lead to the development of leukoplakia.
“Factors influencing the development and progression of leukoplakia”
Read And Learn More: Pathology Questions And Answers
Leukoplakia Gross Features
- Lesions of leukoplakia appear white or whitish-yellow or red velvety of more than 5 mm diameter and are variable in appearance.
- Lesions are circumscribed, slightly elevated, smooth or wrinkled, speckled, or nodular.
“Steps to identify clinical features of leukoplakia in oral pathology”
Leukoplakia Histologically
Leukoplakia is of two types, i.e.
- Hyperkeratotic type: It is characterized by orderly and regular hyperplasia of squamous epithelium with hyperkeratosis on the surface.
- Dysplastic type:
- When cellular changes such as loss of stratification of epithelium, focal areas of increased and abnormal mitotic figures, hyperchromatism, pleomorphism, loss of polarity, and individual cell keratinization lesion are considered epithelial dysplasia.
- Mild dysplasia reverts back to normal offending etiologic factor is removed whereas severe dysplasia is indicative of progression into carcinoma.
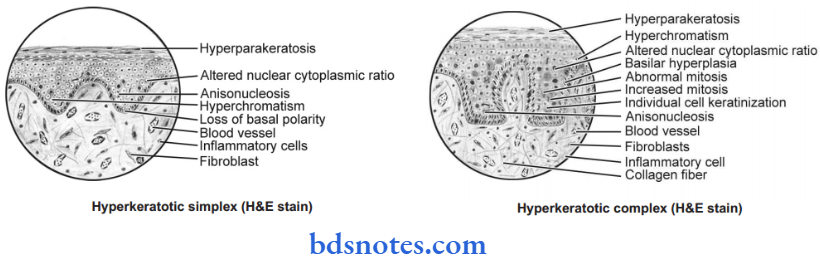
- Histologically, leukoplakia is expressed as a hyperkeratotic simplex and hyperkeratotic complex.
“Role of white patches in diagnosing leukoplakia”
- Hyperkeratoic simplex denotes mild leukoplakia and the chances of its malignant transformation are less while hyperkeratotic complex denotes severe leukoplakia and the chances of its malignant transformation are high.
- In leukoplakia there is often a variable degree of destruction of collagen fibers and moreover, chronic inflammatory cell infiltrate is also present in underlying connective tissue stroma.
“Asymptomatic vs symptomatic stages of leukoplakia progression”
Leave a Reply